
Abstract
Currently available therapeutic options for the correction of osteoporotic posture changes are not effective. Rigid or semi-rigid orthoses are only applicable in the early phase after vertebral body fractures, and the knowledge about the efficacy of flexible spinal orthoses is limited. Therefore, the present study is aimed at investigating the efficacy of a flexible spinal orthosis without any stabilizing components in terms of posture improvement. Forty women aged (65.9 ± 8.4 years) with a proven osteoporosis (DXA ≤ −2.5) were randomized to receive either of three treatment regimens: (i) Orthosis (Thämert Osteomed) with paravertebral/lumbosacral air chamber pads (as commercially available); (ii) The same orthosis without air chamber pads; and (iii) Placebo body stocking. Measurements were performed with a 3D real-time ultrasound topometry system (Zebris® CMS 70). The posture correction was substantially and significantly more marked in the first group (38% of the maximally possible intentional erection) as compared to the second (21%) and third group (13%). The orthosis with air chamber pads causes a clinically meaningful trunk support in patients with osteoporotic posture changes. Since the device contains no rigid stabilizing elements, the change in posture is considered to be a result of muscle activation due to sensomotor stimulation by the air chamber pads.
Objective
Osteoporosis is increasingly recognized as a significant medical and socio-economic problem (Ismail et al. 1998; Cummings and Melton 2002; Finnern and Sykes 2003; Johnell and Kanis 2006). Vertebral fractures are the main clinical consequences of spinal osteoporosis and constitute a major public health burden in developed countries (Dennison and Cooper 2000). Spinal osteoporosis is associated with serious physical, psycho-social and health consequences. It leads to loss of bone density, reduced pulmonary function (Lombardi et al. 2005), disability and pain (Nevitt et al. 1998; Hall et al. 1999), impaired health-related quality of life (Cockerill et al. 2004) as well as increased mortality (Center et al. 1999) and changes in the alignment of the spine with additional physical stress on the mechanically less robust ventral parts of the vertebral bodies. Therapeutic approaches therefore include drug treatment as well as appropriate muscle, coordination and postural training. In addition to active measures aimed at improving the posture of the spine and specifically at straightening the thoracic spine, the provision of orthotic devices as part of the adjunctive therapeutic management is clinically indicated and has been previously discussed (Lin 2004; Pfeifer et al. 2004; Vogt et al. 2005). In particular, the findings reported for a functional osteoporosis orthosis show that it induces improvements in posture towards the norm and is at the same time associated with marked wearing comfort and excellent compliance even during the desired all-day wear (Vogt et al. 2005). The external appearance of the orthosis Osteo-med resembles an item of clothing called a ‘body’ and is characterized by a constructively functional cut with Velcro tabs exerting pressure in the lumbosacral region as well as air chamber pads fixed in the paravertebral and lumbosacral areas which are filled with air to between ⅔ and ¾ of their maximum capacity. Rigid stabilizing elements are deliberately not used (Figures 1a and 1b). A detailed description of the product can be found in, e.g., Hildebrandt et al. (2003).
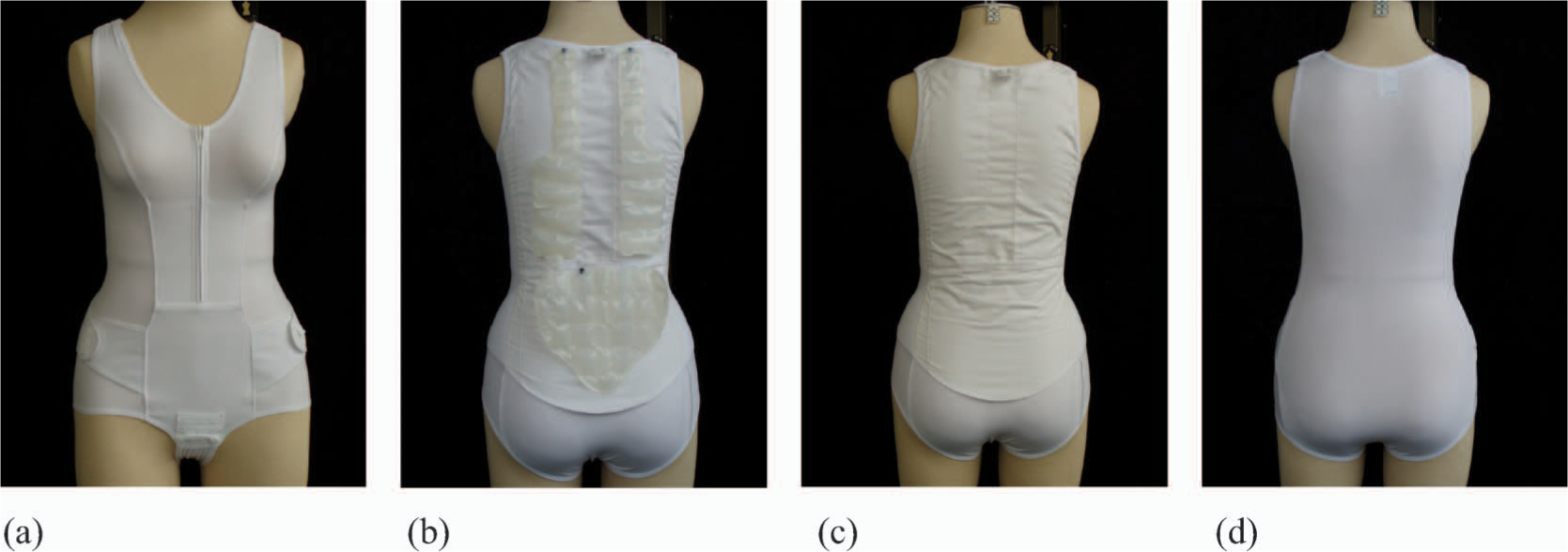
(a) Front view of the Osteo-med osteoporosis orthosis; (b) Dorsal view of the Osteo-med osteoporosis orthosis (for demonstration purposes the air chamber pads are shown on the outside); (c) View of the orthosis without air chamber pads; (d) View of the placebo device.
It remains unclear to what extent the demonstrable straightening of about 60% (Vogt et al. 2005) can be attributed to the effects of the air chamber pads alone or rather to the whole device functioning as a unit. Therefore, the present study is aimed at assessing the effects of the different components of the orthotic device on the immediate changes of the sagittal spinal posture in female patients diagnosed with post-menopausal osteoporosis.
Patients and methods
Participants were recruited through public advertisements in local newspapers. The patient sample was selected according to predefined inclusion and exclusion criteria (Table I). For the a priori calculation of the optimal random sample size an α-level of 5% (one-sided [the trial was planned with a one-sided hypothesis because provision of the orthosis Osteo-med would be only recommended if the group comparison revealed a significant improved posture correction]) and an error probability of β = 0.2 was set (BiAS for Windows 7.0). The variance (δ 2 = 3.61) and the minimum medically relevant difference (2°) were estimated on the basis of previous research (Vogt et al. 2005). Accordingly, 45 patients (aged 66.9 ± 8.6 years, height 163 ± 6 cm, weight 61.6 ± 11.1 kg) were included in the study. All patients were screened by clinicians, skilled in the evaluation and the management of osteoporosis, to achieve a therapeutically relevant straightening of the thoracic spine (clinical inspection). Five participants (aged 75.3 ± 4.5 years, height 163 ± 2 cm, weight 69.5 ± 3.5 kg) had to be excluded from the study due to various reasons (failure to reach the criterion of spinal erection n = 1; comorbidity, e.g., knee arthritis n = 2; personal reasons, e.g., lack of interest n = 2). The 40 individuals (aged 65.9 ± 8.4 years, height 163 ± 7 cm, weight 60.3 ± 11.5 kg) who participated in the entire experiment constituted the effective sample of this study. The experiment was approved by the Institutional Review Board and followed the Declaration of Helsinki recommendations for research involving human subjects. Informed written consent was obtained from all subjects prior to their participation in this research. Participants were allowed to stop the testing at any time without any consequences. The same assessors were used over the course of the study in order to exclude any potential inter-tester variability.
Inclusion and exclusion criteria
Assessment of the kyphosis angle
A three-dimensional ultrasonic movement analysis system (Zebris CMS 70©, Germany) was used to collect external kinematic data with an absolute accuracy better than 0.6 mm (Himmelreich et al. 1998). Sufficient test-retest reliability of the measurement system has been reported previously (Vogt and Banzer 1997). Three ultrasound microphones, determining a local coordinate system, were used to track four low-mass ultrasonic markers (diameter 10 mm, weight 3 g each). The orthogonal coordinate system followed the right-hand rule and had the positive x-direction orientated in the direction of forward progression, the positive z-direction orientated to the left and the positive y-direction orientated vertically upward. Spatial marker positions (x, y, z) were reconstructed by triangulation in relation to the laboratory coordinate system. The main outcome measure, thoracic kyphosis, was according to previous studies based on the measurement of the angle between C7 and Th12 projected onto the sagittal plane of the orthogonal reference frame (Gajdosik et al. 1994) (Figure 2).
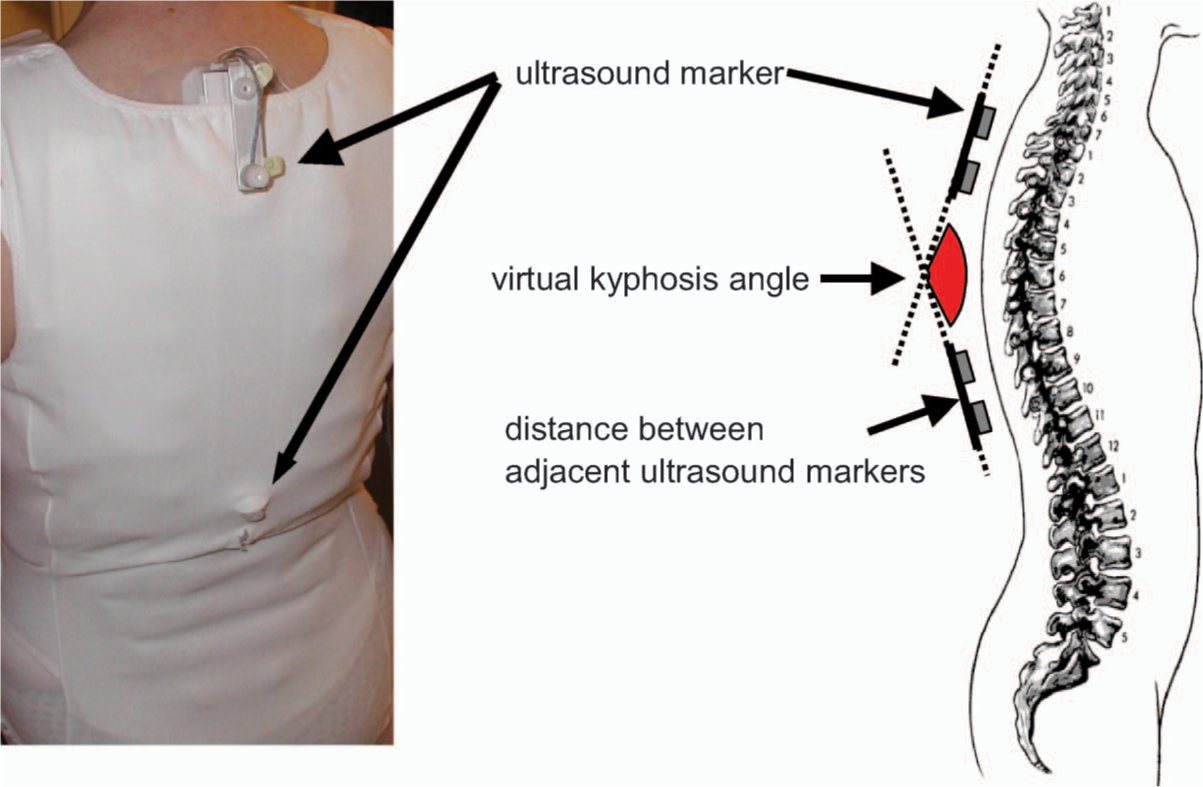
Positioning of markers and assessment of the ‘virtual’ kyphosis angle of the thoracic spine by motion analysis system.
Before testing, subjects were asked to stand motionless in a relaxed (normal) upright position, with surface markers visible to the ultrasound microphones. They were instructed to focus on a point on the wall positioned directly in front of their standing position. This experimental protocol was used for calibrating the angular position during standing (anatomical zero) and for computing relative angular displacement. The measurement system was calibrated prior to each data collection session. Data was sampled at 30 Hz, monitored in real time and stored on PC for later offline analysis. After data acquisition kinematic data was optically controlled and low-pass filtered (critical damped, 2nd order, double pass, 8 Hz cut-off). Measurements containing reflection artifacts were excluded from further analysis. Data was processed using LabView (National Instruments©) and ALEA© Solution software (Switzerland).
The following versions of the orthotic device were used: Spontaneous posture when wearing a Thämert Osteo-med with air chamber pads
(commercially available version); Spontaneous posture when wearing a Thämert Osteo-med without air chamber pads; Spontaneous posture when wearing a placebo orthotic device (body without directed
pressure).
Figures 1b – 1d show the
different orthotic and placebo devices compared in this study. To assess the posture
alterations induced by the Osteo-med osteoporosis orthosis, the kyphosis angle was
measured in all patients under the three different test conditions with the three devices
administered in random order (computer-assisted block randomization, BiAS for Windows
7.0). The respective degrees of straightening were assessed relative to the individual's
conscious maximum straightening of the spine assessed by ultrasound topography.
Statistics
Levene and Kolmogorov-Smirnov-tests were performed to examine the homogeneity of variance and the normal distribution of the parameters in order to present them in terms of mean and standard deviation. To evaluate the differences occurring under the different test conditions of wearing the orthotic or placebo devices, one-way analysis of variance (ANOVA) for repeated measures was used. Scheffé test was used for post-hoc analysis of significant findings. A one-sided p-value of less than 0.05 was considered statistically significant. All statistical computations were made with a commercial statistics package (SPSS, SPSS Inc, USA).
Results
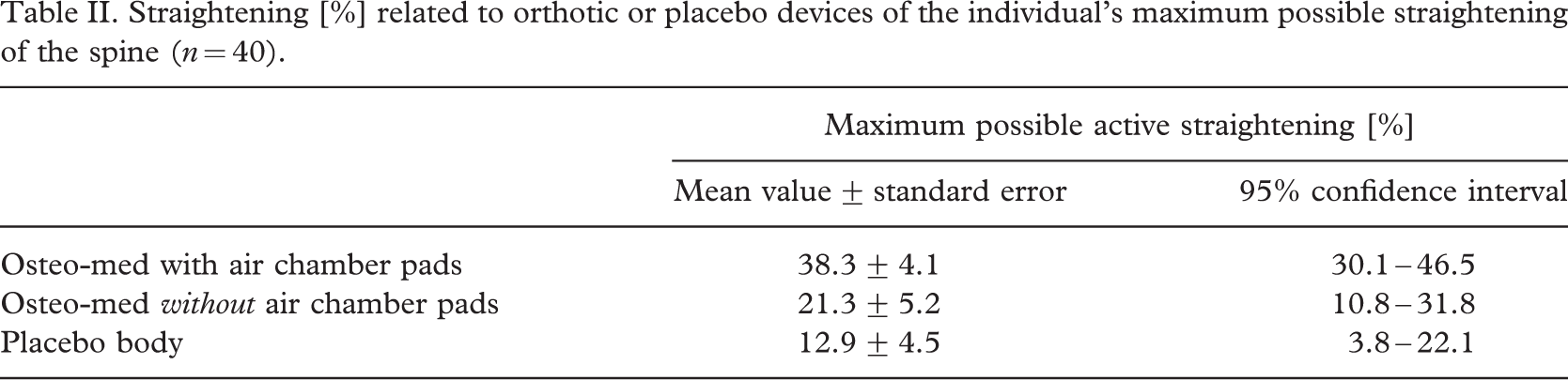
The results of the kinemetric measurements of the maximum straightening of the spine that can be actively achieved by the patient indicate an average straightening of the thoracic spine in the study sample of almost 5°. Regular wearing of the osteoporosis orthosis with partially filled air chamber pads, as intended by the developer and provider of the device, yielded a straightening of the thoracic spine of on average 38%. In contrast, a significantly smaller degree of straightening (21%) was achieved with the device without air chamber pads. The use of the placebo ‘body’ did not produce any consistent effects on spinal posture compared with the two orthotic devices. Figure 3 demonstrates clearly that patients showed a straightening of the thoracic spine only with regular use of the orthosis. More than 2/3 of the participants achieved a stretching of the thoracic spine of over 30% relative to their individual maximum degree of the actively possible straightening. The 95% confidence intervals of relative postural changes (Table II) corroborate this general impression and indicate at the same time the comparatively small significance of the effects that can be attributed to placebo.
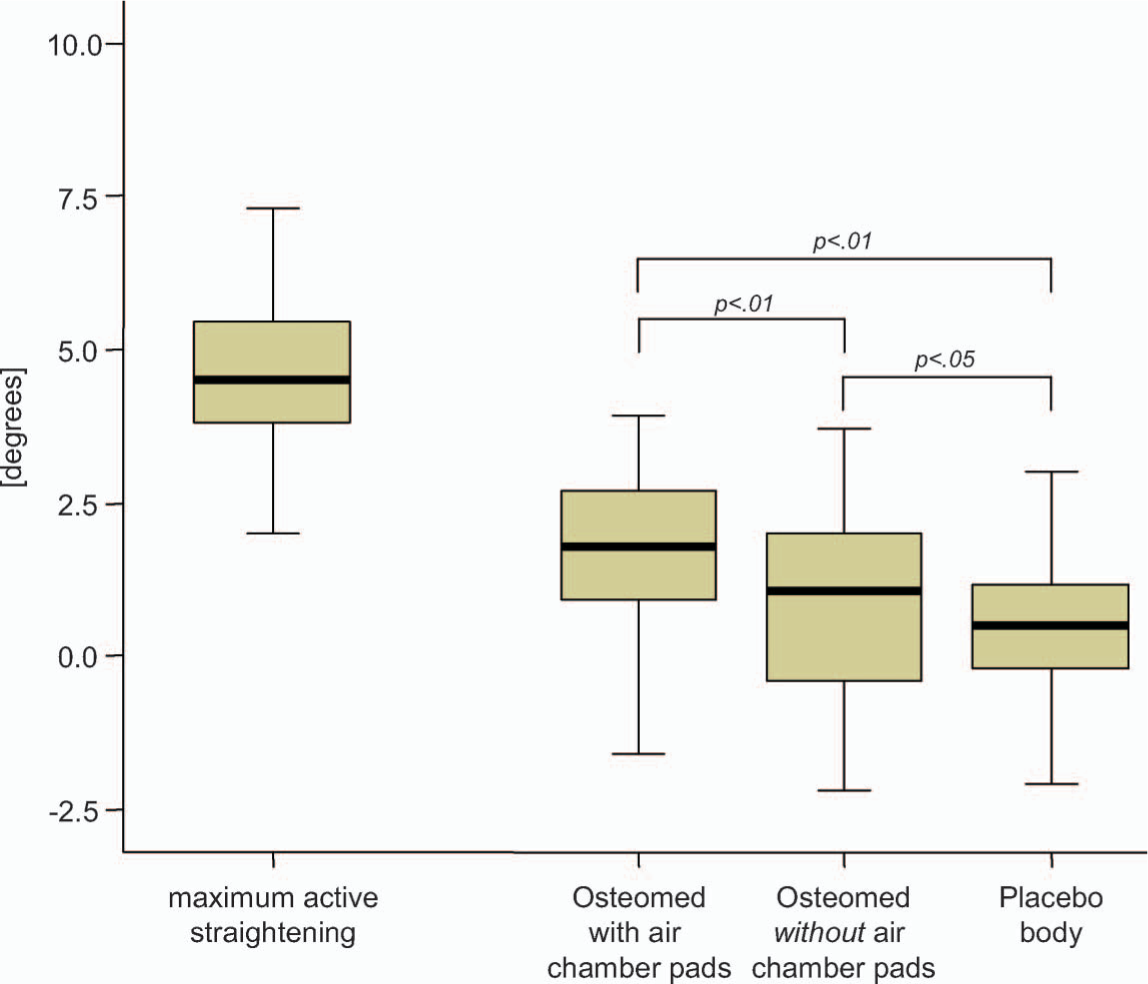
Maximum, minimum, median, and interquartiles of absolute straightening related to orthotic or placebo devices in degrees compared to the individual maximum possible straightening of the spine (n = 40).
Straightening [%] related to orthotic or placebo devices of the individual's maximum possible straightening of the spine (n = 40)
Conclusion
The current study focused on the specific mechanisms of the osteoporosis orthosis developed by Hildebrandt et al. (2003). According to the findings, the use of an orthosis with integral air chamber pads is associated with spontaneous straightening of the spine of almost 40% of the conscious maximum achievable straightening. The use of an orthosis with pads hence leads to a clinically significant straightening of the trunk in terms of an improvement in posture and stability. These results are in agreement with findings of previous investigations (Vogt et al. 2005), which also demonstrated a straightening or active extension of the spine following the use of an Osteo-med. The use of the partially elastic orthosis device with Velcro tabs without additional pads leads, due to compression-traction stimuli, to half the straightening of the conscious maximum achievable.
The greater reduction of kyphosis with integrated pads confirms the mechanism of action of the orthosis as a functional unit, as intended by its developer, with the different construction elements possibly contributing partially to the stimulation of the active muscular straightening. Since the Osteo-med does not use rigid stabilizing elements, the demonstrated thoracic straightening is achieved through active muscle use following sensomotoric stimulation. With the investigated orthosis, these stimuli are reinforced by the integrated and interlinked air chamber pads. From a neurophysiological point of view, the more pronounced effects associated with the pads can be explained through an increased stimulation of cutaneous mechanoreceptors related to the massage-like effects of the traction-compression stimuli (Laube and Hildebrandt 2001). Otherwise studies demonstrated that people affected by osteoporosis had more postural sway and greater use of hip strategies for maintaining balance (Lynn et al. 1997). Additionally flexed posturing, often caused by osteoporosis, increases the propensity to fall (Wolfson et al. 1992). Therefore, it can be speculated that the orthosis induced facilitation of back extensor muscles with repositioning of the spine and shift of the centre of gravity contributes to balance improvements and fall prevention, as it has been demonstrated by a weighted kypho-orthosis (Sinaki and Lynn 2002). The functioning of the orthosis as a unit is also corroborated by the demonstrated extent of the absolute straightening in degrees, since a clinically relevant change (>2°) was only achieved with regular use of the Osteo-med. The straightening with the placebo device of on average 13% of the actively possible straightening is significantly different from the results yielded under the trial conditions with or without pads; with an absolute straightening of on average <1° it does not reach a clinically relevant level. The demonstrated mean straightening of 13% might be explained by the patients focusing attention on their posture as a consequence of the particular examination or laboratory situation.
Overall the results demonstrate the role and appropriateness of the principles chosen for the construction and manufacturing of the orthosis. It could be presumed that the stimulation of proprioception, caused by the lumbar and thoracic air chamber pads working in combination with a partially flexible tension band, yet notably without rigid elements, affects the spontaneous posture and consequently leads to an unconscious muscular straightening or active stretching. These suggestions are supported by the fact that the air chambers of the orthoses are interconnected by a tube system and are inflated only up to ⅔ of their maximum capacity. Although encapsulated in fabric, the whole air-chamber system remains flexible and air can float between the single chambers during body movements. In that way, inflating the air-chambers does not result in orthoses induced mechanical stabilization. The investigated orthotic device hence stimulates the use of the body's own neurophysiologic resources to improve posture and function. Regular use of the orthosis provides essential elements in the effective management of osteoporosis. On the basis of the active spontaneous erection with reduction of the load on the particularly vulnerable ventral portions of the thoracic vertebrae and the subjectively perceived erection-related pain reduction (Vogt et al. 2005) the device, may also contribute to a reduction in fear and incidence of falling as proven in other appliance surveys (Pfeifer et al. 2004).
Financial disclosure
This study was supported, in part, by Thämert, which provided the orthoses and funding for the study (Thämert had no control over the decision to approve or submit the manuscript for publication).