
Abstract
Study Design
Systematic review.
Objectives
Spinal orthoses are frequently used to non-operatively treat osteoporotic vertebral fractures (OVF), despite the available evidence is rare. Previously systematic reviews were carried out, presenting controversial recommendations. The present study aimed to systematic review the recent and current literature on available evidence for the use of orthoses in OVF.
Methods
A systematic review was conducted using PubMed, Medline, EMBASE and CENTRAL databases. Identified articles including previous systematic reviews were screened and selected by three authors. The results of retrieved articles were presented in a narrative form, quality assessment was performed by two authors using scores according to the study type.
Results
Thirteen studies (n = 5 randomized controlled trials, n = 3 non- randomized controlled trials and n = 5 prospective studies without control group) and eight systematic reviews were analyzed. Studies without comparison group reported improvements in pain, function and quality of life during the follow-up. Studies comparing different types of orthoses favor non-rigid orthoses. In comparison to patients not wearing an orthosis three studies were unable to detect beneficial effects and two studies reported about a significant improvement using an orthosis. In the obtained quality assessment, three studies yielded good to excellent results. Previous reviews detected the low evidence for spinal orthoses but recommended them.
Conclusion
Based on the study quality and the affection of included studies in previous systematic reviews a general recommendation for the use of a spinal orthosis when treating OVF is not possible. Currently, no superiority for spinal orthoses in OVF treatment was found.
Introduction
Spinal orthoses are traditionally applied treating thoracolumbar fractures, but their mechanism is currently not completely understood.1,2 Nevertheless, over 60% of spine surgeons prescribe an orthosis for the treatment of fractures, degenerative diseases or use them after surgical treatment. 3 Most recently a systematic review found no evidence treating traumatic spinal fractures conservatively with an orthosis. 4 However, for osteoporotic vertebral fractures (OVF), spinal orthosis are recommended and previous systematic reviews highlight their benefits though the evidence of included studies is limited.5-11 But methodical aspects of the included studies were not fully evaluated possibly resulting in controversial recommendations.5-12 Additionally, several aspects like the type of diagnostics used, fracture region, number of fractures, orthosis treatment (daily treatment and duration) were sparsely reported. Although several reviews highlight the low quality of included studies, their recommendations are based on them. Besides a risk of bias (RoB) assessment, quality examinations are rare. We aimed to report on the evidence for spinal orthosis treating OVF and describe the treated population, fracture morphology and orthotic treatment. Secondarily, the investigated publications were graded using quantitative quality scores. Thirdly, previous systematic reviews were analyzed and qualitatively graded.
Materials and Methods
The present study was registered on the International Prospective Register of Systematic Reviews (PROSPERO) network (CRD42020177426) before starting the review process and performed accordingly to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
The first authors searched within PubMed, Medline, EMBASE and Cochrane Central Register of Controlled Trials (CENTRAL) without a limitation of the publication date but limited to English and German publications until April 2020 and updated the studies using PubMed messenger. According to the PI (CO) scheme the following question was formulated: Does spinal orthoses improve the outcome of patients suffering from thoracolumbar spinal fragility fractures and related deformities?
An example for the search strategy is outlined for PubMed:
(((((Orthotic devices [Mesh] OR Spinal orthos*) AND ((Spinal Fractures [Mesh] OR Spinal fracture) OR (Spinal Curvatures [Mesh] OR (Adult spinal deformity)) OR ((Fractures, Stress [Mesh] AND Spine) OR (Fracture, Spontaneous [Mesh] AND Spine)) OR (Osteoporosis [Mesh] AND Spine) OR (Osteoporotic Fractures [Mesh] AND Spine))) AND (“german" [Language] OR “english" [Language])) NOT (“case reports" [All Fields] OR “comment" [All Fields] OR “letter" [All Fields])) NOT cervical). Case reports, comments and narrative reviews were excluded. An exclusion based on the level of evidence or study type was not done. The remaining manuscripts were considered for inclusion. Retrieved titles of studies, abstracts and full texts were screened in triplicate by PP, UJS, CEH. At each step controversy was discussed until consensus was achieved. The screening process and extracted data included in tables and figures are presented in Figure 1. Data extraction and qualitative assessment were done by PP and UJS using a predefined Research electronic data capture (REDCap) form.
13
The Coleman Methodology Score (CMS) was assessed for all studies.
14
Higher scores indicate a less risk for bias and confounding factors. The CMS was graded as followed: excellent (85-100 points), good (70-84 points), fair (50-69 points), and poor (<50 points).
15
For non- randomized trials the Newcastle-Ottawa Scale (NOS) was assessed.
16
In addition, the total score was presented in percentage of the maximum available score, low risk of bias was considered if the score achieved ≥50% in the three categories.
17
Randomized controlled trials (RCT) were examined using the modified RoB tool.
18
Based on the 10 questions a score of 10 points is possible; a point is given for each question. A score >8 points indicate low risk of bias. In addition, the Detsky Score was used, a score ≥15 (75%) indicate high quality.18,19 Scheme according to PRISMA criteria and retrieved data. ** Manuscripts were excluded due to wrong treatment indication or comparison to surgery (scoliosis, comparison of non-operative to operative treatment, missing relevant outcome). Retrieved studies were additionally excluded due to missing outcome definition (n = 1),
37
inclusion of patients ± fracture (n = 5).38,41,55-57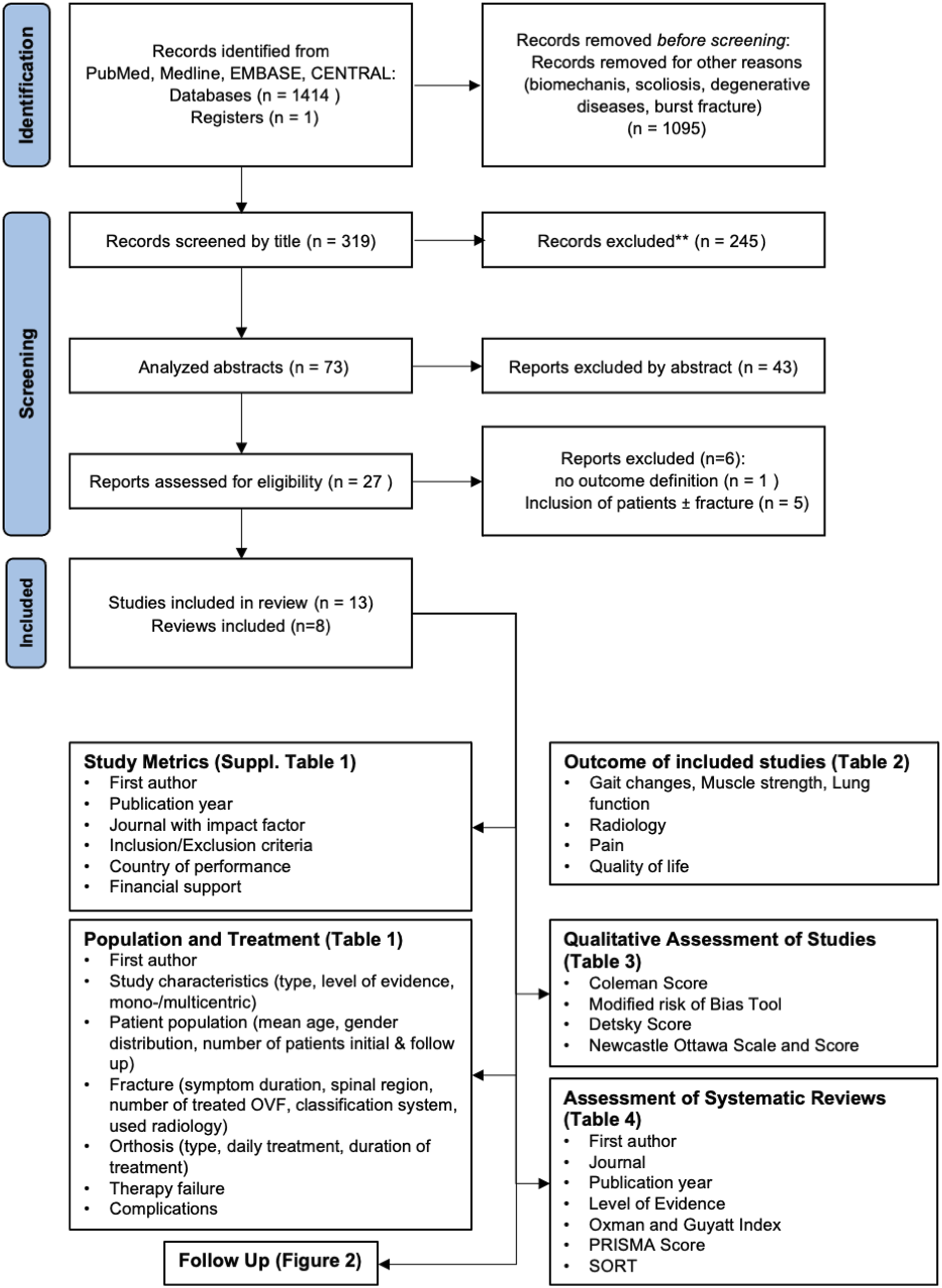
Results extracted from analyzed studies were summarized in a narrative preformatted form after review of each author and approved by PP, UJS, CEH. The primary outcome were gait changes, radiological changes, pain, functional outcome, and quality of life (QoL). If two studies seemed to share data, these studies were summarized.
Studies were categorized as followed: report of only one orthosis without comparison, comparison of orthoses types, comparison of orthosis to no orthosis.
Previous systematic reviews were assessed regarding the following parameters: research question, similar articles included, reason for repetition of the review mentioned, recommendation of spinal orthosis, Oxman and Guyatt Index and PRISMA Score and Strength of Recommendation Taxonomy (SORT). The Oxman and Guyatt Index was categorized as followed: strong weakness 1-2 points, severe 3-4 points, moderate 5-6 points, minimal >7 points.20,21
The PRIMSA score was graded as followed: <19 low quality, 19-22.5 moderate quality, >22.5 high quality.22,23
A meta-analysis was not performed due to the heterogeneity of data.
Results
Thirteen studies and eight systematic reviews were analyzed. Seven studies were performed in Asia (four in Japan24-27 and each one from China, 28 South Korea, 29 Taiwan 30 ) and six from Europe (two from Germany31,32 summarized to one due to an assumed shared patient cohort and one from Netherlands, 33 Denmark, 34 Greece, 35 and Italy 36 each; Supplemental Table 1). Seven studies defined a precise inclusion time frame.24,26,27,29,33,34,36 All studies were unblinded. Three studies had a financial support,29,31,32 two were funded by an orthosis manufacturer.31,32
Population and Treatment. Study Characteristics, Investigated Patient Cohort and Fracture Related Parameters as Well Orthotic Treatment, Therapy Failure and Complications are Presented.
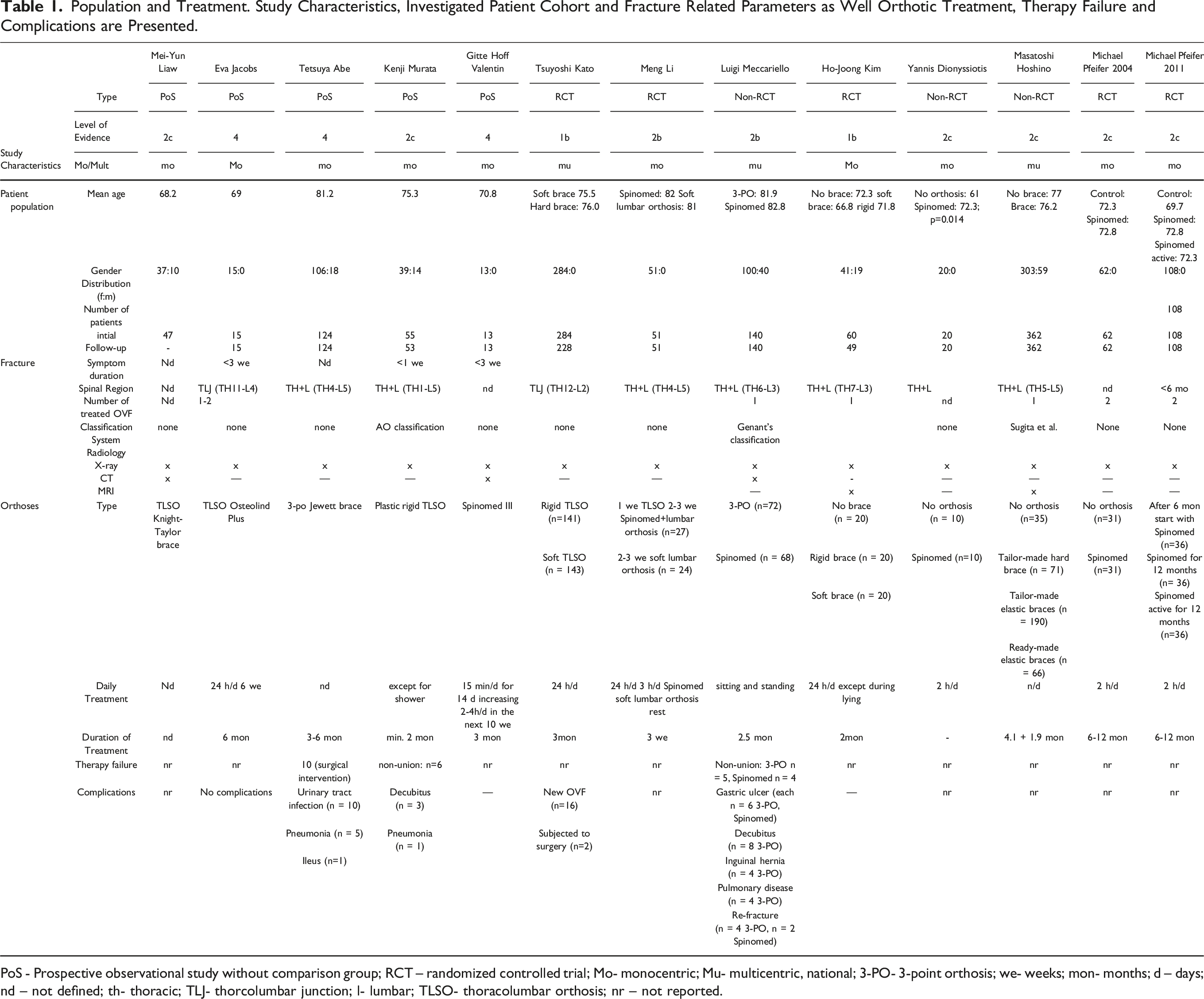
PoS - Prospective observational study without comparison group; RCT – randomized controlled trial; Mo- monocentric; Mu- multicentric, national; 3-PO- 3-point orthosis; we- weeks; mon- months; d – days; nd – not defined; th- thoracic; TLJ- thorcolumbar junction; l- lumbar; TLSO- thoracolumbar orthosis; nr – not reported.
Six studies used solely radiographs28,30-32,34,35 and five studies radiographs and magnetic resonance imaging (MRI).25-27,29,33 Each one study combined X-rays, CT scan and MRI 24 or X-rays and CT. 36
Daily treatment ranged from 15 minutes/day (one study
34
) at the beginning, 2-3 hours/day (four studies28,31,32,35) to the whole day (four studies26,27,29,33) or only during sitting and standing.
36
Three studies did not define the daily duration.24,25,30 The duration of treatment ranged from 2.5 months to 1 year (Table 1). The different follow- up times are shown in Figure 2. Presentation of the different follow-up visits of the included studies.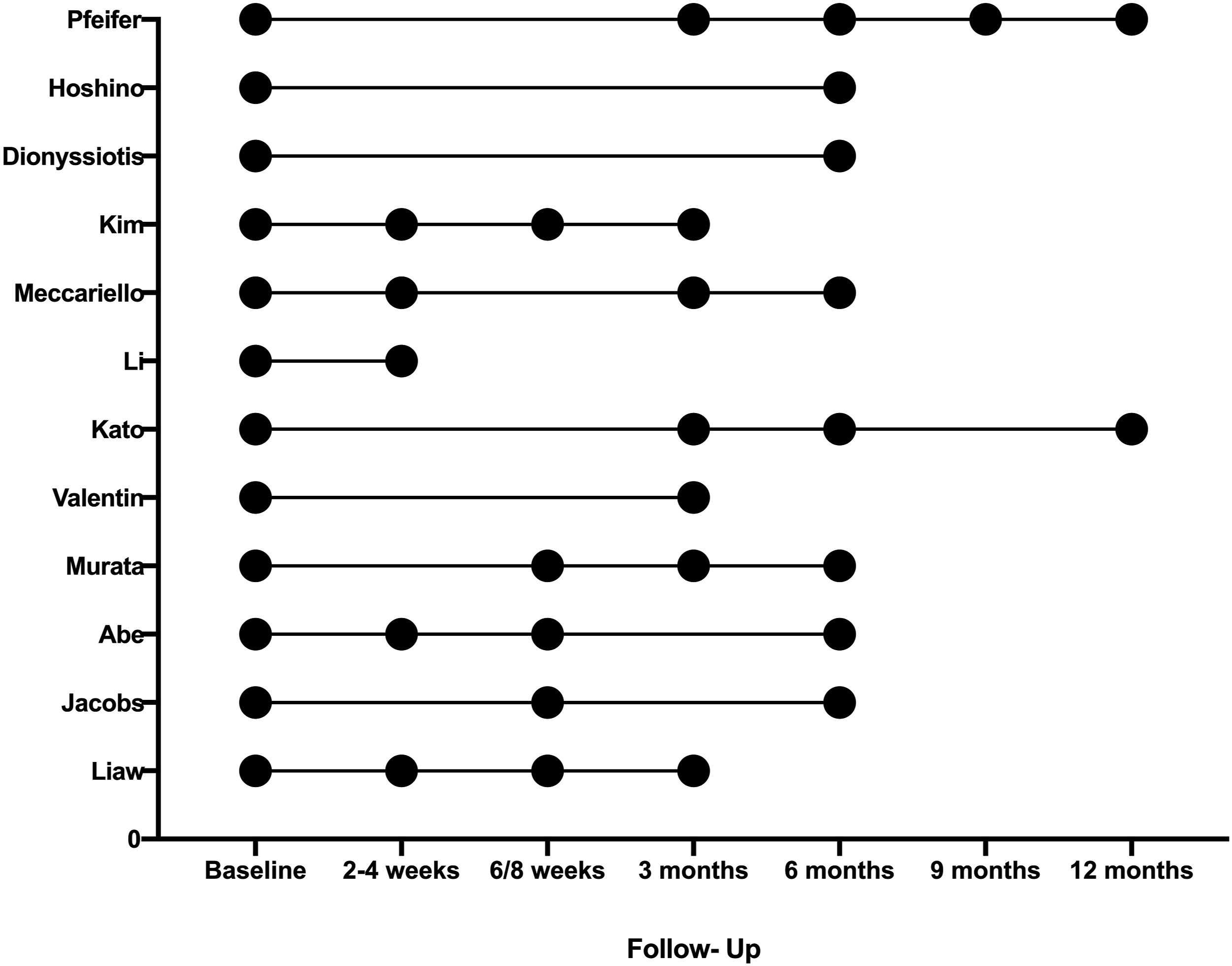
Spinal Orthosis Without Comparison (n=5)
Summarized Outcomes of Included Studies Separated According to the Paragraphs.
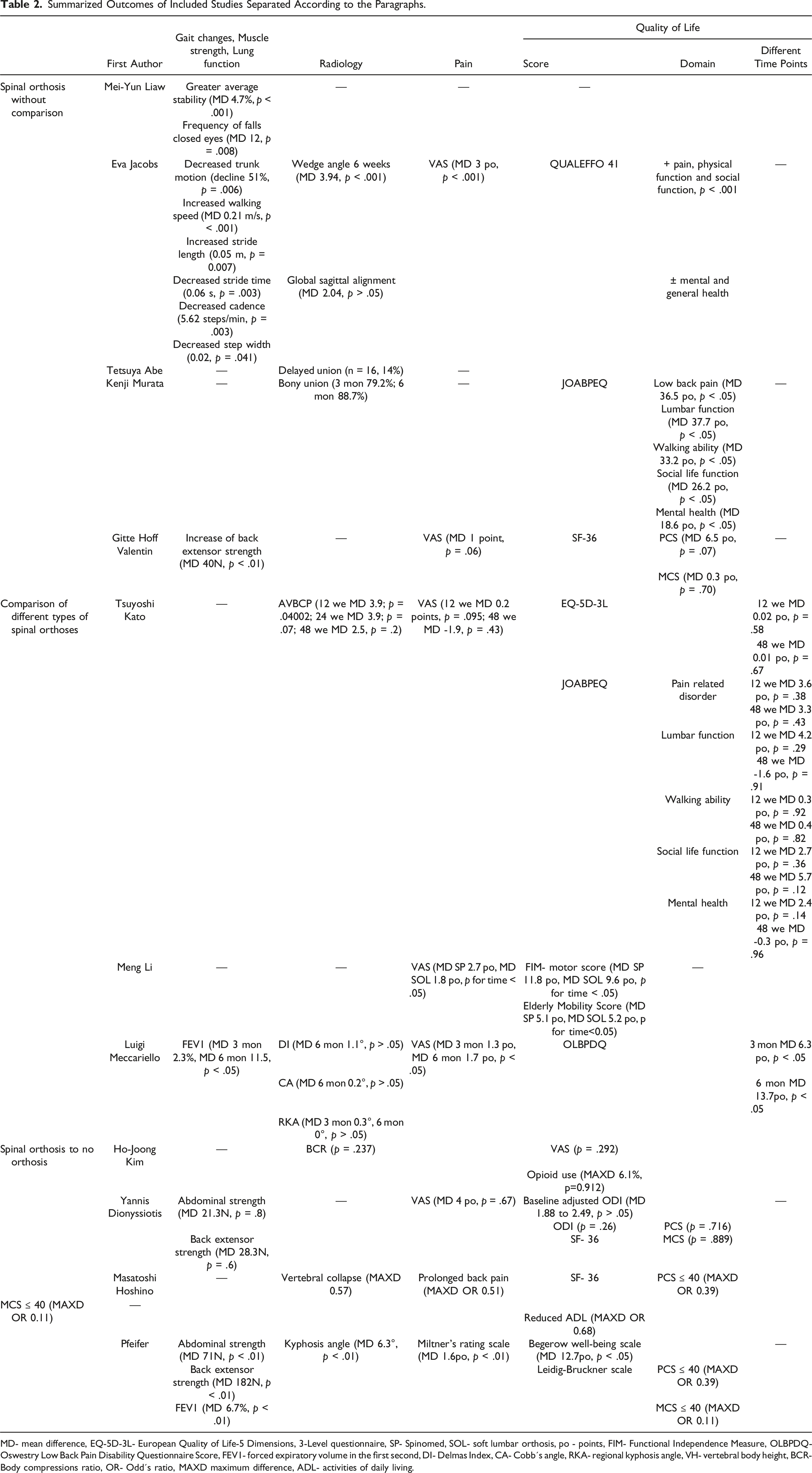
MD- mean difference, EQ-5D-3L- European Quality of Life-5 Dimensions, 3-Level questionnaire, SP- Spinomed, SOL- soft lumbar orthosis, po - points, FIM- Functional Independence Measure, OLBPDQ- Oswestry Low Back Pain Disability Questionnaire Score, FEV1- forced expiratory volume in the first second, DI- Delmas Index, CA- Cobb´s angle, RKA- regional kyphosis angle, VH- vertebral body height, BCR- Body compressions ratio, OR- Odd´s ratio, MAXD maximum difference, ADL- activities of daily living.
Several aspects of QoL improved but Jacobs et al were not able to detect changes for general and mental health.27,33 In contrast, Valentin et al. did not observed significant improvements in pain and QoL. 34 The effects were predominantly found during the first 6-12 weeks.27,33 Using an orthosis resulted in a success rate of >80% analysing dynamic X-ray examination regarding persistent instability24,27 but high intensity on T2-weightened MRI and vertebral instability >5° at 3-week follow were identified as risk factors for treatment failure. 24
Comparison of Different Types of Spinal Orthoses (n = 3)
The Spinomed orthosis led to a significant higher forced expiratory volume in the first second compared to a 3-point orthosis (3-PO) Tables 1 and 2. 36
The anterior vertebral body compression percentage (AVBCP) differed between soft and rigid brace after 12 weeks but not after 24 and 48 weeks. A higher decrease was found in the rigid brace group (MD 3 points) compared to the soft brace group (MD 1.6 points) during the follow-up. 26 Other radiological parameters like the Cobb´s angle did not differ comparing a Spinomed to a 3-PO. 36
A significant improvement in pain, QoL for the Spinomed orthosis at 3- and 6 months follow-up but not after 1-week or 1-month was detected in comparison to a 3-PO. 36 Pain decreased significantly over time independent of the orthoses type. 28 In contrast to the study of Meccariello et al., QoL did not differ comparing orthoses types in two studies.26,28 No association between QoL and AVBCP was determined. 26
Spinal Orthosis to No Orthosis (n = 5)
Wearing an orthosis – independent of the type- did not lead to a significant improvement in QoL, pain, decelerated increase of radiological compression or minimized opioid use compared to patients who do not wear an orthosis.29,35 Pain and QoL improved over time independent of the orthotic treatment.25,29,35 In the study of Dionyssiotis et al, 35 the significantly younger control group refused to wear an orthosis. The two studies of Pfeifer et al31,32 were summarized because the difference of cohorts could not be ensured (please see Table 1, 31 and Group A 32 regarding age and consecutive variables). In their planned crossover study, patients refused after 6 months to discard the orthosis. In contrast to the above-mentioned studies, Pfeifer er al.31,32 observed a significant decrease for kyphosis angle using three-dimensional photomorphometry, improved body sway path length, body sway velocity, pain, QoL and abdominal and back extensor muscle strength. Noteworthy, Pfeifer et al31,32 determined similar changes starting to wear the orthosis after 6 months Tables 1 and 2.
Quality Assessment
Qualitative Assessment of the Included Studies.
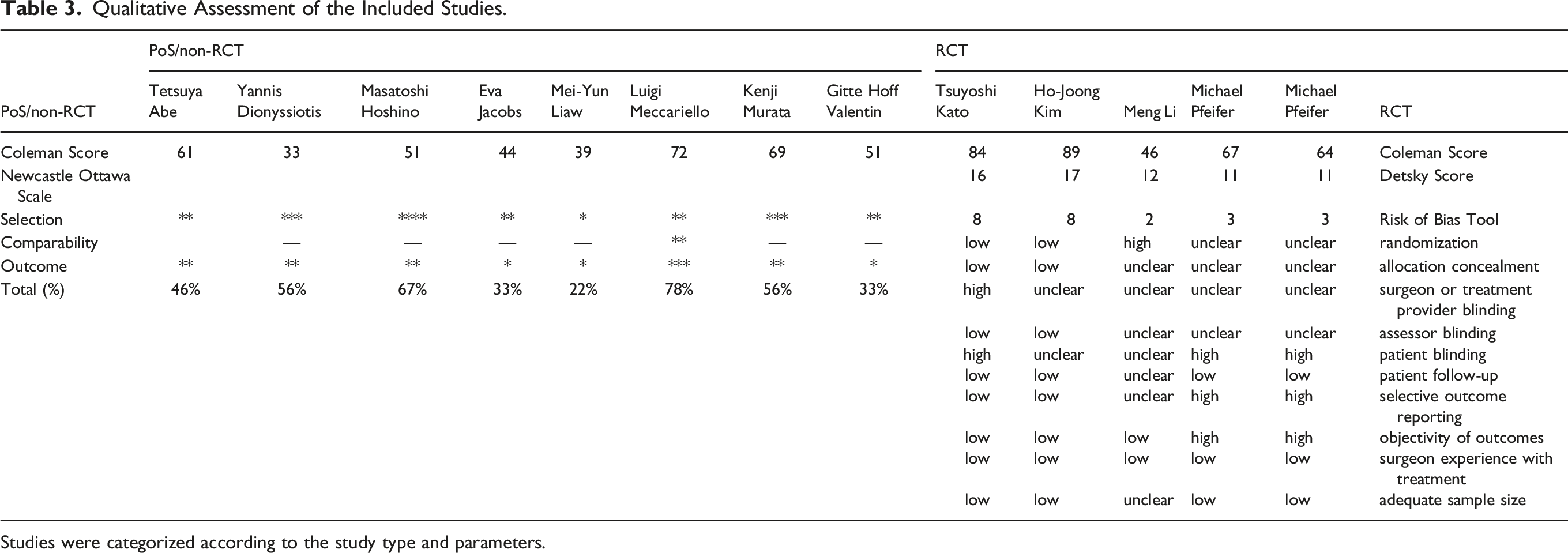
Studies were categorized according to the study type and parameters.
Comparison to Other Systematic Reviews (n = 8)
Assessment of the Included Systematic Reviews Including Quality Assessment and Strength of Recommendation Taxonomy (SORT).
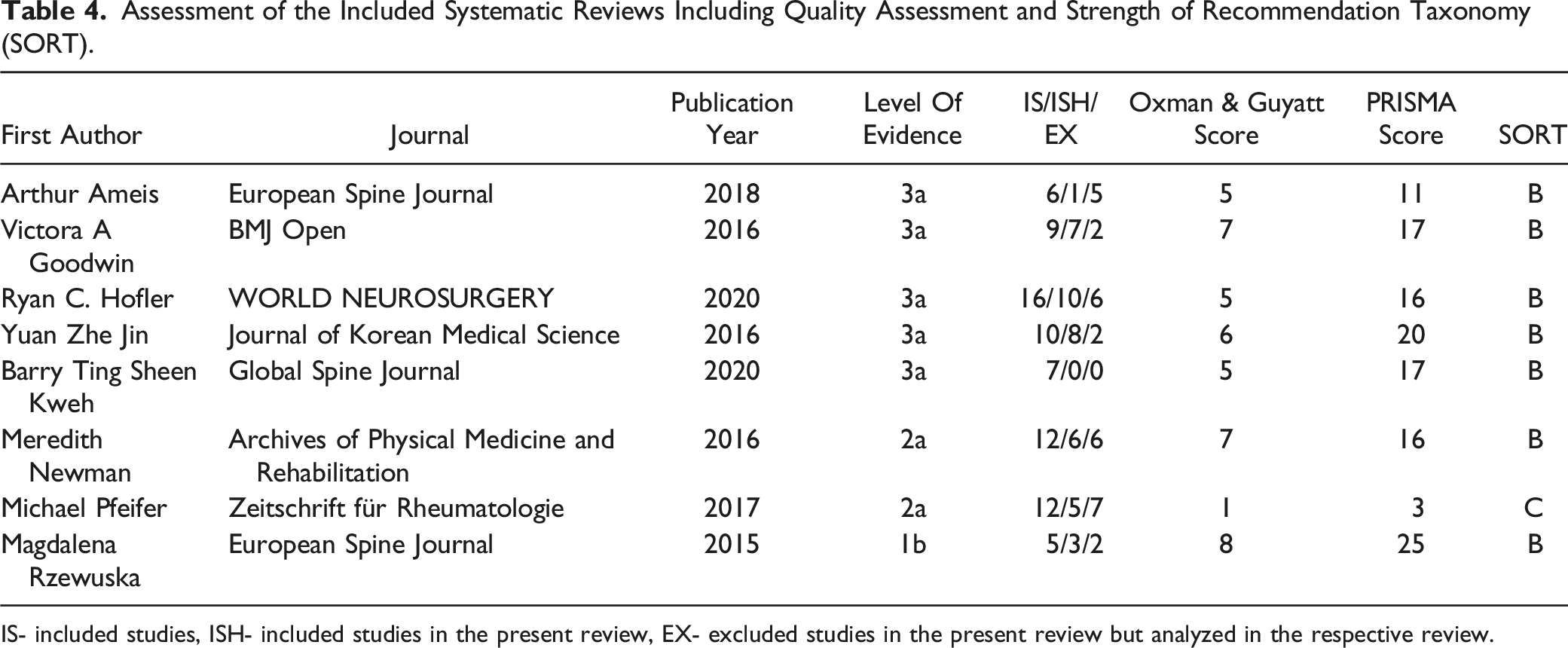
IS- included studies, ISH- included studies in the present review, EX- excluded studies in the present review but analyzed in the respective review.
Three studies analyzed the effects of orthoses independent of their type on biomechanics, pain, QoL.7-10 Besides of bracing Goodwin et al investigated the effects of taping and Hofler and Jones included studies with a crossover design and operatively treated patients.6,12 Included articles in previous reviews, in the present review and excluded articles are summarized for each review in Table 4. The following articles were included in previous reviews and excluded here as follows: included in six6-10,12 and excluded here due to no outcome definition, 37 included in two9,10 and excluded due to language availability, included in three7,9,10 and excluded due to missing fracture status (with/without/healed) (n = 5),38−42 included in one 6 excluded because the intervention was taping, 43 included in one 11 and were excluded because primary intervention was medication, 44 included in one 12 and excluded here due to a crossover design to surgery,45,46 comparison to kyphoplasty, 47 primary comparison regarding bed rest and inclusion of traumatic fractures, 48 orthosis not primary intervention and solely report of reduction over time, 49 orthosis not primary intervention. 50
Despite five5,7-10 reviews detected the low evidence for the use of orthoses in the treatment of OVF, their use was recommended. Two studies determined inconclusive evidence for orthotic use and therefore no recommendation was given.6,11 Hofler and Jones neglected the standard use of orthosis. 12
Five studies did not mention the reason for the repetition of the systematic review.5,9-12 Three authors repeated the review because they detected missing clear recommendations, included further studies or performed statistical analyses.6-8 Six previous reviews used RoB,5-9,12 two the GRADE approach,7,11 and two a meta-analysis7,11 and one study did not perform a qualitative analysis. 9 Meta-analyses7,11 based mainly on the Pfeifer studies.31,32
According to the Oxman and Guyatt index: three reviews had minimal,6,9,11 three some5,7,12 and one with severe weakness. 10 According to the PRISMA Score six reviews were graded low,5,6,8-10,12 each one moderate 7 and high. 11 Except of one review 10 the remaining reviews had SORT grade B.
Discussion
Studies reporting on one orthosis described benefits over time and biomechanically immediately after application.
Liaw et al 30 and Jacob et al 33 showed benefits for gait parameters, decrease of falls and their persistence during follow-up but effects on function, pain and QoL remains unclear because no comparison groups are included. In addition, the orthosis showed a failure rate <25% in terms of bony union.24,27 However, there is no mandatory relation of bony union to the function and QoL.24,27 Most beneficial effects occurred in the first time after applying a spinal orthosis whereas effects after 3 months were rare 27 contradicting observations of other studies.31,32
In terms of the type of orthosis, the data favor soft orthosis or active orthosis like the Spinomed orthosis more than rigid braces based on a determined non-inferiority. Despite spinal orthosis led to a reproducible increase of trunk muscle strength, 34 previous reported improvements on pain and function were not reproducible.31,32 The observed superiority of spinal orthosis was only reported in two studies of the same author.31,32 The comparison of the here applied scores for pain, function and QoL are limited due to the missing use in the remaining studies.31,32 In addition, the authors reported these beneficial effects after delayed treatment (6 months) after inclusion.31,32 Considering the fracture union of >80% after 6 months24,27 may lead to the assumption that spinal orthosis improved osteoporotic related pain but not mandatory fracture related pain.
Here, the used diagnostics in relation to fracture age and thereby fracture related pain of the different studies should be considered. 51 The MRI was only used in six studies and was shown as appropriate diagnostic for OVF. 51 All of them comparing orthosis to no orthosis (n = 225,29) found no significant improvement by the orthosis. In addition, solely three studies25,27,36 used fracture classification systems although they are required guiding therapy and may be used to for the outcome prognosis. 52 Apart from other classification systems, for example the OF classification seems to be an appropriate classification due to the inclusion of the MRI. 53 Considering the performed quality assessment and the thereby identified higher quality studies led to the following conclusions: Comparing orthosis types, a preference for soft or active orthosis compared to rigid braces was found. Nonetheless, the highest quality study 29 showed no inferiority of patients treated without an orthosis compared to patients treated with orthosis though the patient number is limited. A larger study, 25 though with limited quality, supported these findings. Thus, spinal orthoses seem to not significantly improve the outcome of patients suffering from thoracolumbar OVF. Despite previous systematic reviews underline the limited evidence for the application of spinal orthosis and the high risk of bias of the included studies, at least weak recommendations for the application of spinal orthosis were given. At least three of them had only minimal weakness according to the Oxman and Guyatt Index. Thus, the contradicting recommendations given by us might be challenged. Compared to previous systematic reviews we performed a quality assessment and used the obtained results for our recommendations. In contrast, previously the recommendations and meta-analysis are based on two studies31,32 which were here graded with low quality and a high risk of bias. Furthermore, it was not possible to detect if these studies31,32 shared patients’ cohorts as outlined above and a previous review assumed a potential conflict of interest. 11 Therefore, though the reviews were conducted with high quality, their recommendation and analyses were affected by the included studies and the overestimation of two studies caused by their initially planned study design. 54 Currently the evidence regarding the application of spinal orthosis is limited and based on small sample size and/or low-quality studies. Therefore, large multicenter studies considering appropriate diagnostics, the use of therapy guiding classification systems and with power should be carried out. Analyzing the inclusion and exclusion criteria highlight additionally the selective reporting because especially patients with cognitive impairment or neurodegenerative diseases as well as spinal degenerative diseases were excluded but in clinical practice a relevant patient cohort.
Conclusion
After the application of a spinal orthosis pain decreases and QoL improves over time. This is not different to the outcomes of patients treated without an orthosis. Thus, a clear recommendation for the application of spinal orthosis cannot be given. Indeed, this recommendation is predominately based on non-high-quality studies but is based on the grading of the different available studies and caused by the results of a meticulous quality assessment.
Supplemental Material
Supplemental Material - Spinal Orthoses in the Treatment of Osteoporotic Thoracolumbar Vertebral Fractures in the Elderly: A Systematic Review With Quantitative Quality Assessment
Supplemental Material for Spinal Orthoses in the Treatment of Osteoporotic Thoracolumbar Vertebral Fractures in the Elderly: A Systematic Review With Quantitative Quality Assessment by Philipp Pieroh, Ulrich J.A. Spiegl, Anna Völker, Sven Märdian, Nicolas H. von der Höh, Georg Osterhoff, Christoph-E. Heyde; Spine Section of the German Society for Orthopaedics and Trauma in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was organized and financially supported by Deutsche Gesellschaft für Orthopädie und Unfallchirurgie e.V. (DGOU).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.