
Abstract
Background:
There are not many clinical trials investigating the efficiency and compliance of using spinal orthoses in the management of osteoporosis.
Objectives:
The purpose of this study was to investigate the effect of long-term use and the compliance of spinal orthoses in postmenopausal women with vertebral fractures.
Study design:
Clinical trial of spinal orthoses in postmenopausal women.
Methods:
Women were separated into groups wearing different types of orthoses (Spinomed, Osteomed, Spinomed active, and Spine-X). Isometric maximum strength of trunk muscles (F/Wabdominals–extensors) was calculated and back pain was assessed in all women. In addition, women completed a compliance questionnaire about the use of the orthoses.
Results:
Spinomed decreased pain (p = 0.001) and increased trunk muscle strength (F/Wabdominals, p = 0.005 and F/Wextensors, p = 0.003, respectively). The compliance of wearing an orthosis for 6 months was 66%.
Conclusion:
The results suggest that orthoses could be an effective intervention for back pain and muscle strengthening in osteoporotic women.
Clinical relevance
In women with established osteoporosis, wearing Spinomed orthosis for at least 2 h/day for 6 months decreased back pain significantly and increased personal isometric trunk muscle strength. All spinal orthoses could be valuable instruments to help all requested rehabilitation programs like spine muscles’ strengthening and postural correct behavior, but only when used properly.
Background
Spinal orthoses have been used in the management of thoracolumbar injuries treated with or without surgical stabilization. These orthoses, however, have never been tested under standardized conditions. Especially, no prospective, randomized, and controlled clinical trials are available to document efficacy according to the criteria of evidence-based medicine. 1 Moreover, there is a lack of specific studies comparing various types of braces and orthoses. Even though it is widely accepted that spinal orthoses whether made of cloth, metal, or plastic, or whether rigid or flexible, relieve pain and promote the healing process by stabilizing the spine, that is, reducing the load applied on the anterior column and vertebral body by restraining any attempt of forward flexion. 2
Considering the body mechanics, the load of the spine is transferred by the vertebral body. But there are also other structures, that is, muscles, ligaments, and so on, in the region playing a regulatory role. In a kyphotic posture, the spinal kyphosis causes a forward and downward shift of the center of mass of the trunk in the sagittal plane. To maintain balance, the subject has to correct for this shift. This is impossible for some osteoporotic women because of muscle weakness. Anterior column fails resulting in compression while posterior column fails resulting in tension. 3
The most broadly used types of spinal orthoses utilize a three-point pressure system. 4 Different types of spinal orthoses are briefly discussed in the following:
The TLSO type (Knight–Taylor, Jewett, or cruciform anterior sternal hyperextension (CASH) brace, Boston): it provides support to the thoracolumbosacral spine. The CASH or Jewett brace has been favored for patients with acute thoracolumbar vertebral fractures. The goal of these braces is to provide forces to encourage hyperextension. 5 However, a drawback to these orthoses in the treatment of compression fractures in osteoporotic elderly patients is controversial because it can exert excessive hyperextension forces on the lower lumbar vertebrae, which in turn can induce posterior element fractures or exacerbate a degenerative arthritis condition. 6
The Posture Training Support (PTS) type, or the newer postural training support vest with weights (PTSW): these two orthoses are made of a softer material, gained popularity because of their improved comfort and increased compliance. The postural training support is worn over the shoulders similar to a mini-backpack and has a pocket into which small weights (total 1.75 lb) are added. The PTSW is similar to this type of orthosis except that it is fashioned as a vest with a Velcro attachment that fastens around the abdomen. 7
Spinomed and Spinomed active: these are based on biofeedback theory.1,8 Spinomed consists of an abdominal pad, splint along the spine, back pad, and a system of belts with Velcro. The back orthosis consists of a back pad that is workable as a cold material and a system of belts with Velcro. This allows adjustments for individual sizes by an orthopedic technician. The orthosis weighs 450 g and is worn like a back pad.
Osteomed: it is based on the gate control theory of pain. The external appearance of the orthosis Osteomed resembles an item of clothing characterized by a constructively functional cut with Velcro tabs exerting pressure on the lumbosacral region. The air chamber pads, fixed in the paravertebral and lumbosacral areas, are filled with air to between 2/3 and 3/4 of their maximum capacity. 9
The most widely held viewpoint is that the manual muscle strength is basically an attempt to assess the maximum force a muscle can generate. 10 In our view, the manual muscle testing is particularly suitable in the rehabilitation phase when muscles or muscle groups with a lack of contraction to weak muscles or muscle groups are examined. However, the manual muscle testing method that primarily measures force in the final stages of rehabilitation or in subjects with muscular fitness appears unsuitable to identify deficiencies and imbalances. For these reasons, the use of a precise and apparatus-based device having diagnostic power is recommended. The extension of classic muscle function test on the maximum isometric force capability takes into account that it is not individual muscles but functional groups of muscles are to be examined. The functionality of the muscle groups is based on the respective joints that are associated with different patterns of movement, such as flexion and extension of the trunk. The purpose of this study was to investigate the effect of long-term use of modern spinal orthoses (semi-rigid and elastic) to alleviate back pain by exerting force on the trunk (extensors–abdominal) muscles in postmenopausal women with vertebral fractures in thoracic and lumbar spine and the compliance with the use of such spinal orthoses.
Methods
Fifty socially active women aged above 60 years, referred to the University from various departments for routine osteoporosis examinations, were enrolled in this study. Study entry criteria were as follows: established spinal osteoporosis defined by the presence of at least one vertebral fracture in the thoracic or lumbar spine not caused by serious injury or accident, radiographic (x-ray) evidence of morphometry-based fracture of the vertebra with a reduction in vertebral height of at least 20%, and women with a kyphosis angle more than 55° measured in lateral view x-ray of dorsal spine. The standard (Cobb) measuring technique for the quantification of thoracic kyphosis was used, which has the advantage of being part of a global non-invasive postural evaluation, although the precision of the resulting measurement is not very high.11,12 All measurements were performed by the same physiatrist (Y.D.) Women with disorders affecting bone metabolism (hyperthyroidism, primary hyperparathyroidism, and osteomalacia) and also women with serious degenerative diseases such as severe osteoarthritis, scoliosis, and tumors were excluded. Causes of secondary osteoporosis were excluded from the history and biochemical tests of serum blood and urine. We adopted our inclusion and exclusion criteria from the study of Pfeifer et al. 7 Their study introduced the thoracolumbar orthosis Spinomed (Medi Bayreuth, Bayreuth, Germany) in a scientific evidence-based manner. Our purpose was to repeat a clinical trial using similar methods but various orthoses in order to determine generalizability. This was planned as a randomized clinical trial prospective study to be completed in 6 months. Women were separated into group A (n = 20, using semi-rigid orthosis Spinomed or Spine-X), group B (n = 20, using elastic multifunctional orthosis Osteomed, Spinomed active), and the control group (n = 10), which included women of similar age with fractures.
Women were referred to our department with their own orthosis (bought with their own expenses) as prescribed by their physician. All were ready made not custom handmade orthoses, according to subjects’ size and shape. After trying the orthosis, a qualified technician adjusted and modified the device to ensure a perfect fit. All orthoses used during this study were manufactured abroad (in Germany) and imported. Women were assigned in groups immediately (according to the prescribed orthosis) after screening by the physiatrist (Y.D.) to determine whether they met the inclusion criteria. As controls, women who denied wearing the prescribed orthosis were enrolled. Participants were required to wear the provided orthosis at least 2 h/day and keep a dairy (proof of compliance to treatment).
All participants received various medications for osteoporosis including calcium and vitamin D. All were recruited from various departments around Athens (Rehabilitation, Orthopaedic, and Rheumatology Departments) after announcement for participation in a clinical research of Athens University. The protocol was designed according to the Declaration of Helsinki, and all subjects agreed to take part voluntarily. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Measurements and questionnaires
Anthropometric values of height and weight of the subjects were measured in standing position. Weight, W (kg) was recorded on Leonardo™ Mechanography Ground Reaction Force Platform (Novotec Medical GmbH, Pforzheim, Germany). This system measures forces, F (N) applied to the plate over time including stationary forces. Height (m) was measured with a wall-mounted ruler. Body mass index (BMI) was also calculated for each subject (BMI = weight (kg)/height 2 (m)).
We calculated the maximum personal isometric strength of trunk muscles (Force/Weightabdominals and Force/Weightextensors) in a seated position with knees and hips bent at 90° with the system Digimax ISO-Rack (Digimax Systems, Hamm, Germany). This system is a low-cost versatile isometric measuring station. The basis of the automated supplement is a digital, microprocessor-controlled instrument from Digimax Systems. The meter consists first of a force sensor, which operates on the basis of strain gauges, and the other composed of a display unit in the form of a handheld device, which is also equipped with an interface to the PC. We used a lower filtering setting for acquired signals from ISO-Rack to ensure harmonious and more accurate curves with the cut-off frequency of 5 (filter interval) according to the manufacturer’s instructions. For an optimal reproduction of the measurement situation, there are numbers printed across the Rack and on the surface of a floor mat. This floor mat is completed in a chest-type pattern with reference numbers and stands in the floor beside the Rack device (Figure 1). The average force from three trials was recorded. The maximum strength in each trial was measured, and these values showed high reproducibility (r = 0.990, p < 0.0001). All subjects were assessed by the same (Y.D.) examiner. The coefficients of variance were 2.5% for back extensor strength and 2.33% for abdominal flexor strength. More details for the methodology of the measurement can be found here. 13
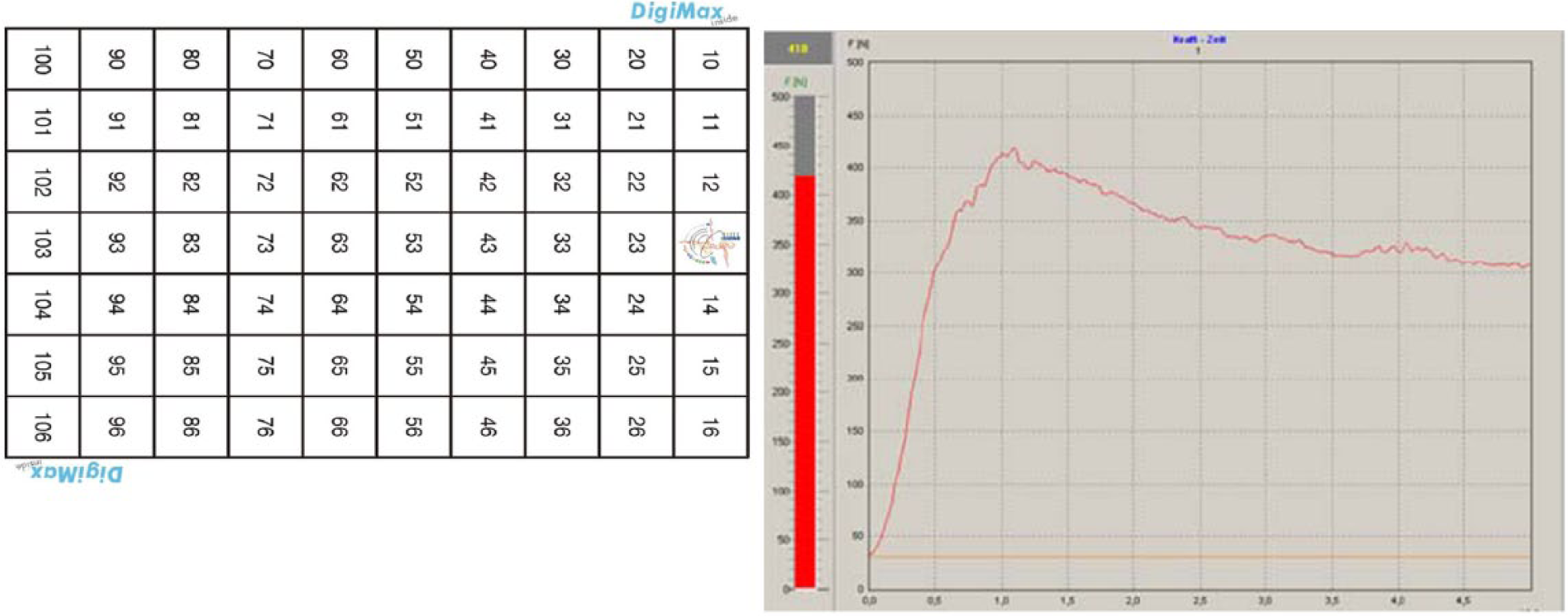
Digimax ISO-Rack (Digimax Systems, Hamm, Germany) system is a low-cost versatile isometric measuring station. The basis of the automated supplement is a digital, microprocessor-controlled instrument from Digimax Systems. The meter consists first of a force sensor, which operates on the basis of strain gauges, and the other composed of a display unit in the form of a handheld device, which is also equipped with an interface to the PC. For an optimal reproduction of the measurement situation, there are numbers printed across the Rack and on the surface of a floor mat. This floor mat is completed in a chest-type pattern with reference numbers and stands in the floor beside the Rack device.
We assessed back pain with Visual Analog Scale (VAS) translated in Greek (Figure 2). The VAS is continuous, independent of language, and it measures the intensity of pain where “no pain” scores 0 and “pain as bad as it could be” or “worst imaginable pain” scores 10. The VAS score was measured from assigning marks on VAS from none to severe and was calculated by the equation: (distance of marking from the left end of the line/total length of the line) × 100%. A higher percentage indicates a greater problem encountered by the subjects in using the orthosis.14,15
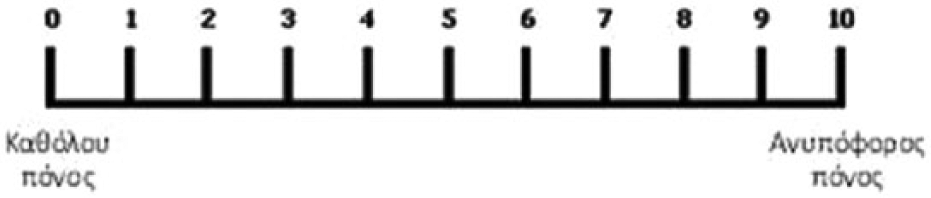
Greek version of VAS.
In addition, women completed a compliance feedback questionnaire designed for this study (in Greek language) developed by Y.D. and translated in English. The questionnaire was back translated by S.T. (who is an English-certified M.D.) to check the accuracy of the original translation. Validity of the draft questionnaire was established using a panel of experts and a field test. All questions were coupled with readability test and approval from the Institutional Review Board (IRB) was also obtained after the pilot study that was carried out in Athens University (scientific research program “Kapodistrias”). Reliability was established using a pilot test with 20 subjects not included in the sample. Data collected from pilot test were analyzed using Statistical Package for Social Sciences (SPSS). SPSS provided a reliability coefficient (alpha) of 0.80.
The surveys were carried out in the 1st month, 6th month (interviews), and 4 years of the use of orthoses. Patients were followed via telephone calls to their home to complete the survey after 4 years of the orthotic intervention.
The subjects were requested to answer the following question relating compliance: “How long you are wearing the brace during the day?” Possible answers given by the subjects were as follows: none at all, half an hour, 2 h, and so on.
Statistical analyses
All quantitative data were represented by the number of patients (n), mean value (mean), and standard deviation (SD) and qualitative data by the number of patients (n) and percentage (%). Qualitative variables were analyzed using chi-square (χ 2 ) test and Fisher’s exact test. All tests are two-sided with 95% significance level. Statistical analysis was performed using the SPSS version 12.00. Significance was set at 0.05 level.
Results
In this pilot study, we present anthropometric measurements and variables of force and pain in a subgroup of group A (using Spinomed orthosis) in comparison to a control group C. The effect of wearing different types of orthoses was compared after 6 months between group A and the control group. We checked the effect between Spinomed and Spine-X orthoses. Women of group A (Spinomed) were significantly older, and at the beginning of the study, they felt more pain compared to the control group (72.3 ± 8 vs 61 ± 10.5; p = 0.015 and 65 ± 16.5 vs 45 ± 16.5; p = 0.014). The rest of the anthropometric parameters were identical and there was no significant between groups (as shown in Table 1). Spinomed-wearing subjects had lower strength compared to controls (F/Wabdominals: 176.5 ± 58.5 vs 131.2 ± 53.7, p = 0.088 and F/Wextensors: 218 ± 60 vs197.6 ± 48, p = 0.4). The values of F/Wabdominals and F/Wextensors were reduced by 25% and 10%, respectively, in subjects wearing Spinomed compared to controls. Over a period of 6 months, the use of Spinomed decreased pain as measured with VAS significantly (41 ± 17.3 vs 65 ± 16.5, p = 0.001) in group A (37% decrease) (Figure 4). After 6 months of wearing Spinomed trunk, muscle strength was significantly increased (F/Wabdominals: 197.8 ± 82.7 vs 131.2 ± 53.7, p = 0.005 and F/Wextensors: 246.3 ± 59.5 vs197.6 ± 48, p = 0.003), as depicted in Figure 3.
Anthropometrics and measured variables of the study population.
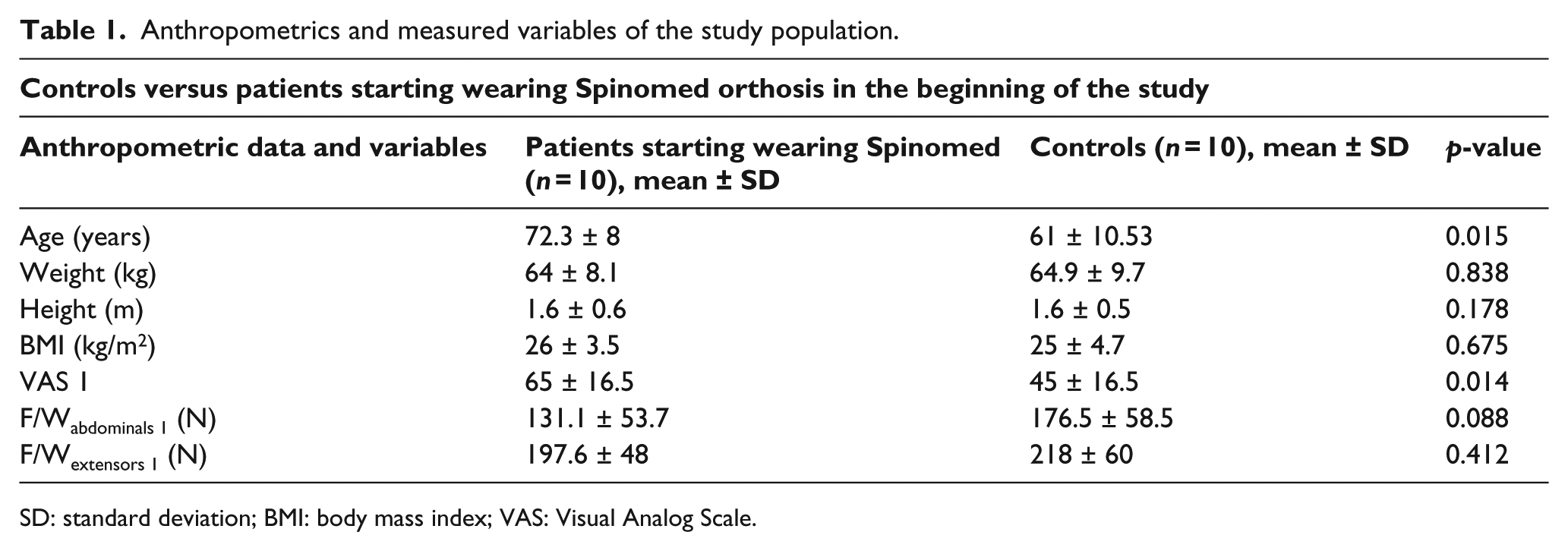
SD: standard deviation; BMI: body mass index; VAS: Visual Analog Scale.
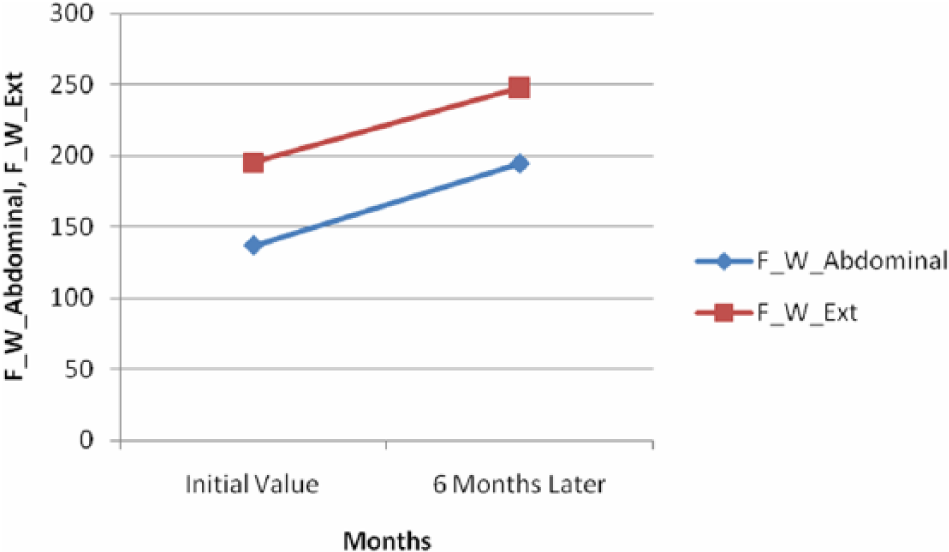
Schematic presentation of differences in the values of personal isometric force: force (F)/weight (W) in abdominal and extensor muscles (F/Wabdominals and F/Wextensors, respectively, after 6 months of wearing Spinomed orthosis (F: force in Newton; W: weight in kilogram), measured with Digimax ISO-Rack (Digimax Systems, Hamm, Germany).
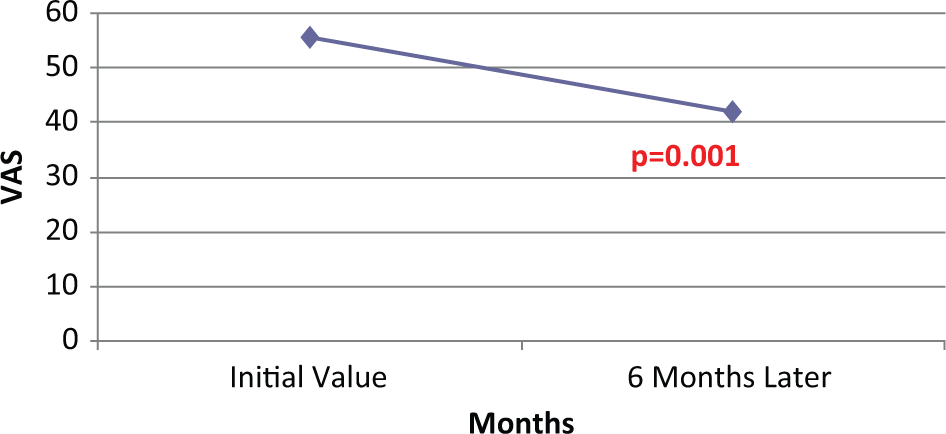
Assessment of back pain with VAS at the beginning of the study and after 6 months of Spinomed wearing.
During this period, subjects wearing Spinomed increased F/Wabdominals and F/Wextensors by 50% and 25%, respectively. Moreover, after 6 months of Spinomed wearing, subjects felt less pain than controls (9% less), and the values of strength in trunk muscles (F/Wabdominals and F/Wextensors) were 12% and 13% higher than the significantly younger controls (as shown in Table 2). We could not perform a statistical analysis of trunk muscle strength in subjects wearing Spine-X orthosis due to lack of data. The results were available for five subjects only at the time of submission, although four subjects wearing Spine-X for 6 months showed increase in their strength and decreased VAS (mean difference VAS 20) (Table 3).
Variables of trunk muscle strength and VAS after 6 months.
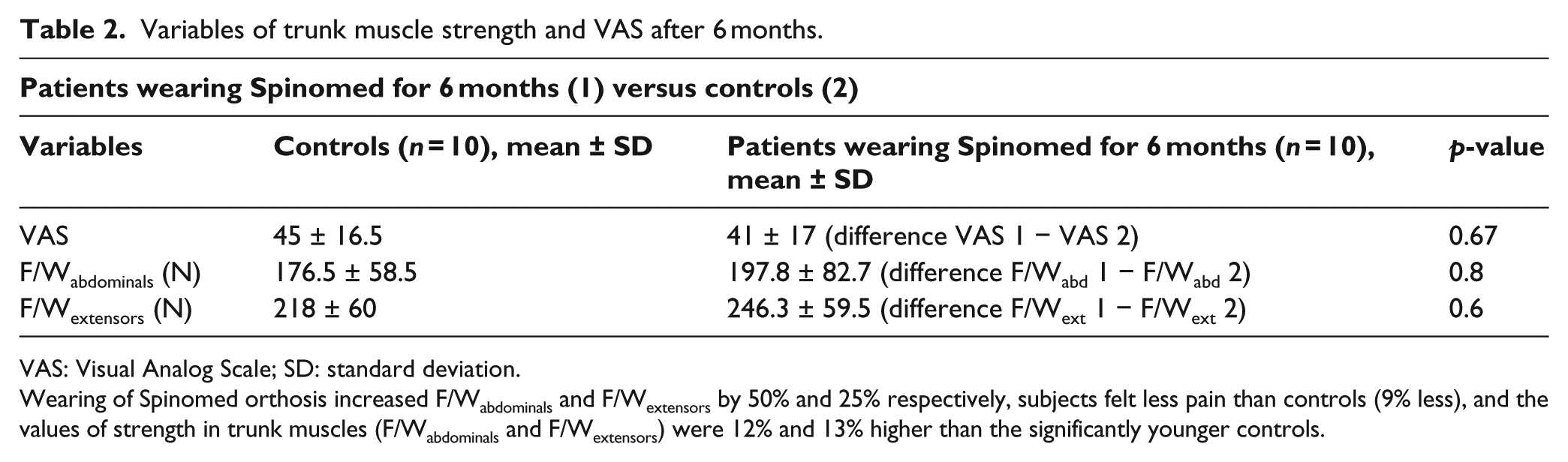
VAS: Visual Analog Scale; SD: standard deviation.
Wearing of Spinomed orthosis increased F/Wabdominals and F/Wextensors by 50% and 25% respectively, subjects felt less pain than controls (9% less), and the values of strength in trunk muscles (F/Wabdominals and F/Wextensors) were 12% and 13% higher than the significantly younger controls.
Anthropometrics, trunk muscle strength variables, VAS, and compliance with Spine-X.
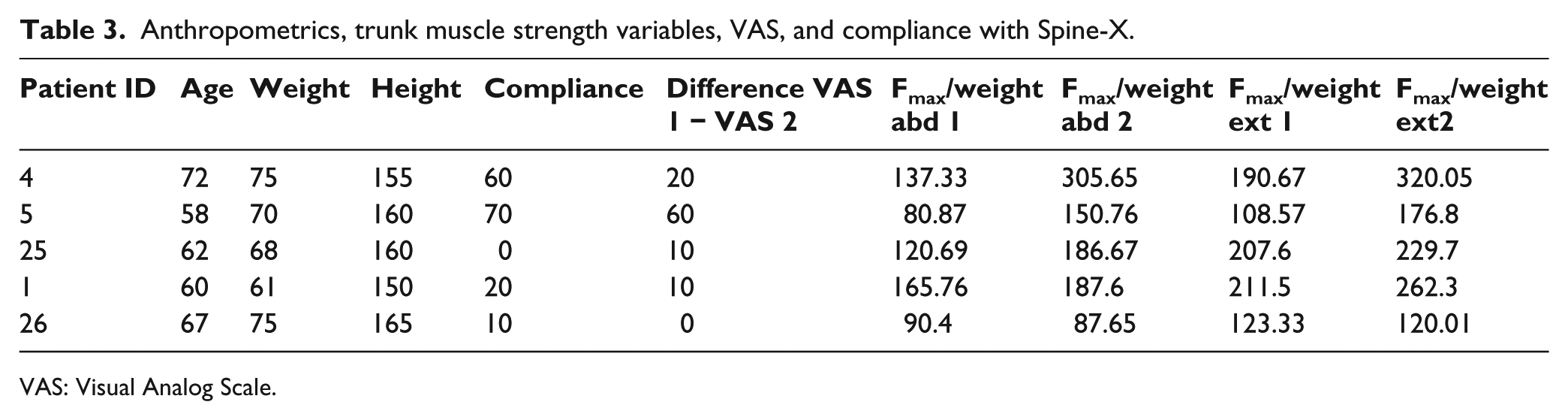
VAS: Visual Analog Scale.
The compliance of wearing an orthosis for 6 months was 66% (Figure 5). The compliance was highest for Spinomed (90%) followed by Osteomed and Spinomed active (50%), while Spine-X showed the lowest compliance of 30%. Lowest compliance as shown by Spine-X and the results of the measured variables are presented in the table.
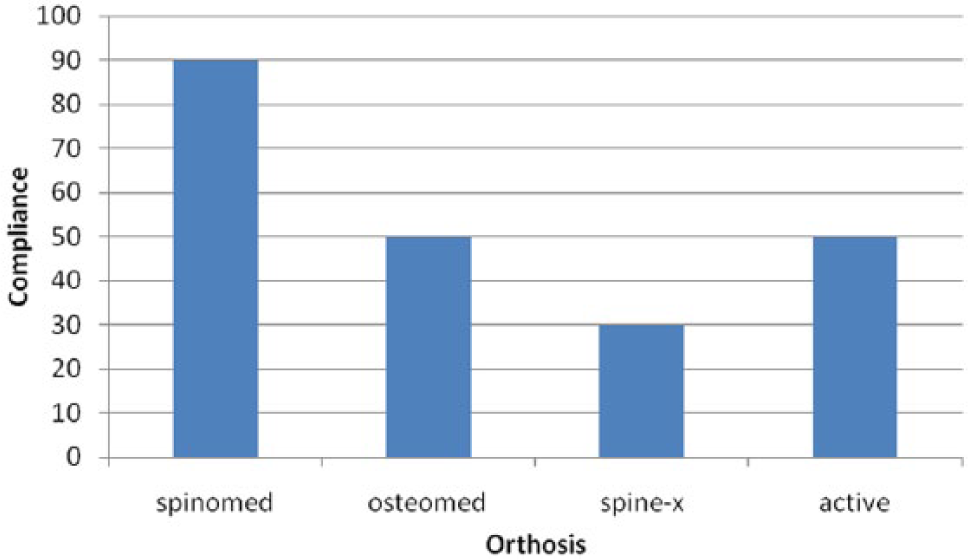
Compliance of each type of orthosis: the compliance was highest for Spinomed (90%) followed by Osteomed and Spinomed active (50%), and finally Spine-X showed the lowest compliance of 30%.
Discussion
Spinomed orthosis decreased back pain significantly in women with established osteoporosis and/or an angle of kyphosis more than 55° who wore the orthosis for at least 2 h/day for 6 months. The orthosis also increased personal isometric trunk muscle strength.
Personal isometric force (F/Wabdominals and F/Wextensors) measurements
According to our results, values of personal isometric force (F/Wabdominals and F/Wextensors) were reduced by 25% and 10%, respectively, in subjects who started wearing Spinomed compared to controls in the beginning of this study. This non-significant difference (only a trend was found in F/Wabdominals between groups) can be explained from the significant difference in age between the groups of Spinomed and controls. Women who started wearing Spinomed were much older compared to women in the control group.
Between the ages of 65 and 90 years, muscle strength is lost with a rate of about 1.8% per year; concentric force development is lost more rapidly than the eccentric variety. In both sexes, there is a little fall-off in strength until about the mid-40s, after which it drops by approximately 25% by the age of 65 years. 16 In women, there may be an accelerated postmenopausal fall-off in strength. 17 Nevertheless, loss in force parameter appears to be partially reversible. For example, Morse et al. 18 investigated the reversibility of the decline in specific force in old age in response to long-term (12 months) resistive loading of males aged over 70 years and found an increase (p = 0.05) in specific force.
After 6 months, in subjects wearing Spinomed, trunk muscle strengths (F/Wabdominals and F/Wextensors) were significantly increased by 50% and 25%, respectively. The values in group A were 12% and 13% higher compared with the younger control group, without any additional exercise programs. Our findings suggest the importance of maintaining good posture in performing daily activities. The use of orthosis corrects the posture activating the body’s own natural muscle power and strengthens the spine. An earlier controlled pilot study with a 4-week observation period found that the strength of the back extensors was reduced to below the initial value in 40% of female patients wearing a stable orthotic device. This suggests that orthotic devices impose a risk of reduction in muscular strength. 19 On the contrary, in another Spinomed study, which is in line with our results, wearing the orthosis resulted in a 73% increase in back extensor strength and a 58% increase in abdominal flexor strength, most likely because of increased muscular activity while wearing the orthosis. 1
In osteoporotic individuals, flexion exercises should be approached cautiously, at least in the early stages of engaging in a new exercise program, because of the potential of additional compression fractures associated with it.20,21 Spinomed could be a valuable tool to strengthen alternatively the abdominals dynamically and safely during this period. The difference in the improvements in trunk muscle strength between Spinomed studies is based only on the anthropometrical characteristics of the studies’ populations as the methodology and the devices used to measure force were identical. According to the results obtained from Osteomed studies, the orthosis brings an active erection of the spine of 60% on average of the deliberate maximum possible active erection. The wearing of the orthosis leads to an improvement of posture and statics, a straightening of the spine of 46% on average of the conscious maximum achievable straightening.9,22 The strengthening not only maintains bone density in the spine but also reduces the risk of vertebral fractures especially for back muscles. After a 2-year back exercise program, fractures (both wedging and vertebral compression fractures) in women were significantly less (only 11% in the exercise group as compared to 30% in the control group) several years after the exercises were discontinued. 23 Four out of the five subjects who started wearing Spine-X orthosis also increased their strength. Unfortunately, we were not able to perform a statistical analysis because of the small size of the sample. We still found it interesting to report these results in this article as there are no data available to the best of our knowledge about this specific orthosis (Spine-X). However, this orthosis is used by many patients all over Europe. Therefore, it is important to have more reports about this orthosis and its comparison with Spinomed since both the orthotics are targeting the same patient group and appear to be working with the same concept. Moreover, in our study, subjects from group A showed a high compliance to the use of the Spine-X orthosis and had a remarkable increase in trunk muscle strength. The details are given in Table 3.
Back pain
By far, the most frequent complaint of patients with osteoporosis is pain upon standing and under physical stress, particularly when bending forward. 24 Pain reduction is a usual endpoint in many published reports about orthotics. 25 In a 6-month period, the use of Spinomed significantly decreased pain as measured with VAS in group A. Moreover, after 6 months of Spinomed wearing, subjects felt 9% less pain compared with the younger controls. Generally, patients with osteoporosis (in our study both Spinomed and control) experience several kinds of pain: pain from external injury such as compressed vertebral fractures or pain from internal consequences of the osteoporotic state without injury, which has been accounted for pain in 89% of menopausal osteoporosis patients. 26 Back pain may arise either directly from vertebral fracture or indirectly from the consequences of spinal deformity, secondary degenerative change, and disk disease. In addition to the changes in vertebra and annuli, back pain may also be originated from impact on associated muscles, posterior ligaments, and facet joints. Nerve root compression may cause additional pain in the buttocks and legs. 27 A broadly accepted concept for the mechanism of osteoporotic pain is as follows. Nociceptors in the bone tissue respond to mechanical, thermal, and chemical stimuli. Injury (or inflammation) results in the release of a variety of chemical mediators (i.e. prostaglandins, cytokines, and growth factors). These mediators not only stimulate osteoclasts activity but also activate nociceptors and decrease their threshold for activation. 28 Menopause is well known to be one of the essential causes of osteoporosis in women. 29
The most important change after menopause is the depletion of estrogen that regulates the expression of various genes. A decrease in the amount of gene products including receptors and peptides required for the modulation of nociceptive transmission is evident.30,31
It has been observed that in most cases, the fracture has been recognized during a routine examination. The pain ranges from mild to intense, and it can become chronic, but it can also disappear after a few weeks, that is, once the fracture has consolidated. The persistence of pain is higher in people with slow bone repair. In the chronic phase, we observed a deformity of the spine due to loss of height of the vertebral body and the gradual emergence of a protuberant abdomen. The residual back pain in patients with healed vertebral fracture is typically of muscular origin and derives from the now permanent spinal deformity caused by the fracture. 32 Increased spinal kyphosis is likely to induce abnormal stress on the supporting structures of the spinal column and may cause chronic back pain that usually develops while standing, walking, or doing other normal daily activities. 33
Traditionally, spinal orthoses have been used in the management of thoracolumbar injuries treated with or without surgical stabilization. 34 However, lumbar corsets are not recommended as they place additional stress on fractures at the thoracolumbar junction. 35 Wearing the orthosis resulted in a 38% decrease in average pain versus 37% in our study in a 6-month period. 1 The results obtained from Osteomed studies also showed a statistically significant and clinically relevant reduction in chronic back pain by approximately 25% in female patients with osteoporosis while wearing orthosis for a period of 2.5 months. 25
Compliance of wearing an orthosis
An important problem in osteoporosis management is compliance. This study showed that modern orthoses have a high compliance emphasizing the usefulness of orthoses among all anti-osteoporotic strategies. The compliance of wearing an orthosis for 6 months was 66%. The compliance was highest for Spinomed (90%) followed by Osteomed and Spinomed active (50%), while Spine-X showed the lowest compliance of 30%. Compliance has been a big problem with patients on osteoporosis medications. Solomon et al. in a study of unselected older adults found relatively low compliance with medications used for osteoporosis. After 1 year, 45.2% of patients were no longer taking an osteoporosis medication; this increased to 52.1% after 5 years. 36 Cramer et al. reviewed 14 reports describing 14 databases. They reported persistence values of 32% for daily bisphosphonates and 44% for weekly bisphosphonates. In addition, the mean duration of therapy to discontinue was 139 days with daily bisphosphonates and 269 days with weekly bisphosphonates. 37 For this reason, pharmaceutical companies developed novel therapies such as the biannual dose of denosumab, which could aid patient medication adherence. However, the management of osteoporosis is not limited to drugs only. There should be compliance in supplementary means against the disease, for example, some guidelines for managing the disease with proper nutrition supplements or exercise. Only 50% of patients reported taking calcium and vitamin D supplements. 38 We recently published a report showing that the weekly frequency of physical activity in the Greek women population is extremely low (6% 1–2 h, 5% more than 2 h). 39 The most recent survey (2002 Eurobarometer survey) that looked at levels of physical activity in Europe also showed similar percentage of women who exercised more than 2 h/week (3.5%). 40
Spinomed’s compliance was unique. An explanation for the lower compliance of Osteomed and Spinomed active could lay on the orthoses design itself, which resembles clothing also in the perigenital region and is causing problems during voiding. A 40% of the general population report some form of trouble with voiding. More specifically in Greece, incontinence (of all types) has occurred in 20% of women aged 50–65 years (190,000 Greek women) and 30% of women aged above 65 years (300,000 Greek women). 41 For this reason, most women who participated in the current trial felt not so comfortable wearing these two orthoses. Therefore, we suggest that physicians should prescribe these orthoses in middle-aged sportive women mostly for prevention purposes. This could increase the compliance.
Here are the opinions given by some participants: patients’ files were randomly selected as 1, 3, 5, and 7 from the subgroups Spinomed, Spinomed active, Osteomed, and Spine-X, by a colleague not familiar with the study who called patients randomly, that is, patients 1, 3, 5, 7, and so on. Patients’ comments were as follows: for Spinomed (I wear it 1h/day especially in winter time; I feel less pain), Osteomed (It was a failure given me such an orthosis; I found difficulties to unzip it easily in case of urgent voiding), and Spine-X (I have wear it in the first year, especially in winter, have not see much according to pain or I do not wear it at all). The lowest compliance of Spine-X in the five subjects could not be explained due to small sample size, and hence, the study was inconclusive with this orthosis.
There are some limitations in our study especially with the selection of the right orthosis. For example, whether subjects included in Osteomed group could have been more benefited with some other orthosis. This seems to be actually a prescription problem whether the physicians are recommending the correct orthosis that fits best in patients. All the female participants were referred to our department according to the prescription from their physician from various departments. However, we believe that patients were prescribed with the right kind of orthosis since all the referral physicians were very experienced. The main drawbacks of this study were that the treatment with orthosis could not be masked and the small number of the participants. The effect of some drugs on back pain was not analyzed as controls also took drugs. All women were under anti-osteoporotic therapy. Moreover, knowledge of the treatment might have affected patient responses to questions or radiologist assessments.
Conclusion
In this study, the classic muscle function testing was modified and an apparative and isometric force measurement method that can be used in rehabilitation was developed to be applied in areas for testing documentation. Our results suggest that in women with established osteoporosis, wearing Spinomed orthosis for at least 2 h/day for 6 months decreased back pain significantly and increased personal isometric trunk muscle strength. Once someone wears it, they do not want to give it up—that is almost unheard of in brace wear. All spinal orthoses could be valuable instruments to help all requested rehabilitation programs such as spine muscle strengthening and postural correct behavior, but only when used properly. It is essential to make medical practitioners aware about the advantages of using an orthosis so that they are able to recommend the right kind of orthosis best fitted for their patients.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.