
Abstract
Background:
Although knee braces are used by individuals with patellofemoral pain syndrome, the effect of patellofemoral bracing on knee flexion during walking has not been elucidated.
Aim:
The purpose of this study was to evaluate the effect of patellofemoral bracing on sagittal plane knee joint kinematics and temporal spatial parameters during walking in individuals with patellofemoral pain syndrome.
Study design:
Quasi-experimental.
Methods:
Ten subjects with a diagnosis of patellofemoral pain syndrome were fitted with a knee brace incorporating an infrapatellar strap. Testing was performed at baseline and after 6 weeks of use. Gait analysis and a visual analog scale were used to assess outcomes in this study.
Results:
A 59.6% decrease in pain was reported by using bracing. Bracing significantly improved speed of walking (p ≤ 0.001) and step length (p ≤ 0.001). The mean cadence was also increased following 6 weeks of patellofemoral brace use, but this was not significant (p = 0.077). Knee flexion angles improved during initial contact, loading response, and mid-swing (p ≤ 0.001) after 6 weeks of patellofemoral brace use.
Conclusion:
Knee orthoses resulted in decreased pain, improved temporal spatial parameters (speed of walking and step length), and increased knee flexion angles during ambulation in patients with patellofemoral pain syndrome.
Clinical relevance
The results of this study demonstrate a positive effect of patellofemoral bracing in improving specific gait parameters and provide evidence to support its use as a conservative treatment.
Keywords
Introduction
Patellofemoral pain syndrome (PFPS) is one of the most frequently observed disorders in runners, sport medicine centers, and orthopedic clinics.1,2 This type of injury is more prevalent in females than males and also in young adults.3–6 PFPS is described as a pain in the anterior aspect of the knee joint that is increased with activities that load the tibiofemoral joint, for example, while running, squatting, climbing, and descending.7,8 Excessive tibiofemoral rotation during stance phase secondary to excessive pronation of the foot and its resultant effects on the knee joint have been demonstrated as a risk factor for development of PFPS.6,9–12
Activity modification, physical therapy, patellar taping, provision of foot orthoses, and patellofemoral bracing have been introduced as conservative methods in the treatment of PFPS. 8 The positive effect of many types of knee brace such as knee sleeves or infrapatellar straps, which are designed to provide centralization of the patella within the femoral sulcus to correct patellofemoral tracking, have previously been reported.13,14 They have been shown to reduce knee pain and improve function and could therefore be a useful form of conservative treatment.15,16
Due to pain in the knee joint, patients with PFPS demonstrate an antalgic gait pattern during ambulation especially when ascending and descending stairs. 3 Anecdotal evidence suggests that reduced knee flexion during stance phase of gait may be observed in patients with PFPS in an attempt to reduce their knee pain by reducing the applied loading through the patellofemoral joint. 3 However, this is not well documented, as most studies have tested knee flexion while ascending and descending stairs; even these studies have demonstrated conflicting results.
In one study, a series of subjects (n = 17) with symptomatic knee joints with either chondromalacia patellae or recurrent subluxation were treated by restricting their affected knee to a maximum of 30° of flexion by application of a knee range of motion (ROM) control brace. 17 Improvements in symptoms were noted after 6 weeks of brace wear compared to a control group. The authors postulated that the improvements in symptoms may have been due to the restriction of knee flexion afforded by the brace. However, it is not clear whether such improvements may be afforded by wearing a less restrictive knee brace continually for a similar period, which supports the patella while offering little or no resistance to knee flexion and extension. Gait velocity, cadence, and stride length may also be reduced in PFPS patients.18–21 However, alterations to the sagittal plane kinematic characteristics of gait, which may be expected in patients with PFPS when using a knee brace during walking activities, are not well documented.
Powers et al. 22 evaluated the immediate effect of patellofemoral bracing on knee flexion between braced and un-braced groups during various activities and demonstrated that knee flexion was increased by approximately 2° during self-selected and fast walking. 22 In another study, Bek et al. 23 assessed the immediate effects of an infrapatellar strap on dynamic pedabarography in patients with unilateral PFPS. Lun et al. evaluated the effectiveness of patellar bracing on pain and knee function of PFPS over a 12-week period. They reported that patellar bracing did not improve the symptoms of PFPS more quickly following a program of leg strengthening but did show that patellar bracing alone could improve the symptoms of PFPS. 24 However, these tests were performed following periods of physical sports activity or long periods of sitting rather than during walking activities.
The mechanism by which knee braces may reduce the pain associated with PFPS and how this affects knee flexion and extension during gait are therefore unclear. It has been postulated that encapsulation and support of the patella via brace wear may increase the surface area of the patella to the sulcus and thus reduce excessive localized loading, as well as stabilizing it in subjects who experience repeated subluxation. 3 This may result in a more efficient knee extensor mechanism and could feasibly reduce pain and the need to reduce knee flexion during loading response.
The evidence to date regarding the effect of knee braces on increasing knee flexion during loading response in subjects with PFPS on purely walking activities is therefore inconclusive when tested over a 6-week period. Increased knowledge of the effect of patellofemoral bracing on the kinematics and temporal spatial parameters of the knee joint in patients with PFPS during ambulation is therefore needed to provide further evidence for introducing this type of intervention to improve walking function. The purpose of this study was therefore to evaluate the effect of patellofemoral bracing on knee joint sagittal plane kinematics and temporal spatial parameters during walking in patients with PFPS over a period of 6 weeks.
Methods
Subjects
Ten patients (six females, four males; age (mean ± standard deviation (SD)) = 36.4 ± 3.71 years, height (mean ± SD) = 179 ± 5.35 cm, and weight (mean ± SD) = 75.7 ± 4.54 kg) who were diagnosed with PFPS for a minimum period of 6 weeks in the orthopedic clinic and six healthy matched subjects according to age, height, and weight participated in this study. The six healthy subjects were recruited to offer normal matched initial baseline data. Inclusion criteria used in selection of the patients included the presence of anterior knee pain associated with resisted terminal knee extension, during stair descent or following a unilateral partial squat. 22 In addition, those subjects with no history of knee ligament injury; surgery on the knee joints; pain in the knee joint that originated from bursae, plica, and the patellar ligament; or neurological and orthopedic impairment that affected their balance were suitable to be included in this study. All patients signed a consent form before participating in this study. Ethical approval was obtained from the ethical committee of Isfahan University of Medical Sciences. All patients were screened by the same physician. The subjects were instructed to wear the knee braces for at least 8 h during the day and did not receive any concomitant treatment during the study period.
Procedure
Pain was evaluated using a visual analog scale (VAS) that ranged from 0 (“no pain”) to 10 cm (“worst pain imaginable”) following the last painful activity. Gait was analyzed by a Vicon digital motion capture system (Vicon 640; Oxford Metrics, UK) using six cameras (Vicon, Infrared) at a frequency of 100 Hz and two force platforms set apart and positioned to capture a left heel and right heel strikes (Kistler 9286BA, Switzerland). Markers were used at the following positions: bilaterally over anterior superior iliac spine (ASIS), the position of the greater trochanter, the lateral condyle of the femur, the anterior aspect of the thigh, the head and lateral malleolus of the fibula, and the head of second and fifth metatarsal and calcaneus. 22 Patients walked with their self-selected speed along a 6 m walkway. Data gathered from four walking trials were analyzed for each volunteer subject.
Patients were fitted with a suitably sized knee brace (8387 Genu Therma Combi; Otto Bock Company, Germany), which incorporated an infrapatellar strap (Figure 1). The brace was chosen because it had an infrapatellar strap that could be used on all patients to control the position of the patella. The orthosis utilized the infrapatellar strap to act as a “U”-shaped support to control the position of the patella mediolaterally. After 6 weeks of using the orthosis, gait analysis was performed, and pain levels were again assessed when patients walked without the brace.

The knee orthosis used in this study.
The purpose of this study was to evaluate the effect of using orthotic intervention in the form of a patella control brace on knee flexion and temporal spatial parameters when walking. Patients were initially evaluated without the brace in the gait laboratory prior to wearing the knee brace for 6 weeks, after which time the same testing protocol was followed without the brace in situ to enable a direct comparison to be made on the primary outcome measures (Figure 2).

Patient evaluation in the gait laboratory.
Statistical analysis
Normality of data was confirmed by using the Kolmogorov–Smirnov technique. According to the normality of data, a paired t-test was used for analyzing the effects of the within-subjects design before and after intervention. SPSS statistical software was used for the analysis of data. The level of significance was set at 0.05.
Results
Pain
A reduction in the VAS pain scores following 6 weeks of using the patellofemoral bracing was shown in this study, resulting in a mean of 59.6% in reduction in pain levels (Table 1).
Mean ± SD of spatial–temporal gait parameters in baseline and after 6 weeks of using patellofemoral bracing.
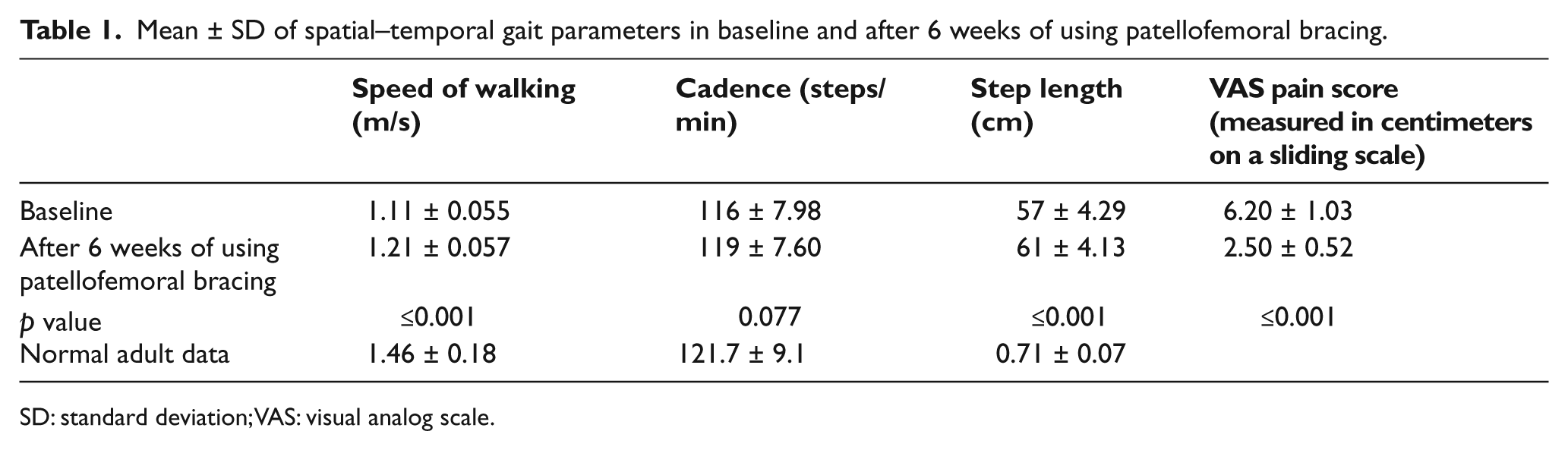
SD: standard deviation; VAS: visual analog scale.
Spatial–temporal gait parameters (speed of walking, step length, and cadence)
As shown in Table 1, the mean walking speed following 6 weeks of patellofemoral brace use (1.21 ± 0.057 m/s) was significantly improved (p ≤ 0.001) compared to the baseline situation (1.11 ± 0.055 m/s). The mean cadence was also increased following 6 weeks of using patellofemoral bracing, but this was not significant (p = 0.077); however, step length was significantly increased (p ≤ 0.001) compared to the baseline (Table 1).
Knee angles
In analyzing knee flexion angles, individuals demonstrated significantly greater knee flexion during initial contact, loading response, and mid-swing after 6 weeks of patellofemoral brace use compared to baseline (Table 2). However, while being statistically significant, they were clinically nonsignificant, as they were less than the accuracy afforded by the measurement system (±1°).
Mean ± SD of knee angle in baseline and after 6 weeks of using patellofemoral bracing.
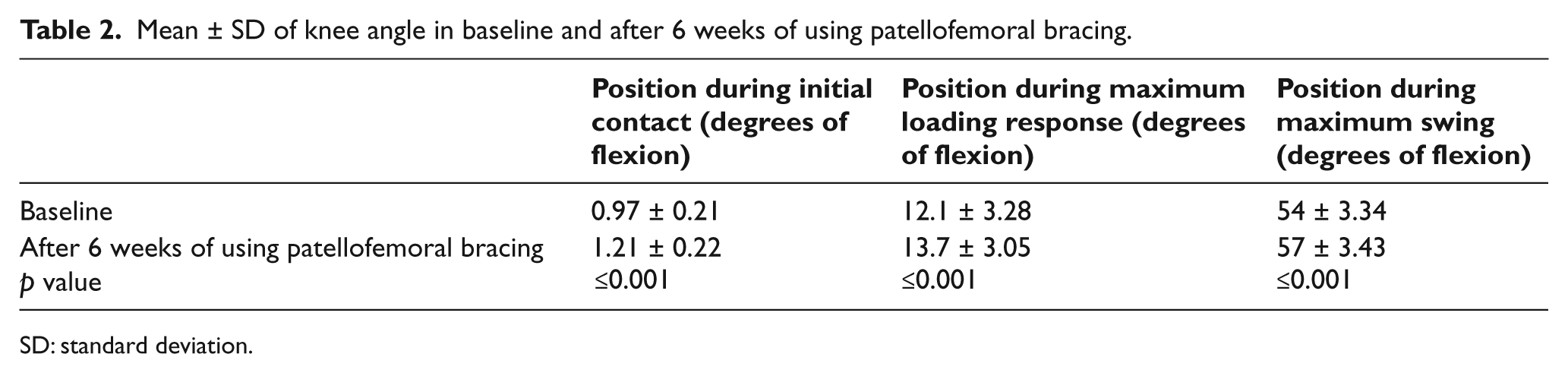
SD: standard deviation.
Discussion
Conservative management is usually considered as an initial approach in the treatment of PFPS, and the use of patellofemoral bracing is one conservative treatment method. A systematic review in this field by Warden et al. 25 reported limited evidence for the use of patellofemoral bracing in patients with PFPS. Other studies investigating the effects of different types of patellofemoral bracing have also demonstrated limited clinical or biomechanical evidence for wearing this type of brace for the treatment of PFPS.24,26
The main findings in this study were a significant reduction in the mean VAS pain scores following 6 weeks of patellofemoral bracing use along with a faster walking speed, increased knee flexion angles, and a greater step length compared to the baseline situation. The mean cadence was also increased, indicating that an increased confidence in walking may have been achieved.
The use of patellofemoral bracing reduced knee pain in this study by 59.6%, although the reduction of pain has been reported as being 44%–78% using a taping technique.27–29 Similar findings have been demonstrated when using knee orthoses,30,31 but Powers et al. 22 reported contrary findings. Walking speed, cadence, and step length have all been shown to be decreased in patients with PFPS compared to that demonstrated in healthy subjects,18,22 but within 6 weeks of using the brace, the temporal spatial parameters of walking were significantly improved for subjects in this study. Reduction of pain may have produced these results and improved gait function. The improvements in gait characteristics demonstrated in this study were similar to the findings of previous studies in this field when using tape instead of a knee orthosis. Powers et al. 29 demonstrated increase in knee flexion angles and speed of walking during level walking when using taping, and Ernst et al. 31 reported increase in peak knee extensor moment after using patellar taping. However, Powers et al. 22 demonstrated no significant differences in pain, torque, and gait function in immediate effect of patellofemoral bracing in females with PFPS.
The mean knee flexion at heel strike is reduced in subjects with PFPS compared to that published for healthy subjects.20,32,33 Reduction of knee flexion angle during initial contact is performed by patients with PFPS in an attempt to decrease the load on the patellofemoral joint and reduce pain. 34 In this study, following 6 weeks of patellofemoral bracing use, this parameter was improved, albeit nonsignificantly.
Knee braces and sleeves are designed to correct the position of the patella in the sulcus and to alter patellar tracking. The external supportive and corrective structure may have been responsible for providing the positive effects on gait parameters shown in this study. Patella bracing is usually used to prevent lateral dislocation of patella and to stabilize the knee during ambulation. 18 A previous study has demonstrated an additional positive thermal effect when using knee bracing along with increased sensory feedback and alteration to the circulation of the knee joint. 14
The patellar bracing used in this study incorporated an infrapatellar strap in its design. In addition to the benefit from adding resistance to dislocation of the patella during physical activity, the infrapatellar strap may have applied pressure to the patellar tendon and theoretically altered its line of action and therefore may have stabilized the patella.
There were several limitations in this study. Only level walking was analyzed in this study. Evaluation of this orthosis in stair climbing and descending should also be performed in a further study. In addition, only one type of brace was analyzed, and comparison between other designs of knee brace, foot orthoses, and a knee sleeve incorporating an infrapatellar strap could prove beneficial to detect and compare effective conservative approaches in the treatment of patients with PFPS or indeed a combination of them. A habituation effect of brace wear over the 6-week period may also have occurred. This study utilized a small sample size (n = 10), and brace compliance was not recorded or monitored during the study.
Conclusion
During in level ambulation, a knee brace resulted in decreased pain, increased temporal spatial parameters (speed of walking and step length), and increased knee flexion angles in subjects with PFPS. Therefore, this type of brace may be used as an effective conservative method in improving the gait of patients with PFPS.
Footnotes
Conflict of interest
The authors have no conflict of interest in this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.