
Abstract
Background and aim:
If a person does not become ambulant after an amputation, a knee disarticulation (KD) shouldbe considered and the person may then benefit from a cosmetic KD prosthesis. The features of a cosmetic KD prosthesis are, however, seldom described. The aim of this clinical note is to describe the development of a cosmeticKD prosthesis.
Technique:
A non-ambulant person with bilateral KD formulated, together with her physiatrist, the criteria for a cosmetic KD prosthesis. On the basis of these, a lightweight, natural-looking, well-fitting, easy-to-put-on and take-off KD prosthesis, with no thigh lengthening during sitting, was made. This prosthesis was fixed on a wheelchair and does not impede transfer.
Discussion:
A newly constructed cosmetic prosthesis for non-ambulant persons with a KD is described in detail. We hope that this will encourage physiatrists and prosthetists to offer non-ambulant persons with a KD a cosmetic prosthesis.
Clinical relevance
A cosmetic leg prosthesis with good cosmetic properties, good sitting comfort, and no restrictions in making transfers is described in detail for non-ambulant persons with a knee disarticulation.
Background and aim
After a lower-limb amputation, 50% of patients will not use a prosthesis.1,2 A (functional) prosthesis is currently generally not prescribed if the patient had already been non-ambulant before amputation, or is judged to be incapable of using a prosthesis.
If a patient cannot use a (functional) prosthesis after amputation, a knee disarticulation (KD) may be the preferable level of amputation.3,4 The alternative of a transtibial amputation has no functional advantages compared with a KD, and often results in a flexion contracture of the knee. 5 The alternative of a transfemoral amputation results, compared with a KD, in a decrease in sitting balance, especially if muscular imbalance causes flexion contracture in the hip.6,7
The requirements for a KD prosthesis differ between ambulant and non-ambulant persons. For ambulant persons, a standard KD prosthesis consists of a (open) socket, a knee device with an anchor (to connect this knee device to the socket), a shank with a cover, and a prosthetic foot. The socket is constructed to allow suspension on the stump as well as end-bearing. The knee device is constructed to create stability in stance phase, control in swing phase when walking, and for flexibility when sitting. Moreover, due to the positioning of the knee distally to the femur condyles, when sitting, lengthening of the thigh occurs, and as a consequence, shortening of the shank. 8 This hampers sitting in confined spaces, such as cars or theater seats. For non-ambulant persons with a KD most of these features are, however, irrelevant. They prefer no prosthesis at all, or a cosmetic prosthesis to regain their body image. In such cases, a cosmetic prosthesis should look like a natural leg.
Descriptions of cosmetic prostheses are rare. The only description we are aware of is from Germany. 9 The authors in that study described a flexed transfemoral prosthesis where the prosthetic foot was fixed on the footboard of the wheelchair. The aim of this study was to develop and describe a cosmetic prosthesis for a non-ambulant KD amputee.
Technique
Participant
This clinical note is based on an 87-year-old woman (the patient), weighing 70 kg, who had a right KD a year ago, due to vascular disease with diabetes, and a recently performed left KD. After her first (right) KD, she was wheelchair bound. She was judged incapable of using KD prostheses functionally after her left KD. She wished to wear prostheses for cosmetic purposes. Written informed consent was obtained from the patient. The medical ethics committee of the local hospital ruled that a formal application and approval was not required for this clinical note.
Prosthetic considerations
Before designing the KD prosthesis, the patient formulated design criteria in cooperation with her physiatrist. The prosthesis had to:
Look like a natural leg;
Have a good and comfortable fit with the stump, with no transpiration;
Have no thigh lengthening during sitting, in order to prevent bumping her knees while maneuvring with her wheelchair;
Be easy to put on and take off;
Create no impediment during transfers;
Be lightweight;
For health insurance purposes, be relatively cheap.
Description of the cosmetic KD prosthesis
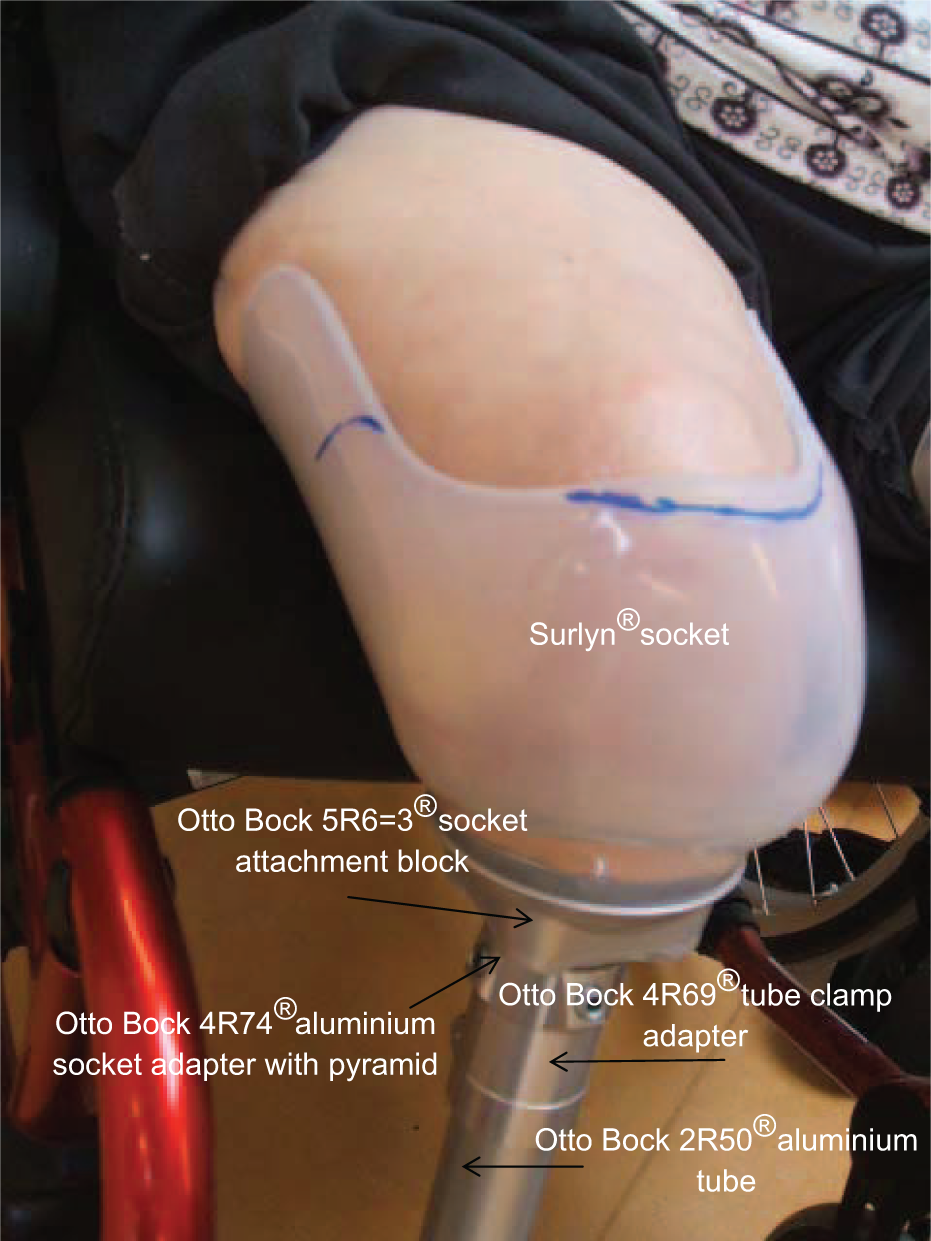
The KD prosthesis we designed is shown in Figures 1 and 2. To create a natural-looking leg, the shank was covered with urethane foam 10 and a natural-colored stocking. To create a good and comfortable fit and no thigh lengthening of the stump during sitting, we placed the socket directly on the shank of the prosthesis, with no knee mechanism. Moreover, we created a short socket, just covering the condyles, to prevent transpiration, with little distal suction of the cup, to ensure a good fit. The socket is closed only distally on the ventral side, to prevent the stump from moving upward out of the socket (Figure 2).
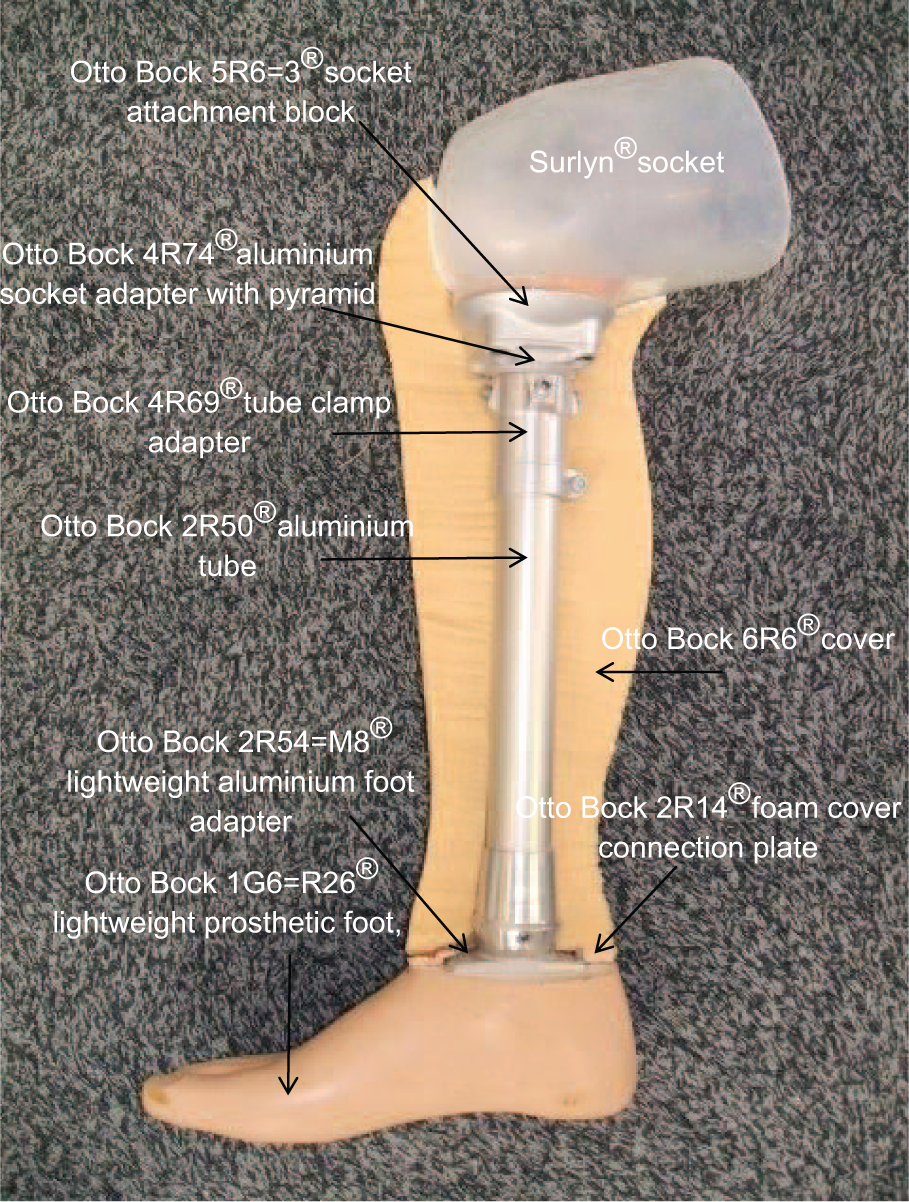
Cosmetic KD prosthesis, sagittal view.
Cosmetic KD prosthesis, frontal view without cover.
The foot of the cosmetic prosthesis was fixed onto the footboard of the wheelchair by Velcro strips. The plusher (loop) side was attached to the bottom of the heel of the shoe so that the prosthesis does not stick if placed on the carpet. The hook side of the Velcro strip was attached to the footboard of the wheelchair (Figure 3). In this way, little movement (play) of the proximal part of the prosthesis is possible, allowing the patient to don and doff the cosmetic prosthesis by pressing or pulling the socket to her stump. The footboards were able to rotate laterally, permitting the patient to transfer without her prostheses.

Fixation of the shoe of the cosmetic KD prosthesis on the footboard of the wheelchair by Velcro strips.
When the patient is wearing a skirt or a dress, she can simply use this to cover her prosthesis. Trousers can be pulled on over the prosthesis, with the prosthesis fixed on the footboard and the trousers being pulled on (when sitting), in the same way as someone with no prosthesis.
The patient was happy with her KD prostheses, especially that they looked like natural legs. The feedback for further improvement was twofold: first, that it was initially difficult for her to use the Velcro strips in a proper way, and second, that the prostheses on the wheelchair made some people think of her as being able to transfer and even to walk, thus creating confusion about her mobility.
The components of the cosmetic KD prosthesis and a functional KD prosthesis are shown in Table 1. Compared with standard prosthetic components, there is about a 685 g overall weight reduction: 485 g due to the absence of a knee mechanism and about 200 g due to light components. The cosmetic KD prosthesis is three times cheaper than a functional KD prosthesis, mainly because of the absence of the knee device. The manufacturing time of the cosmetic KD prosthesis is half that of a functional KD prosthesis, mainly because of the reduced time required to fit the socket and to align the socket with the shank.
Comparison of the components of the cosmetic KD prosthesis and a functional KD prosthesis.
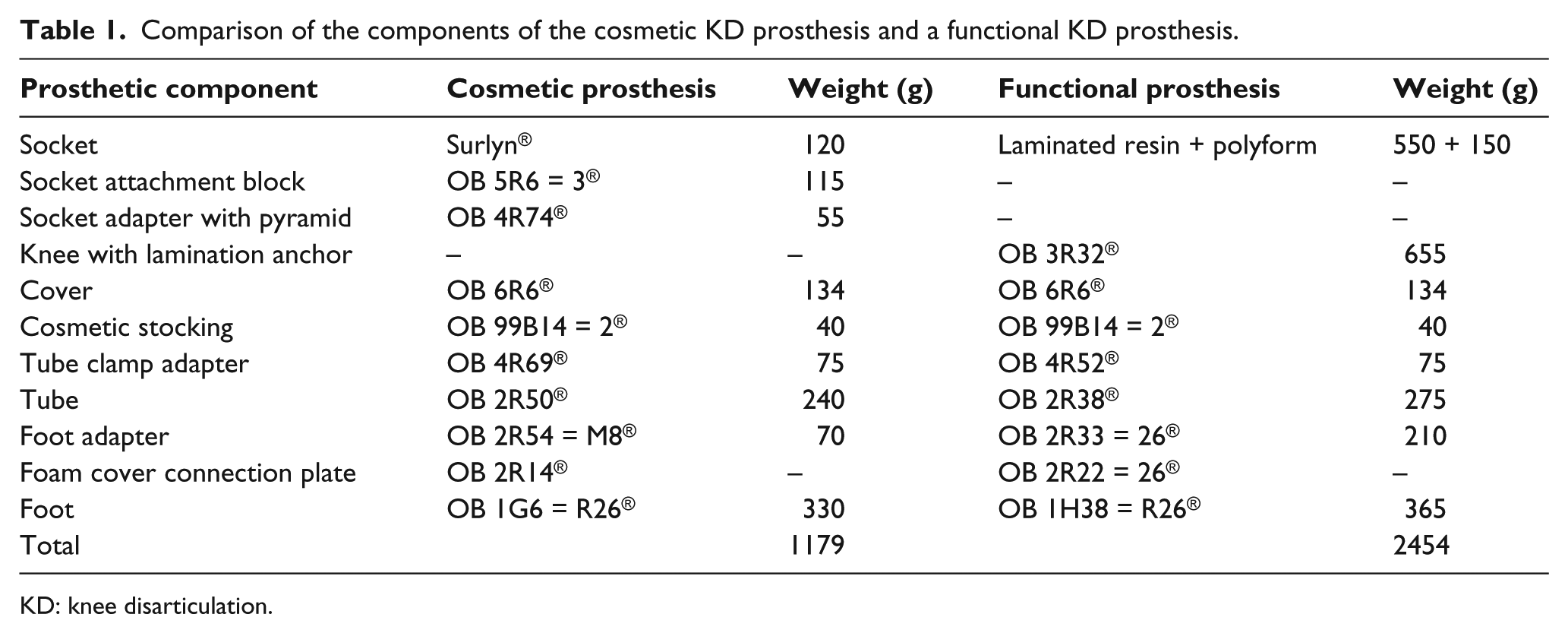
KD: knee disarticulation.
Discussion
This clinical note describes a cosmetic prosthesis for a non-ambulant KD amputee. The cosmetic KD prosthesis looks like a natural leg, has a good and comfortable fit because it is fitted with only a distal cup; has no thigh lengthening because it has no knee mechanism; can be put on and taken off easily; is fixed on the footboard of a wheelchair, and because of the possibility of rotating this footboard, transfers are easy; and is lighter. This latter statement is because of the absence of a knee mechanism and, second, because of the lightweight foot. This cosmetic KD prosthesis is cheaper than a functional KD prosthesis.
Design criteria for a cosmetic leg prosthesis are unknown. For a arm prosthesis, the most desired criteria are lightness, good fit, minimal transpiration problems, acceptable costs, and good appearance under clothing. 11 With the exception of easy transfers, these criteria are in accordance with the design criteria formulated by the patient in cooperation with her physiatrist. Being lightweight was less important, as we fixed the cosmetic KD prosthesis onto the footboard of the wheelchair. Additionally, in order to don and doff the cosmetic KD prosthesis easily, the prosthesis has to be tiltable around the footboard in order to place the cup at the end of the stump. It is therefore recommended that the KD prosthesis be light, especially on the proximal side.
Most principles of the cosmetic KD prosthesis can be applied to a cosmetic transfemoral prosthesis. However, a simple, single-axis knee mechanism has to be used, allowing some movement in order to push the socket to the stump when being donned. There is a urethane foam cover from the socket to the foot, which also covers the knee.
We are not aware of studies that have examined body image when a cosmetic prosthesis is used, although aspects of body image in persons with a lower-limb amputation can be measured with the revised Amputee Body Image Scale (ABIS). 12 Perhaps the unfamiliarity with cosmetic prostheses, the rarity of their descriptions, and the non-reimbursement by some health insurance companies play roles in this.
A limitation of this case (clinical note) is that, by discussing the possibility of being fitted with a cosmetic prosthesis, in conjunction with the participant, we were not able to assess the impact of the regaining of the body image without bias. In the future, we recommend that further investigation is concentrated on the impact of a cosmetic KD prosthesis and its effect on body image.
In conclusion, a cosmetic KD prosthesis was described for a non-ambulant patient. A key point of this cosmetic KD prosthesis is the absence of a knee mechanism. Therefore, there is no thigh lengthening during sitting, resulting in a more natural look. This also reduces the weight and cost of the prosthesis. Moreover, the fit of the cosmetic KD prosthesis, with a simple short cup, gives greater sitting comfort, less transpiration, and easier donning and doffing. Also, the cosmetic KD prosthesis does not impede transfer, as it is fixed on the wheelchair. We hope that this clinical note will encourage physiatrists or prosthetists to discuss cosmetic prostheses with non-ambulant amputees.
Key points
This clinical note is the first to describe a cosmetic KD prosthesis in detail.
In contrast to a functional KD prosthesis, the cosmetic KD prosthesis has no thigh lengthening during sitting, due to the absence of a knee mechanism.
The cosmetic KD prosthesis can be put on and taken off easily, and transfers are easy without the prosthesis.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.