
Abstract
Background:
Dysvascularity is the main cause of lower limb amputations in Scotland, and there is an insignificant proportion (1.7%) of knee disarticulations, despite the benefits of amputation.
Objectives:
The outcomes of knee disarticulation and its associated surgical techniques will be evaluated based on healing, reamputations, functional outcomes, prosthetic ambulation and gait biomechanics to determine whether a greater rate of knee disarticulations can be justified among dysvascular patients.
Study design:
Systematic review.
Methods:
Key electronic databases were searched for the relevant literature based on a pre-specified eligibility criterion.
Results:
The 17 articles included in this review were appraised for their quality, and key findings are extracted.
Conclusion:
Healing rates are favourable, but there is a need for appropriate amputation level selection to prevent reamputations. Knee disarticulation patients have better maintenance of independent living status than transfemoral patients, but overall prosthetic ambulation rates are inconsistent. In terms of gait biomechanics of knee disarticulation, there are some positive indications, but the evidence is insubstantial. A stronger body of evidence is required in this subject field, and recommendations are made for future research – Scottish Intercollegiate Guidelines Network Grade of Recommendation: C.
Clinical relevance
This review aims to inform the multidisciplinary teams involved in the rehabilitation of dysvascular amputees about evidence-based outcomes following knee disarticulation. This knowledge will be beneficial when formulating treatment pathways for this vulnerable population group.
Keywords
Background
The rate of knee disarticulations (KDs) has frequently been disproportionally lower than transfemoral amputations (TFAs), although they have greater functional outcomes. The dysvascular amputee population usually consists of elderly patients with comorbidities and minimal rehabilitation potential. 1 They are ideal candidates to benefit from the additional functionality of KD, but this is often avoided by the amputating surgeon due to wound-healing complications. However, there are studies indicating positive results following KD, with some authors recommending different surgical techniques.
Demographics
Dysvascularity is the main cause (84%) of lower limb amputations in Scotland, including diabetes and peripheral arterial disease without diabetes. 2 KD consists of only 1.7% of lower limb amputations, which is highly disproportional compared to transfemoral (TF) (40.6%) and transtibial (TT) (56.6%) levels. 2 These are depicted in Figure 1 and Table 1.
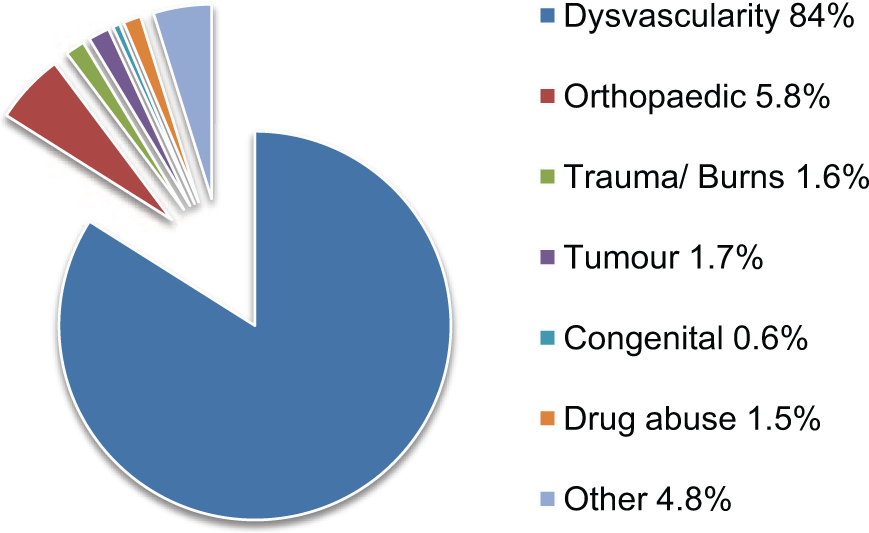
Aetiology of lower limb amputations in 2011.
Levels of amputation in 2011.
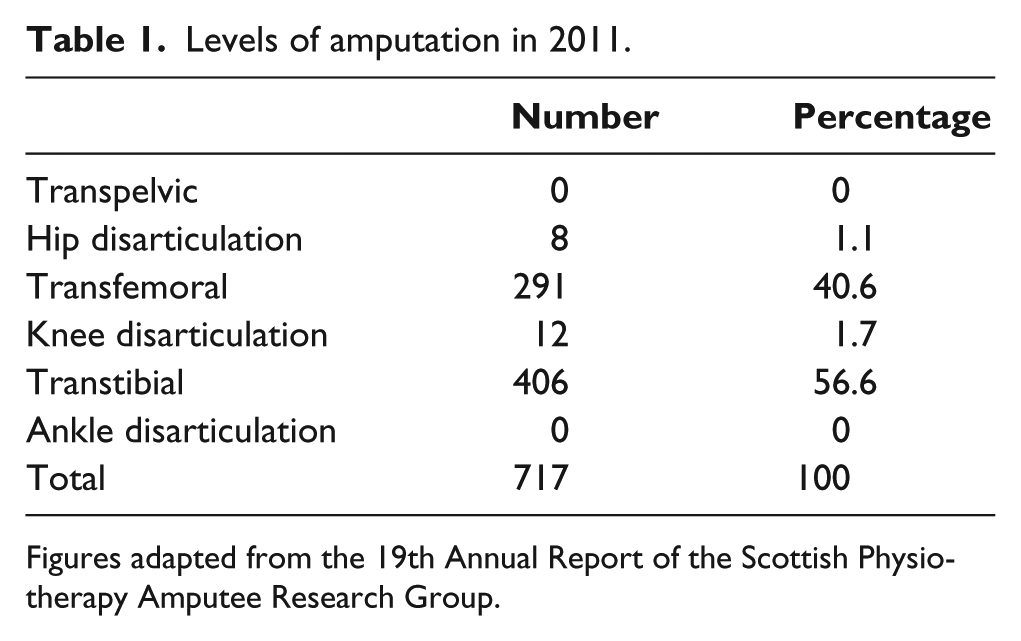
Figures adapted from the 19th Annual Report of the Scottish Physiotherapy Amputee Research Group.
Advantages and disadvantages
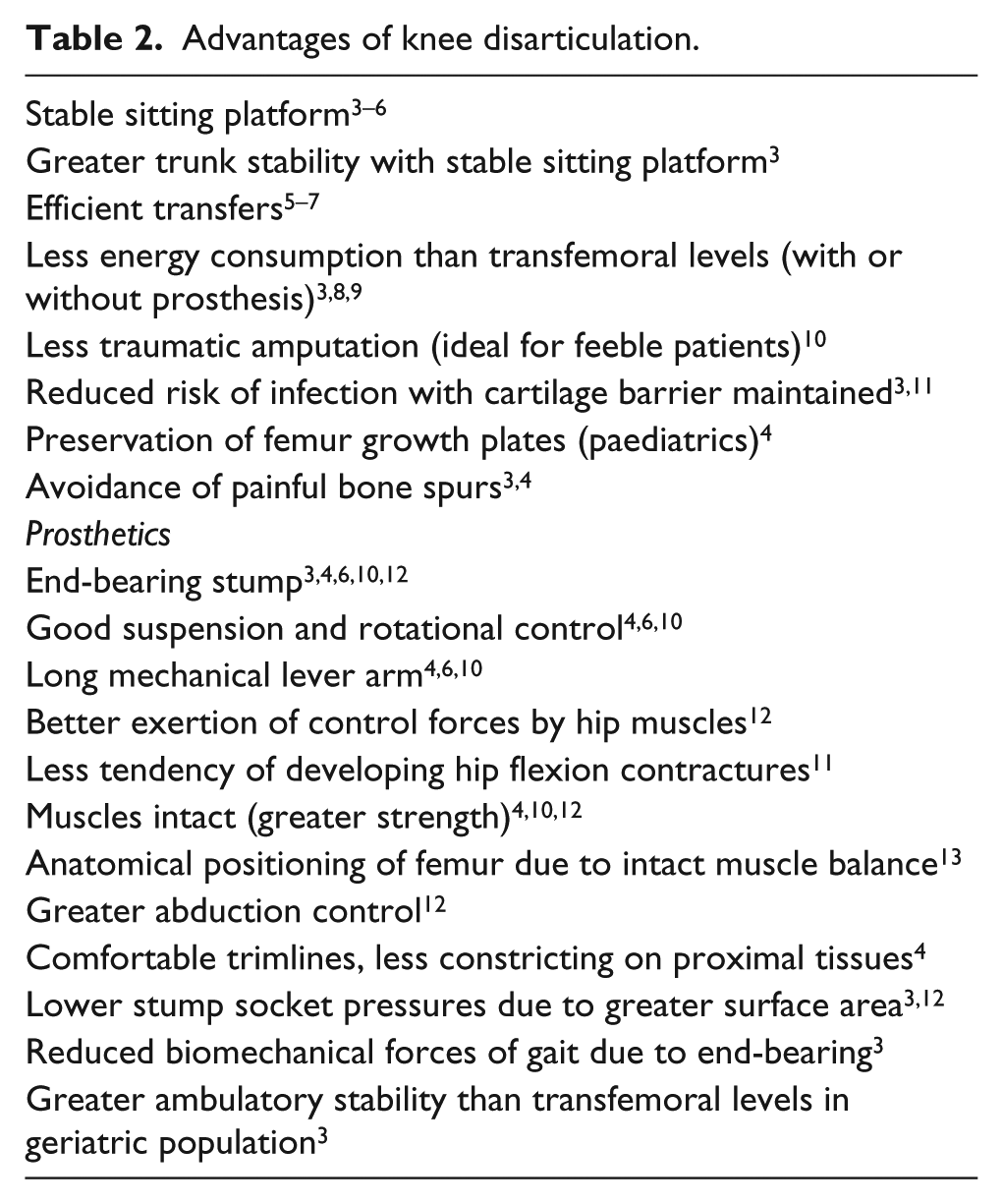
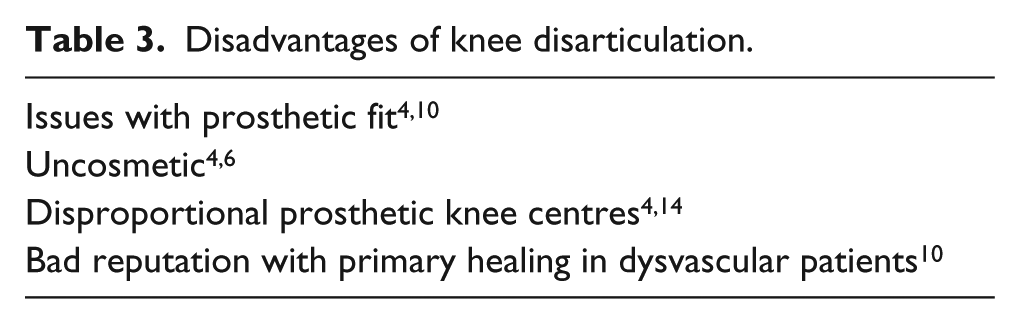
There are many known advantages and disadvantages of KD, listed in Tables 2 and 3, respectively. For dysvascular patients, the tissue viability required for stump healing is similar to the TT level, 3 but KD can be indicated for the reasons listed in Table 4. Transtibial amputations (TTAs) often have risks of knee flexion contractures and stump necrosis for bedbound patients, 15 as the contractures often cause pressure ulcers. 3
Advantages of knee disarticulation.
Disadvantages of knee disarticulation.
Indications of knee disarticulation.
Surgical techniques
KD was unpopular due to poor prosthetic fitting skills, poor healing 10 and poor flap interface consisting of only skin and subcutaneous tissue. 3 The long anterior flap was a standard technique historically,16,17 usually leading to flap necrosis16,18 and reamputations,10,16 and was not recommended for dysvascular patients.16,18 Equal sagittal flaps were advocated by many, with better outcomes10,16,19–22 and a more reliable blood supply than anterior flaps. 21 The minimised flap lengths are ideal for dysvascular patients. 20 Suture lines lay posteriorly in the intercondylar region avoiding the weight-bearing area,16,21,22 with the use of gastrocnemius bellies to enhance end-bearing 20 and preserve blood supply. 10 Skin tension can be avoided with circular incisions and trimming to sagittal flaps before suturing. 21 When the long posterior myofasciocutaneous flap incorporating the gastrocnemius bellies was introduced, 23 it provided excellent padding and blood supply.11,15,23 It was ideal for prosthetic rehabilitation, 15 prevented flap necrosis 23 and was claimed to have better outcomes than sagittal flaps. 11
Mazet and Hennessy 24 introduced another technique to reduce bulkiness of the KD stump by trimming medial, lateral and posterior condyles, and patellectomy. Burgess 25 modified the technique to remove 1.5 cm of the distal end additionally, raising the prosthetic knee joint centre. The shorter flaps required allow improved healing24,26 while still retaining an end-bearing stump.26,27 However, there were authors who condemned this technique due to the reduced weight-bearing area,10,18 impaired suspension,3,18 risk of stump breakdown,5,10,18 and potential haematoma and infection from the bleeding bone. 10
The Gritti–Stokes technique involves using the patella and surrounding tissues as an osteoplastic flap for end-bearing 28 by fixing the patella to the distal end of femur after a transcondylar amputation. 29 The femur is bevelled posteriorly to prevent the patella from slipping.16,30 Published reports indicated better healing rates16,30–34 and an end-bearing stump,30,32 while other authors disputed that it created high peak pressures3,10,16 and had risks of failure at the condylar–patella union.3,10
Objectives
The proportion of KDs does not correspond with the apparent advantages of KD and the claimed benefits of different surgical techniques. This review will aim to evaluate the outcomes of KD based on healing, reamputations, functional outcomes, prosthetic ambulation and gait biomechanics to determine whether a higher rate of KD can be justified among dysvascular patients.
Methods
Protocol
The methodology of the review was pre-specified and documented, adapting the structure of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 35 Studies were graded according to the Scottish Intercollegiate Guidelines Network (SIGN) 50 guidelines. 36
Eligibility criteria
Studies were picked based on the criteria listed in Table 5. Mortality was excluded from the outcome measures as it was mainly influenced by age, physical status and comorbidities and not directly influenced by amputation surgeries.37–40 Higher mortality rates of patients with proximal amputations are generally due to poorer health conditions than patients with distal amputations. 41
Eligibility criteria.
Information sources
Studies were identified by searching electronic databases and scanning the reference lists of included studies. Journals with the most relevant results were handsearched additionally to ensure a thorough search process, but this was only done for the recent publications. These are listed in Table 6. The last search was conducted on 3 April 2014, and the full search strategy including search terms is shown in online Appendix A.
Information sources.
Study selection
The first author (T.M.) performed the eligibility assessment independently, and studies that require difficult judgments of selection/rejection were discussed with the project supervisor (K.M.). Due to the nature of the project, there was a lack of multiple expert reviewers and arbitration in the study selection; hence, there cannot be a complete avoidance of biasness.
Data collection process
A data extraction template was developed and pilot-tested on three randomly selected included studies and refined by K.M. The data extraction was then conducted by T.M. and reviewed by K.M. Any disagreements were resolved by discussion. The completed data extraction is found in Table 7.
Summary of studies.
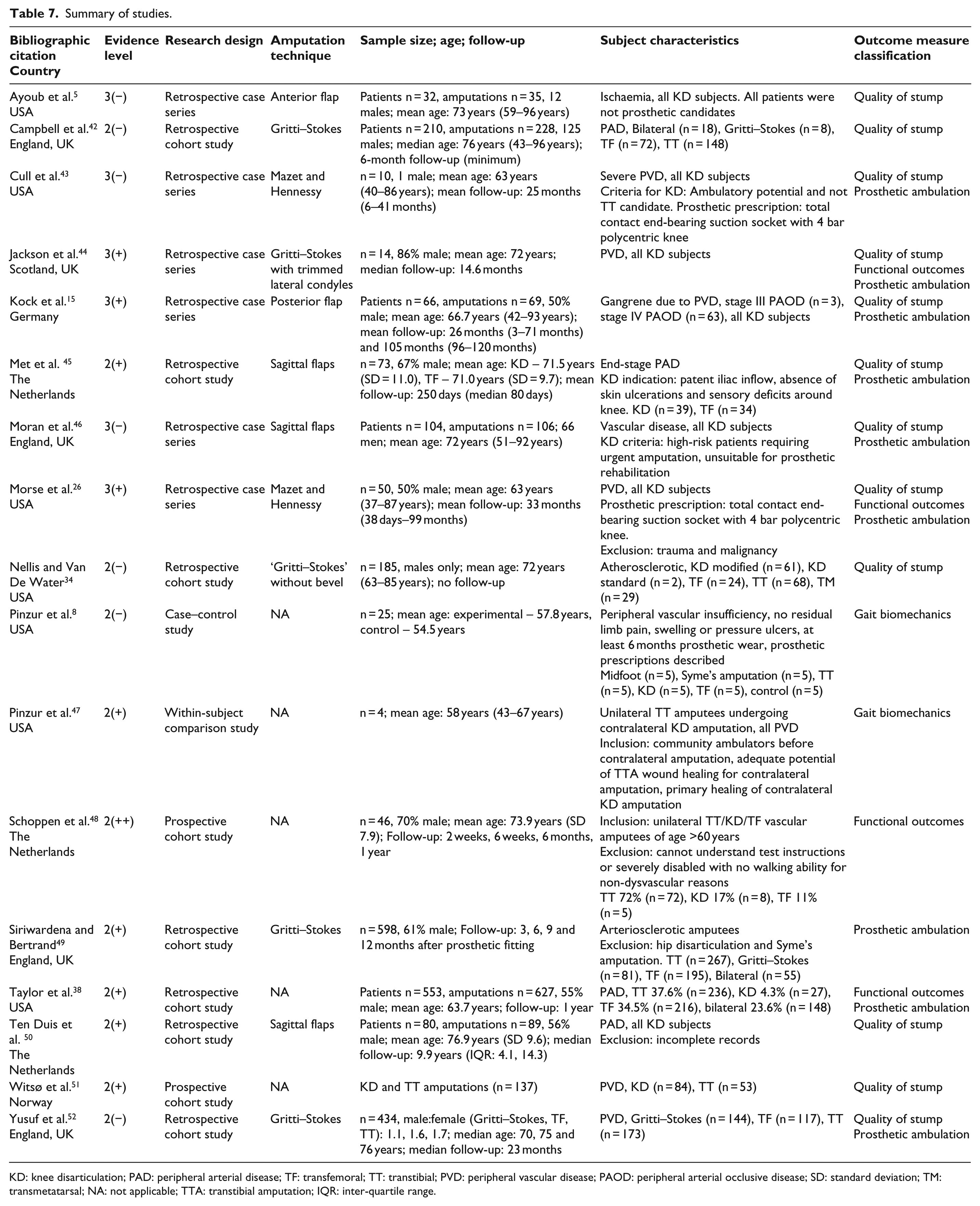
KD: knee disarticulation; PAD: peripheral arterial disease; TF: transfemoral; TT: transtibial; PVD: peripheral vascular disease; PAOD: peripheral arterial occlusive disease; SD: standard deviation; TM: transmetatarsal; NA: not applicable; TTA: transtibial amputation; IQR: inter-quartile range.
Risk of bias
Risk of bias was evaluated using a self-developed checklist (online Appendix B), modified from the SIGN 50 Methodology checklist, 36 to account for factors pertinent to this review. The checklist helps to determine the level of bias present in a study, and a methodological quality grading is given (++ very low risk, + low risk, − high risk). The study design and quality grading given will determine the level of evidence provided by the study, according to the SIGN 50 guidelines. 36
Results
Study selection
A total of 17 studies were identified for inclusion in this review. The selection process is depicted in Figure 2, and key characteristics of the selected studies are listed in Table 7. No studies were found that measured quality of life among KD amputees, and hence this outcome measure was removed.
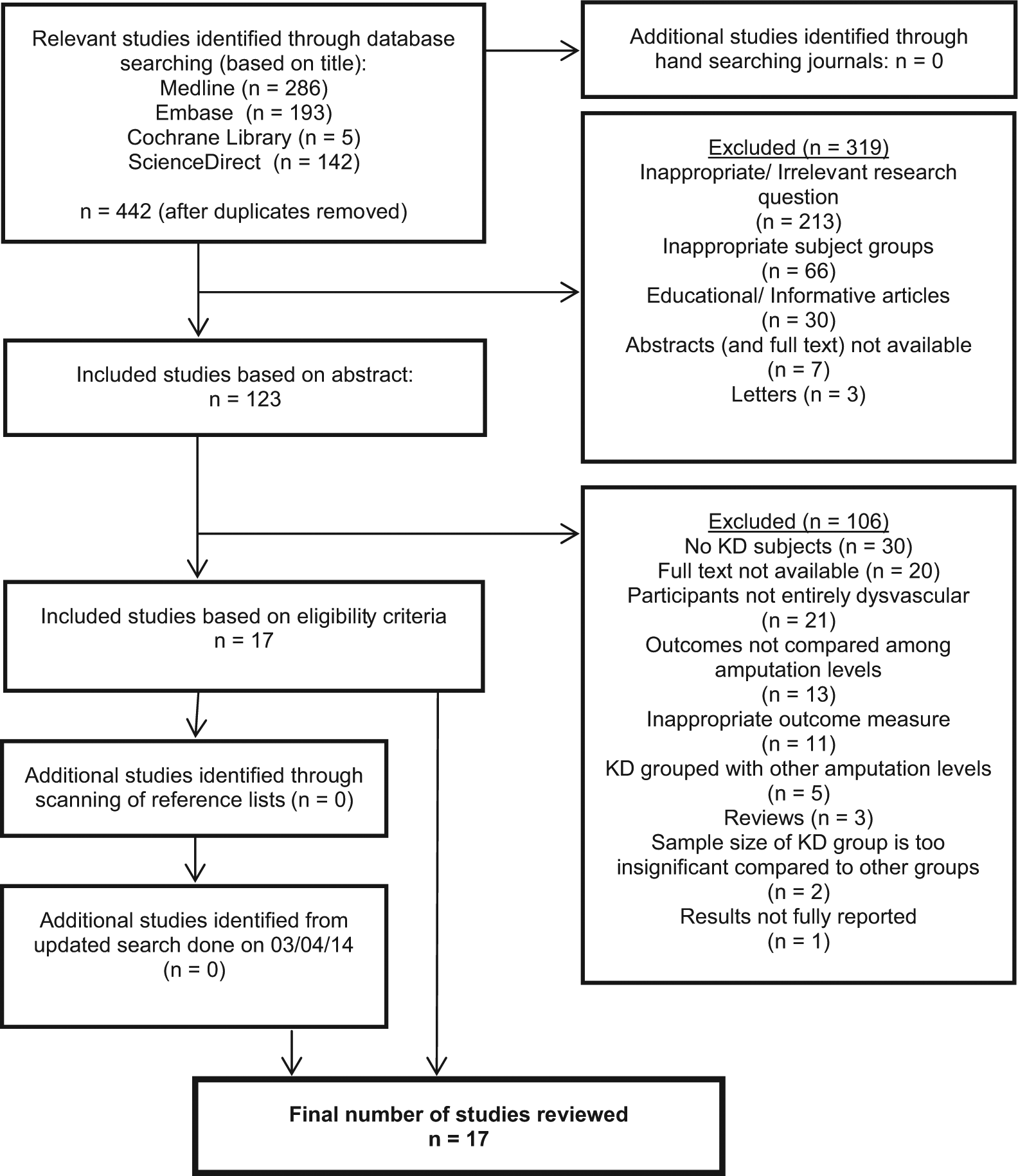
Study selection process.
Quality appraisal
The proportion of studies according to study designs and risk of bias are depicted in Figures 3 and 4, respectively. Specific quality appraisal of each study is shown in online Appendix C. The study designs and the risk of bias will together determine the level of evidence of the studies, which are listed in Table 7. There were no controlled trials found (level 1), with 11 observational studies (level 2)8,34,38,42,45,47–52 and 6 non-analytical studies (level 3).5,15,26,43,44,46 Seven studies had a high risk of bias (−),5,8,34,42,43,46,52 eight studies had a low risk of bias (+)15,26,38,44,45,47,49–51 and only one study had a very low risk of bias (++). 48 Most of the studies were retrospective with only four prospective studies,8,47,48,51 and it was due to the retrospective nature that a higher quality grading (++) could not be given in four other studies.38,45,49,50
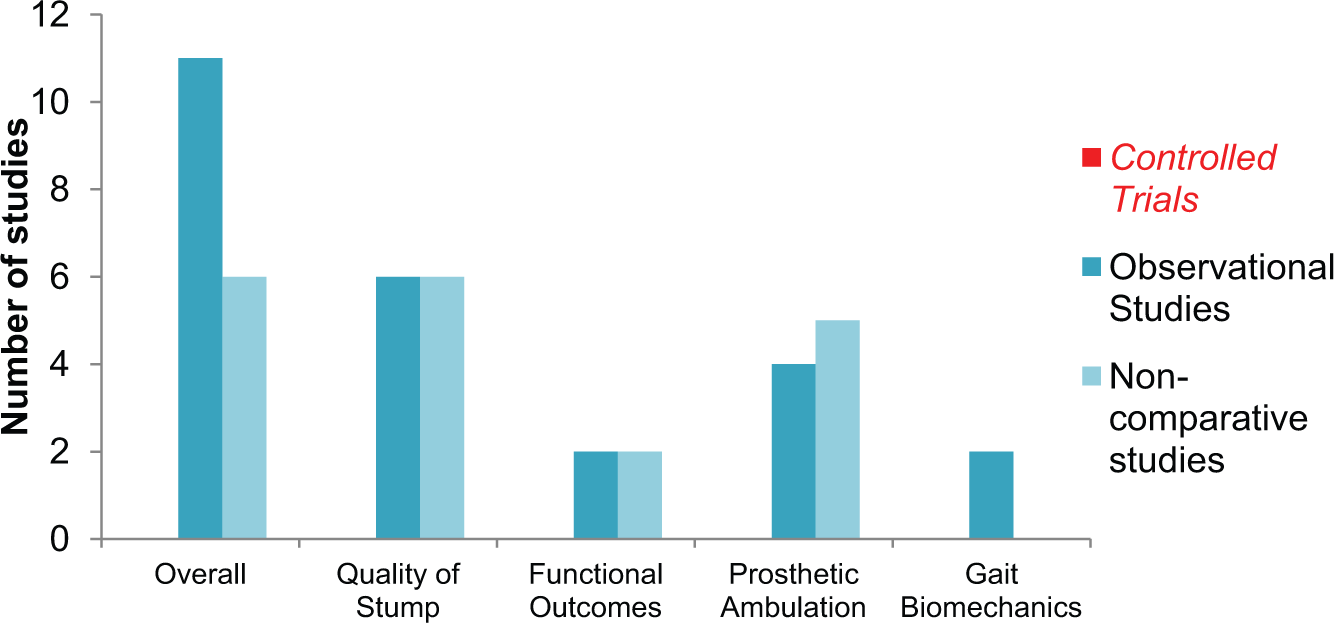
Distribution of studies by study design.
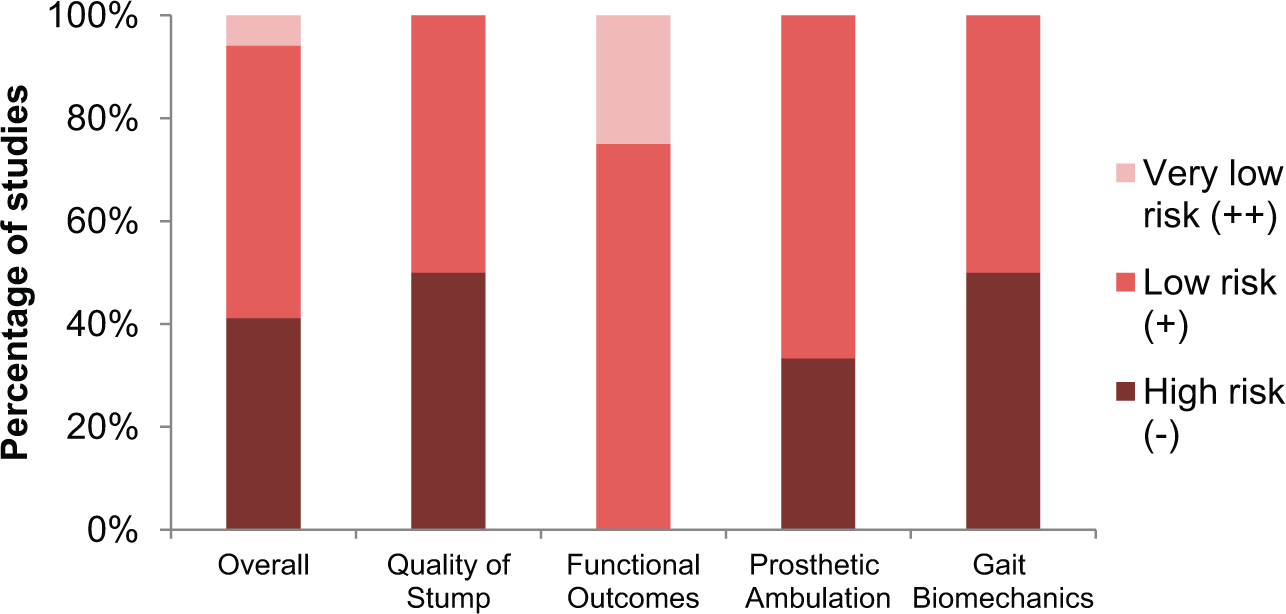
Distribution of studies according to the risk of bias.
Quality of stump
A summary of results for the quality of stump is listed in Table 8. In total, 12 studies reported on the quality of stump, with a total of 709 KD amputations; however, data pooling was not possible due to heterogeneous samples. Primary healing ranged between 60% and 100%, delayed healing/revision was between 0% and 26% and reamputation was between 0% and 21%. Gritti–Stokes had lower reamputation rates ranging between 0% and 13%; no other distinct observations can be made between techniques or countries.
Summary of results for quality of stump in KD.
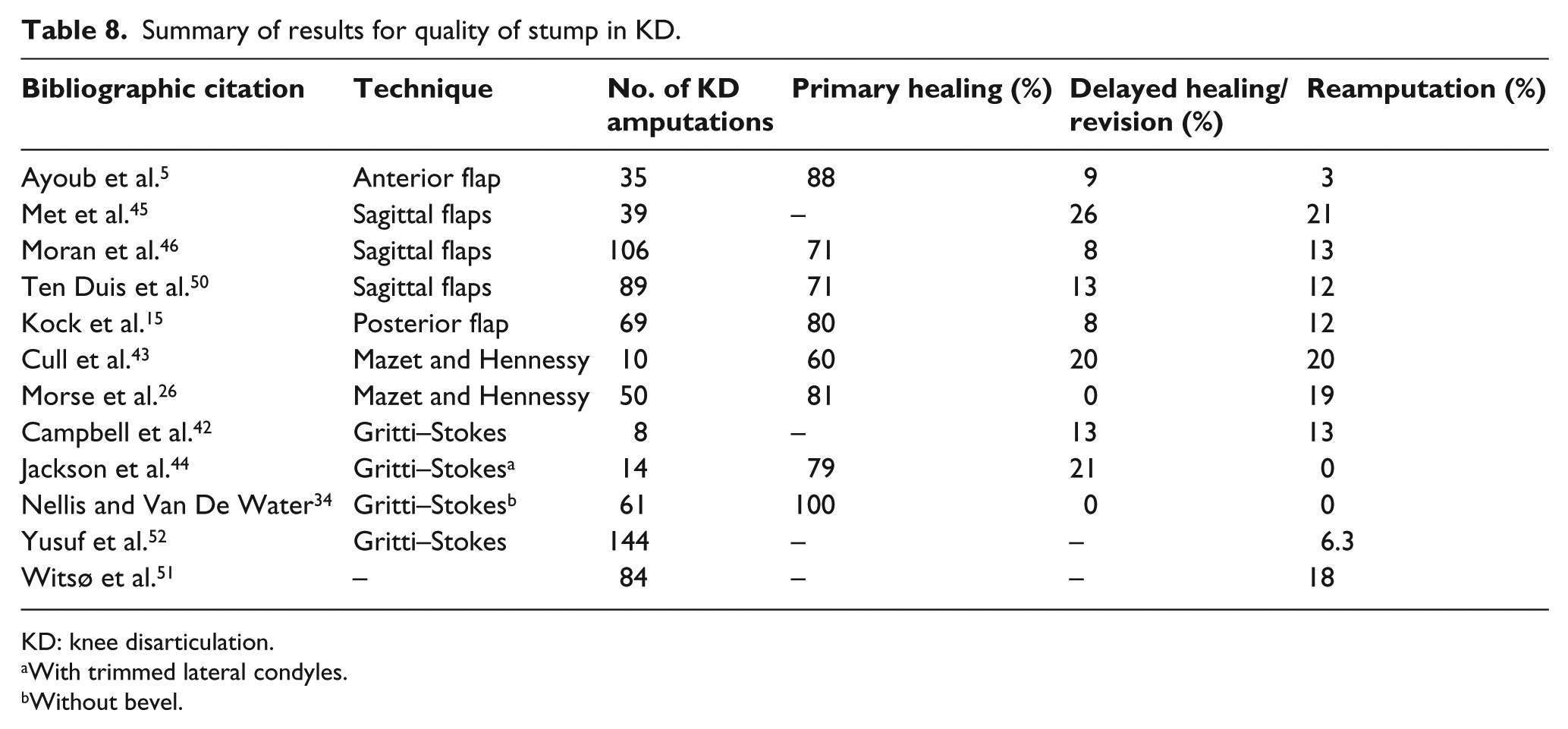
KD: knee disarticulation.
With trimmed lateral condyles.
Without bevel.
Nine studies used clinical judgments to determine the appropriate amputation level,5,15,26,42–46,51 none of the studies utilised physiological tests and three studies did not indicate the method of assessment.34,50,52 The number of identified variables/confounders that affect wound healing ranged from 0 to 5 among the studies, but only one study analysed how the variables influenced the results. 50
Functional outcomes
Four studies reported on results relating to the functional outcomes. One prospective study used the Sickness Impact Profile 68 (SIP-68), Groningen Activity Restriction Scale (GARS) and Timed Up and Go (TUG) test. 48 Another study measured the maintenance of preoperative independent status based on clinical records. 38 Both studies made comparisons to TT and TF levels.38,48 The last two studies used custom surveys to measure independent living with no comparison to other amputation levels.26,44
Prosthetic ambulation
A summary of results for prosthetic ambulation is listed in Table 9. Prosthetic ambulation rates do not include therapeutic and cosmetic limb wearers. Nine studies reported on results relating to prosthetic ambulation, and data pooling was not possible due to heterogeneous studies. The prosthetic ambulation rate for KD amputees ranged from 13% to 75%. No distinct observations can be made between the countries undertaking these studies. Moran et al.’s 46 results excluded reamputated TF ambulant patients, and the follow-up results from Kock et al.’s 15 study were based on surviving patients only; hence, the rates increased at 9 years when a greater proportion of ambulant patients survived.
Summary of results for prosthetic ambulation in KD.
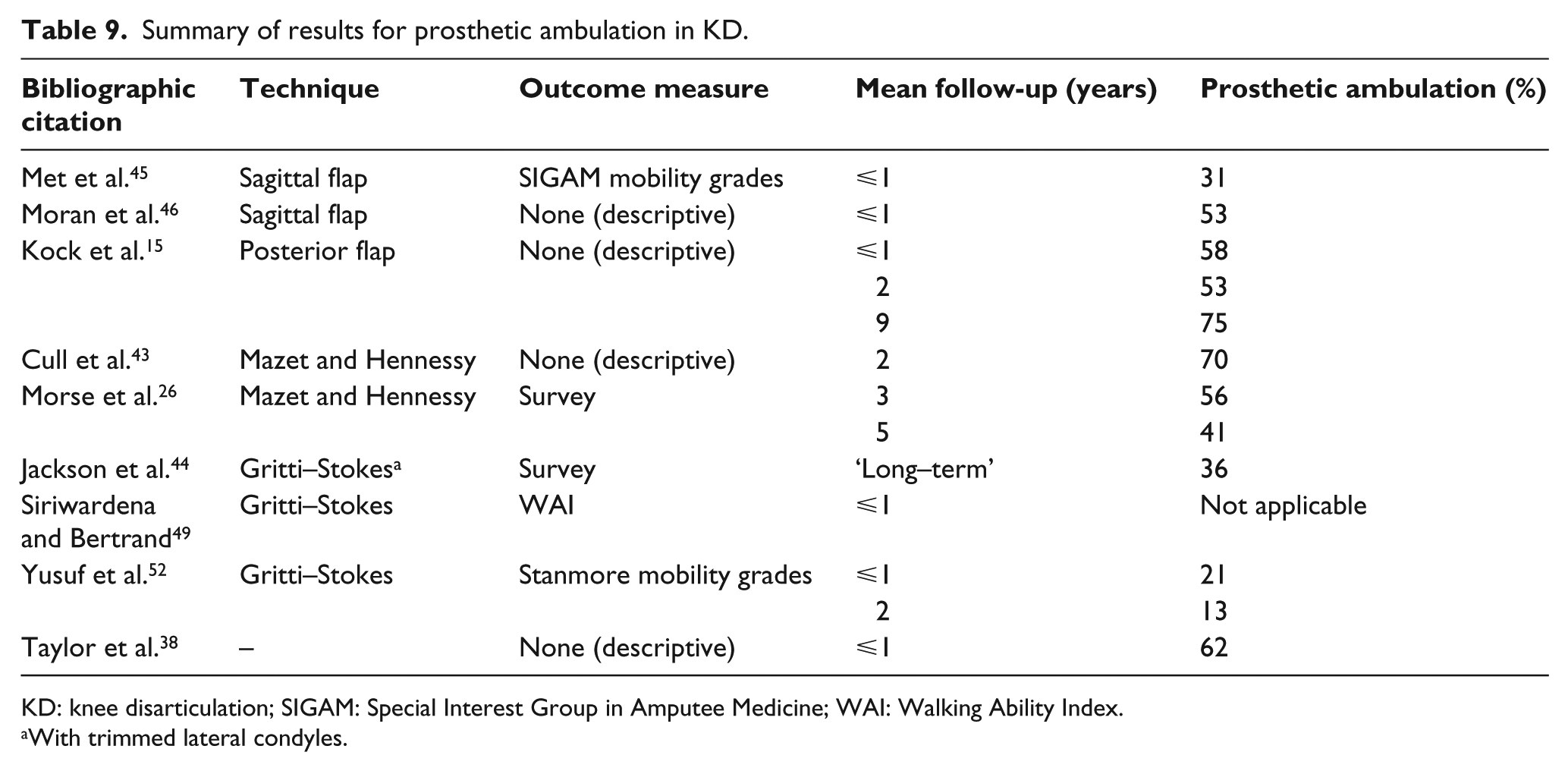
KD: knee disarticulation; SIGAM: Special Interest Group in Amputee Medicine; WAI: Walking Ability Index.
With trimmed lateral condyles.
Three studies used mobility scales,45,49,52 and six studies did not do so,15,26,38,43,44,46 out of which two were surveys.26,44 Three studies involved a prosthetist in the research team,38,43,44 while others did not.15,26,45,46,49,52 The number of identified variables/confounders that affect prosthetic ambulation ranged from 0 to 5 among the studies; however, only two studies analysed how these variables influenced the results.38,49
Gait biomechanics
Two studies reported on results relating to gait biomechanics. One study compared the walking capacity and metabolic costs of amputees. The walking capacity, measured by speed, cadence and stride length, decreased with proximal amputations. 8 Some of the results involving the metabolic costs (net oxygen cost, maximum capacity and functional energy cost) were unclear and did not relate to their derivations in the reported table legends in the study; hence, they are excluded from this review. The other study analysed the gait of four bilateral patients with TT and contralateral KD amputations, comparing forefoot propulsion, vertical ground reaction forces (GRFs) and centre of pressure (CoP) progression within the foot. 47
Discussion
Quality of stump
Due to a small number of studies, the effects between surgical techniques were not obvious, and no patterns were observed between countries where the studies were conducted. As only four studies made comparisons to other amputation levels, the comparisons were not conclusive too.42,45,51,52 There was also a lack of statistical analyses in most studies; hence, it was hard to determine whether results were significant especially for studies with small sample sizes.
With regard to primary healing, low rates in Cull et al.’s 43 study could be attributed to subjects having severe peripheral vascular disease, secondary amputations (40% had failed TTA) and high rates of previous unsuccessful revascularisation (90%). Furthermore, the study had a small sample size (n = 10) and would not be statistically significant. Excluding this study, the primary healing rates would range between 71% and 100%, which is similar to 70% primary healing rates of TFAs. 53 However, healing rates were subjective due to a lack of full reporting of confounders and multivariate analyses of reported confounders. Factors affecting wound healing are manifold, such as smoking, malnutrition, absence of demarcation, method of amputation level selection, use of prophylactic antibiotics, surgeon experience, drain usage and type of dressing. 54 Other controversial factors include hemorheology, previous revascularisation and presence of diabetes mellitus. 54 One study found that the type of dressing may not affect KDs as much as TTAs (p = 0.447), but a high number of comorbidities may influence healing as well (p = 0.009). 50 These factors need to be addressed with multivariate analyses for conclusive comparisons of primary healing of KD against other amputation levels.
Reamputation rates are also multifactorial, including non-physiological methods of determining amputation levels, surgeon experience, infection, circulatory failures and enfeebled patients. 1 None of the studies used physiological methods (e.g. systolic/perfusion pressure measurements 54 ) for determining amputation levels; hence, higher reamputation rates of KD compared to TF levels may be due to the fact that many patients were unsuitable for KD in the first instance. In certain studies, 40%–50% of reamputations were also previously failed TTAs, indicating inappropriate amputation level selection.43,46 Met et al. 45 recognised that not using physiological methods might explain higher reamputation rates, and Witsø et al. 51 highlighted the need for additional methods of assessment. Patients with absent ipsilateral femoral pulse should not be undergoing KD due to high risks of complications (odds ratio: 74.0). 26 TF is naturally the safest level of amputation with lowest reamputation rates; however, it does not mean KD should not be considered. The key is having ancillary physiological tests to supplement clinical judgments in deciding the appropriate level of amputation. These would include testing of skin blood flow, perfusion and nutritional status of the patient before amputation. Reamputations lead to increased risks to patient, prolonged hospitalisation and low morale. 42 This warrants the need for continued research in valid and reliable assessment methods of amputation levels.
The amount of viable tissues required for KD is similar to a short TT stump, 3 but none of the studies addressed when a KD is indicated over a short TTA. Witsø et al. 51 highlighted the need for a well-circulated posterior flap in KD, which is advocated by Kock et al., 15 as the blood supply to the knee region comes from the gastrocnemius heads. Gritti–Stokes had lower reamputation rates, which coincides with findings from the International Society for Prosthetics and Orthotics (ISPO) consensus, 1 but issues with long-term pain and patella instability have been previously reported. 55 These were, however, not reported in the studies of this review. The follow-up period could be too short, or it could be a past issue. There were also many detriments reported against the Mazet technique,3,5,10,18 but these were not present in the studies included in this review. The technique allows shorter flaps for wound closure and hence improved healing. 26 Mazet et al. 56 also recommended the technique for the dysvascular patient only if the patient has a palpable femoral pulse and good skin quality around the knee joint.
The belief that KD is prone to wound complications was based on studies dated back to1970s when anterior flaps were used.57–60 This is possibly no longer relevant, and there should be a reconsideration of KDs since healing rates are similar to TFAs. However, the crucial point is to have accurate methods of assessing appropriate amputation levels. With regard to modified KD techniques like the Gritti–Stokes and Mazet, there needs to be further well-established research done to justify that these techniques are suitable for the dysvascular patient.
Functional outcomes
There were no significant differences among the amputation levels in Schoppen et al.’s 48 study with the outcome measures; however, it might be due to a high proportion of TT patients and interaction of different variables. Patients with poor one-leg standing balance did significantly poorly in all tests, and these patients were likely to have more proximal amputations. 48 Hence, proximal amputation levels are likely to be linked with poorer outcomes. Taylor et al. 38 found that the TFA had the poorest maintenance of preoperative independent status (p < 0.001), whereas KD, like the TTA, did not have any significant influence. TFA was also the only level that was independently associated with the failure to maintain independence (hazard ratio: 1.8). 38 Patients with the Mazet technique had almost identical maintenance of independence at a 3-year follow-up to Morse et al.’s 26 study; however, no comparisons to other amputation levels were made and the survey results were subjective. Gritti–Stokes patients had poor rates of independence, but measurements were not related to maintenance of preoperative independence, and it was a survey (subjective) with no comparisons to other levels. 44 Studies suggesting that KD gives a greater functional outcome than TFA in dysvascular patients were only from a 1-year follow-up period,38,48 and further research is required to determine the long-term effects of KD.
Prosthetic ambulation
Due to the small number of studies, the effects between surgical techniques were not conclusive, and no patterns could be seen between countries where the studies were conducted. Met et al. 45 found no significant differences between KD and TF levels, but the identification of variables/confounders to prosthetic ambulation was poor and hence the results cannot be directly attributed to amputation levels. Variables that influence prosthetic rehabilitation are advancing age, presence of comorbidities (including mental diseases), premorbid functional/ambulatory level, condition of contralateral limb, presence of oedema and psychosocial factors.38,41,45,49 These factors will have to be part of a multivariate analysis together with the level of amputation to determine whether any amputation level has an independent influence on prosthetic ambulation. It will also be more accurate to indicate the maintenance of ambulatory status rather than actual ambulation rates, as many older dysvascular patients have limited preoperative mobility. The only study that fulfilled these criteria indicated that KD had better ambulatory rates than TF (p < 0.001). 38 The study also found that only the TFA had an independent factor in influencing non-prosthetic wear (odds ratio: 4.4). 38 In terms of outcome measures used, there was a lack of reliable and validated mobility scales,15,38,43,46 and the use of surveys26,44 would be subjective. It will be difficult to have reliable results since all of the studies were retrospective and mostly based on clinical records. There was also minimal involvement of prosthetists in the research teams; ideally, both a prosthetist and a physiotherapist should be present in assessing the ambulation of an amputee to rule out any bias.
Yusuf et al. 52 mentioned that prosthetic rehabilitation was difficult in their study due to old age and associated diseases, Met et al. 45 stated that the reasons for diminished mobility in their study were serious comorbidities and mental diseases, and Jackson et al. 44 stated that 50% of the subjects in their study were not ambulating due to comorbidities but 81% achieved expected preoperative functional status. These three studies accounted for the lowest ambulatory rates ranging between 13% and 36%; hence, higher rates may be achieved if maintenance of preoperative ambulatory status was reported.
Kock et al. 15 used the posterior flap technique, and the rates of prosthetic ambulation increased at 9-year follow-up, excluding non-survivors. This is possibly indicating that ambulatory rates are high among the healthy surviving patients, and results from the initial years were influenced by patients with greater comorbidities. The posterior flap aids prosthetic rehabilitation as it allows a well-padded end-bearing stump and is particularly beneficial to the elderly. 15 The study appeared to have better results than studies that used the sagittal flap technique,45,46 but a direct comparison is not possible due to the other variables that influence prosthetic ambulation. A short TTA could also be done with this technique, but this was not addressed in the studies. Nevertheless, good outcomes are still highly dependent on patients’ preoperative functional status, postoperative care and access to a well-functioning rehabilitation clinic, regardless of amputation level.
It was claimed that the Mazet technique allows effective use of KD suction sockets, distributing forces over the entire stump surface rather than over the condyles while maintaining some end-bearing characteristics. This is possible due to the conical stump shape from the shaved condyles, and the authors reported no late skin breakdown, no rotational instability, no belts/straps required and ease of donning.26,43 If the claims are true, that could potentially reduce the disadvantages of KD, with no prosthetic shear forces on the condyles, ease of fit and better cosmesis. The weight-bearing area is reduced,10,18 but the suction sockets would redistribute forces over a greater area. Compared to the TFA, the long lever arm is maintained with a reduced need for ischial bearing or auxillary suspension. An excluded study, which consisted of both dysvascular and non-dysvascular patients, combined the posterior flap and the Mazet technique for patients who were likely to ambulate and achieved 81% maintenance of ambulation. 11 Other authors condemned the technique due to the risk of haematoma and infection from the bleeding bone; 10 however, that may not be entirely relevant as TFAs also involve bone transection. Consequently, there is a possibility of a greater level of trauma involved in using the osteotome for the Mazet technique, compared to the amputation saws used in TFA. There needs to be more detailed reporting of follow-up results and direct comparisons with TF patients within the studies to justify the benefits of the Mazet technique.
The Gritti–Stokes amputation had a lower prosthetic ambulation rate ranging between 13% and 36%. It allows space for the prosthetic knee mechanism, and the posterior bevel prevents the patella from slipping forward. 52 However, some authors have stated that high peak pressures are created during weight-bearing, with possible failure of patella union.3,10,16 These issues were not reported in the studies of this review, although many patients abandoned prosthetic use over a 23-month follow-up in one study. 52 The reasons were not stated, but it could be possible that it was due to the stated detriments by other authors. Jackson et al. 44 stated that long-term pain and patella instability were not apparent in their study; however, they failed to mention the exact period of follow-up. Only 50% of Gritti–Stokes patients were satisfied with their prosthetic cosmesis, compared to 84% of TF and 94% of TT patients in another study, and it took a longer time for prosthetic fitting. 49 However, the study was conducted two decades ago, and current prosthetic advancements may have improved prosthetic fitting and cosmesis in Gritti–Stokes amputations. Gritti–Stokes amputees were known to achieve poor prosthetic fitting and ambulation compared to standard KD amputees, 10 which is also apparent in this review. Overall, Gritti–Stokes subjects did not perform significantly better than TF subjects in these studies during follow-up.49,52
Gait biomechanics
Metabolic results from Pinzur et al.’s 8 earlier study were excluded due to the reasons stated in the ‘Results’ section. There were also no consistent patterns observed; the authors stated that the metabolic cost of walking increased with proximal amputations, but this was not apparent from the tables and figures presented. The values fluctuated with higher amputation levels; furthermore, there was no statistical analysis to determine the significance of the results. Only walking capacity decreased with proximal amputations, although there was no proven statistical significance, and the sample size of each group was small (n = 5).
In the study that analysed the gait of bilateral dysvascular amputees with TT and contralateral KD amputations, there was a greater transfer of body weight to the prosthesis in the KD limb compared to the TT limb, based on the vertical GRF results. 47 This was statistically significant in both early (p < 0.01) and late stance (p < 0.005), and it is likely attributed to the end-bearing nature of KD stumps. In normal gait, a limb should experience peak vertical GRFs (approximately 110% of body weight) during loading response (weight acceptance) and push-off due to the deceleration and acceleration of body mass. 61 There was also a smoother transition of GRF in the KD limb than the TT limb as measured in the CoP progression in the foot, although the recording was only provided from one patient. There was no significant difference between the forefoot propulsion of the KD and TT limbs, indicating that there is no loss of propulsion with a polycentric prosthetic knee in KD when compared to an anatomical knee in TT. 47 This may be attributed to the fact that dysvascular TT patients with limited ambulatory function do not maintain quadriceps and hamstrings muscle activity as effectively as active TT walkers, hence not gaining the full benefits of the knee joint. 62 The study indicated greater stability with the KD limb compared to the TT limb; however, more proximal amputations could result in increased energy consumption and decreased walking capacity, and this was not addressed in the study. With current TT and KD prosthetic technologies, the results may also vary if this experiment is repeated. Furthermore, the study was limited by a small sample size (n = 4), and further credible research is required.
Quality appraisal
There were no controlled trials, a substantial amount of non-comparative studies, and only one study had a very low risk of bias. This led to an overall low strength of evidence in this topic of interest, although it is very difficult to conduct controlled trials in amputation surgeries. There was also a lack of detailed, reliable and validated outcome measures along with a lack of relevant multidisciplinary teams. There was a substantial amount of studies that did not execute any statistical analyses, and the results can be deceiving especially with studies of small sample sizes. Some of these studies only had a KD population group but made claims in comparison with the other amputation levels. Many of these studies failed to recognise that rehabilitation outcomes are multifactorial, with many influencing variables. Even when some variables are identified, there was a lack of multivariate analyses to identify independent factors. There was also a lack of follow-up or poor reporting of follow-up results.
Limitations
This review only considered English publications, and other research in foreign languages may be overlooked. There was also a lack of multiple expert reviewers with independent judgments during the conduct of this review. No other medical professions were involved; however, key findings were discussed with an experienced orthopaedic consultant in an effort to reduce the risk of bias judgments.
Conclusion
When dysvascular patients are considered for proximal lower limb amputation levels, they are usually in their advanced ages, with poor preoperative functional status and associated comorbidities. It is difficult to determine the direct effects of KD on such a vulnerable population, especially with the limitations of the available literature. Healing rates are similar to TFAs, but there is a need for valid and practical assessment methods for appropriate amputation level selection to prevent reamputations. It is also unclear when a KD is appropriate over a short TTA for ambulatory patients as they have similar requirements of tissue viability. This warrants the need for further research into formulating prescription guidelines for KD. KD patients have better maintenance of independent living status than TF patients, but prosthetic ambulation rates are inconsistent across studies. The prosthetic ambulation results would be more accurate if variables were accounted for and maintenance of preoperative ambulatory status measured. There is no conclusive evidence regarding the gait biomechanics of dysvascular amputees due to the paucity of credible research in this subject area.
There is a consensus that the anterior flap is a dated technique and should be avoided in KD. Correspondingly, the only study that used this technique was conducted two decades ago. Theoretically, the posterior flap allows better vascularisation and padding for the end-bearing stump than sagittal flaps, but there were no direct comparisons of the two techniques in current studies. The Mazet technique is potentially propitious in both the quality of stump and prosthetic ambulation, but the study designs need to be more robust in providing evidence that previously reported technical flaws are no longer relevant, and the technique is suitable for the dysvascular population. Gritti–Stokes amputations had low reamputation rates and controversial ambulation rates. If it is proven to be unsuitable for prosthetic ambulation, it is still suitable for non-ambulatory patients to achieve the non-prosthetic benefits of KD, with less risk of revisions.
Recommendations
A stronger body of evidence is required to determine whether a greater proportion of KD can be justified among dysvascular amputees. The authors recommend future research to be of prospective studies, with comparison to different amputation levels in the dysvascular population and with long-term follow-up. Variables have to be fully accounted for in a multivariate analysis as rehabilitation outcomes are multifactorial. There is a need for continued research and the use of valid and reliable assessment methods of amputation levels and the formulation of prescription guidelines in the selection of a KD level of amputation. If prosthetic ambulation is measured, the involvement of prosthetists and physiotherapists with the use of validated mobility scales is necessary. The maintenance of preoperative ambulatory status should also be measured. No quality-of-life outcomes have been found during the conduct of this review, and it will be beneficial to analyse the perceptions of KD amputees in comparison with other amputation levels.
Footnotes
Acknowledgements
The authors would like to thank Dr. Amar Jain (Consultant Orthopaedic Surgeon, Ninewells Hospital, Dundee UK) for his expert opinion in this review, together with Sarah Deans and Kim Gadsdon for their valuable contributions.
Author contribution
Tsurayuki Murakami conducted the study and prepared the manuscript, Kevin Murray supervised the study and assisted in the preparation of the manuscript.
Declaration of conflicting interests
The authors report no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.