
Abstract
The aim of this study was to analyze survival, wound healing and ambulation after knee disarticulation (KD). A historic cohort study using medical records and nursing home records was performed. Data included demographics, reason for amputation, concomitant diseases, survival, wound healing, re-amputation and ambulation. Data of 80 patients (71 unilateral and nine bilateral amputees) were available for evaluation. Median follow-up was 9.9 years (IQR: 4.1; 14.3 years). Mean age of amputation was 76.9 (± 9.6) years. Reason for amputation was gangrene in 72 patients. Most common concomitant (96%) disease was peripheral arterial disease (PAD). Survival after 1, 6 and 12 months was 87%, 65% and 52%, respectively. Delayed wound healing occurred in 42% (n = 16) of the patients with two or three concomitant diseases and in 15% (n = 6) of the patients with no or one concomitant disease. Trans-femoral re-amputation was performed in nine (12%) patients. Of the 61 discharged KD amputees, 36 (59%) were provided with a prosthesis. Eventually 21 (34%) patients became household walkers.
Introduction
Despite continuing medical progress and improvements in general living conditions, we increasingly find ourselves faced with elderly, multiple ill patients in whom the limits of reconstructive procedures for peripheral arterial disease (PAD) have been reached. These patients account for more than 90% of all limb amputations.1-3 When vascular intervention in lower limbs by non-invasive or operative treatment has failed, lower limb amputation may be the only option to save the life of a patient. After consultation with a rehabilitation team the surgeon then has to decide on the level of amputation, bearing in mind that maintenance of ambulation is an important factor associated with preserving independence.4
An important goal in the care of the patient who requires amputation is to retain the knee joint, given its contribution in preserving ambulation.5 Ideal stump length for trans-tibial amputation (TTA) is approximately 15 cm below the knee joint.6 Whenever this margin is not feasible, or an adequate soft-tissue envelope of mobile muscle or full-thickness skin in areas of load transfer can not be retained, a more proximal knee disarticulation (KD) or trans-femoral amputation (TFA) should be considered.
Before the use of surgical anaesthesia, the advantage of KD was the speed of surgery and the limited amount of associated bleeding (as this technique does not violate or transect any muscle bellies). Additionally, KD has the advantage of maintaining the cartilage barrier which potentially reduces the risk of infection, which is especially important in compromised patients.7-9 Clinically, the most important advantages of KD procedures are direct load transfer to the residual limb with enhanced walking independency and less energy consumption compared to TFA.7,10-13 KD combined with polycentric (exo-skeletal) prosthetic joints, can offer considerable walking stability in geriatric patients.9,12
Although Smith described a KD as early as 1824,14,15 it initially never gained the popularity as the TFA did, because of assumed greater risk of delayed wound healing with necrosis and/or infection leading to re-amputation.13,16,17 Ever since, surgical techniques have used a variety of surgical flap designs to reduce these problems.7,13,16,18-22
Despite increasing popularity during the past 20 years,23 KD still receives little attention.16 Yet, enhanced stability of walking (better mobility) after KD, as well as lower mortality rates as compared to TFA suggests a more prominent role of KD.12,13,24 Potential ambulatory patients who have a substantial knee-flexion contracture can be successfully fitted with and use a prosthesis after KD. In non-ambulatory patients muscle imbalances in trans-tibial amputees may induce knee-flexion and hip contracture, whereas a hip flexion-abduction contracture may result following TFA. Patients with knee-flexion contractures are prone to pressure ulcers on the distal stump. The stump of the trans-femoral amputee provides little support for sitting in a chair and the lever arm is inefficient for use in transfers.8 A short stump results in decreased trunk stability and limited ability to lean forward in case of bilateral TFA. Concluding, KD can be an appropriate alternative for TTA and TFA, depending on patient and treatment intentions.25-27
The aim of this study was to analyze survival, wound healing and ambulation after KD in patients predominantly suffering from peripheral arterial disease.
Methods
Design and setting
A historic cohort study was performed using medical records and nursing home records. Of all lower limb amputations all KDs between July 1989 and March 2006 were selected. One surgeon (HV) in a single 340-bed community hospital in the north of The Netherlands carried out all amputations. The medical records and nursing home records included data on patient demographics, concomitant diseases such as diabetic mellitus, cerebrovascular diseases, cardiovascular diseases and systemic diseases (e.g., rheumatoid arthritis), reason for amputation, previous ipsilateral revascularisation, previous ipsilateral amputations, and postoperative data, including survival, wound healing, infection, re-amputation trans-femoral, dressing method, hospitalisation time, discharge destination, prosthesis fitting and ambulation level. Data from the records were entered in a database. Dates of death were verified using the hospital's computerized patient records or death certificates derived from municipal offices. Data concerning prosthesis fitting and ambulation were retrieved from records of the rehabilitation centres and nursing homes.
Statistical analysis
Descriptive statistics and χ2 analyses were performed using SPSS version 12.0 for Windows.
Results
Patients
Descriptive statistics concerning patients (n = 80), reason for amputation, side of amputation, concomitant diseases, previous ipsilateral procedures and postoperative dressing method
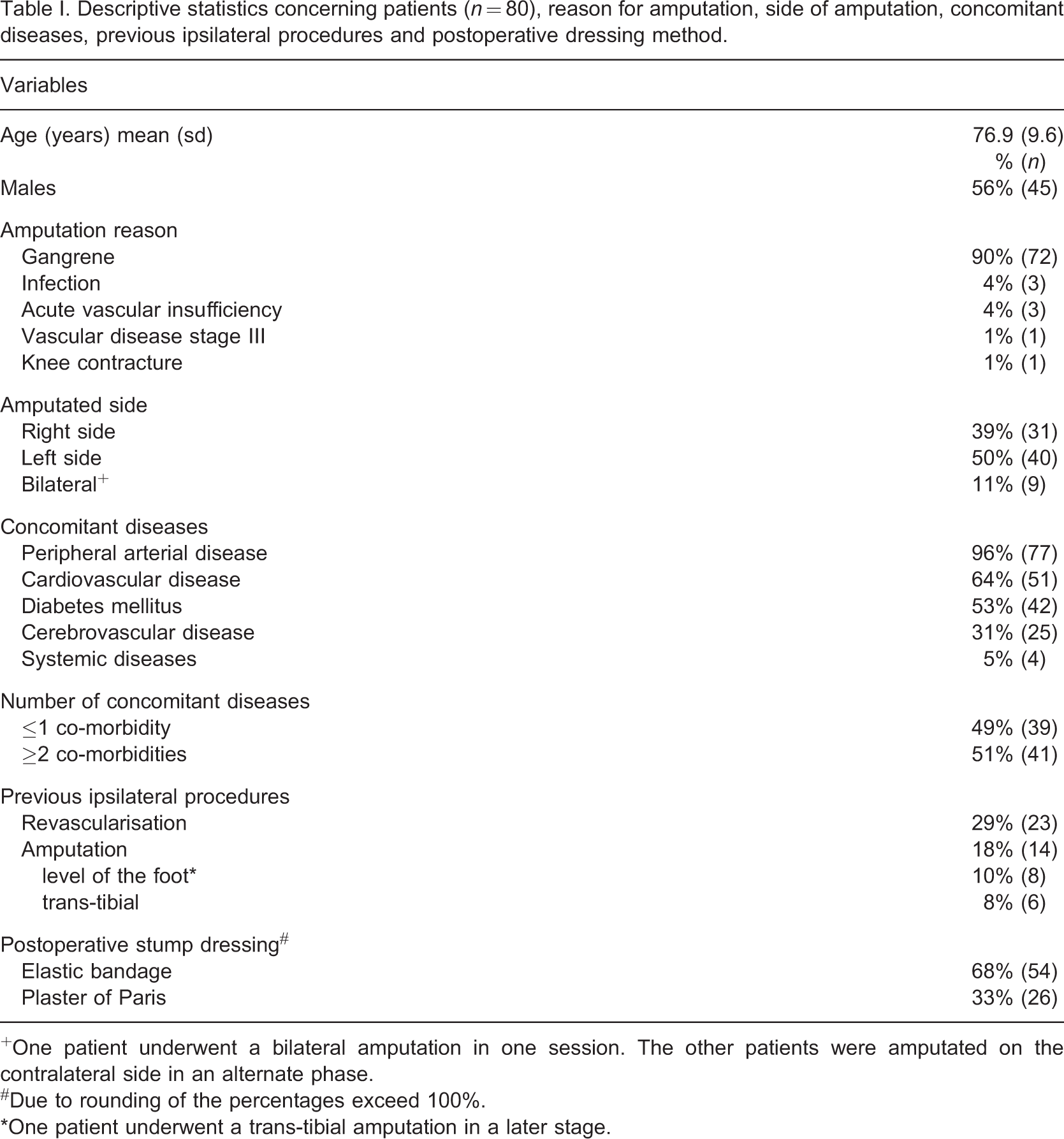
+One patient underwent a bilateral amputation in one session. The other patients were amputated on the contralateral side in an alternate phase. #Due to rounding of the percentages exceed 100%. ∗One patient underwent a trans-tibial amputation in a later stage.
The mean age of women (79.0 ± 9.9) at the time of amputation was slightly higher than that for men (74.4 ± 9.2).
The median interval between the last vascular reconstruction and the KD was 8.9 months (IQR: 1.1; 52.6). The median interval between a previous ipsilateral amputation and the KD was 3.4 months (IQR: 1.6; 20.4). Median hospitalisation time was 36.5 days (IQR: 17; 68.8).
Survival
Three (4%) patients died within three days after the amputation from cardiopulmonary complications and renal failure. Overall, 10 (13%) patients died during hospitalisation. Survival after 1, 6 and 12 months was 87%, 65% and 52%, respectively. Survival of patients with a bilateral KD was considerably poorer than of patients with a unilateral amputation (Figure 1).
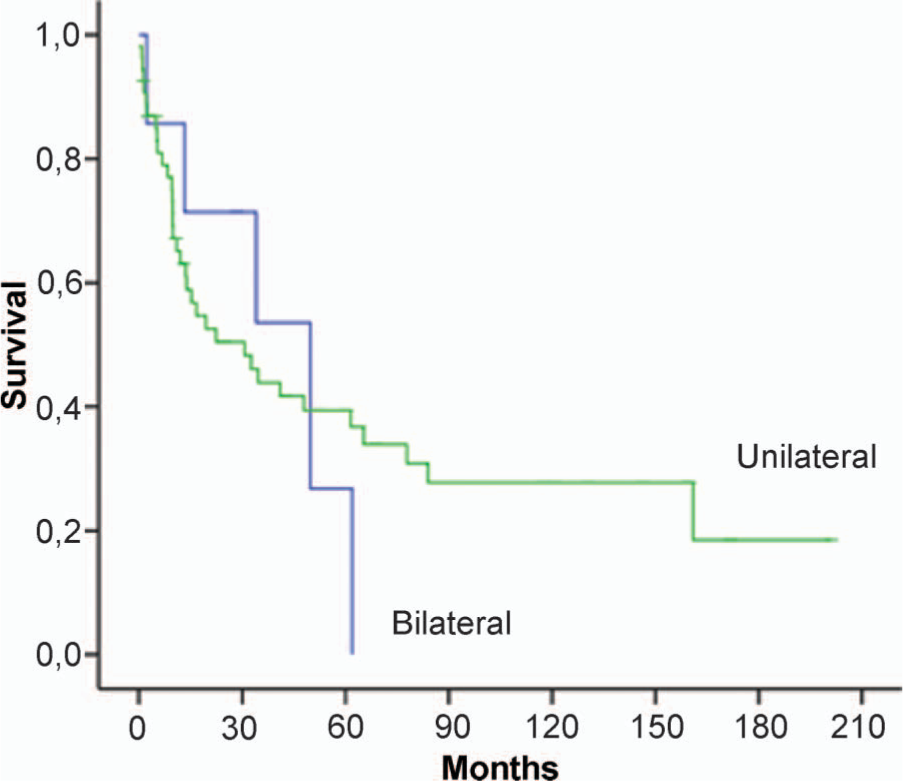
Survival after knee disarticulation in months.
Wound healing
Because three patients died in the very early post-operative phase, data of these patients were excluded from the wound healing analysis, leaving a data set of 77 patients for analysis.
Statistics concerning wound healing (n = 77), discharge (n = 80), prosthesis fitting (n = 61) and ambulation (n = 36)
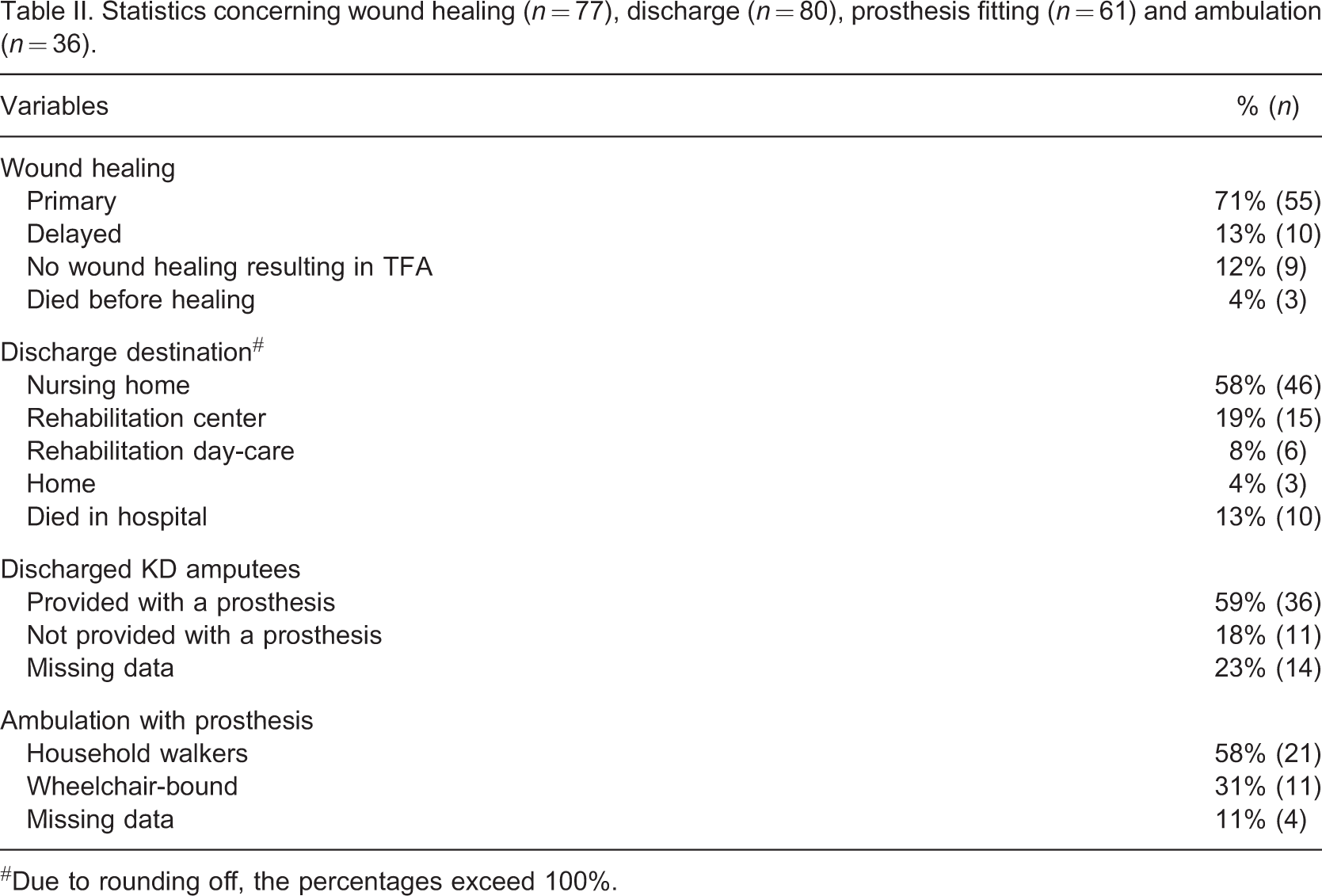
#Due to rounding off, the percentages exceed 100%.
After a median interval of 2.1 months (IQR: 1.0; 18.7), nine patients (12%) were amputated again contra-laterally at KD level due to PAD. Of the patients who had an ipsilateral amputation at the level of the foot or tibia before KD, none needed a TFA in an alternate phase.
Discharge and ambulation
Ten (13%) patients died in hospital. Forty-six (58%) patients were rehabilitated in a nursing home and 15 (19%) patients went to a rehabilitation centre as inpatients. Six (8%) patients received day-care rehabilitation (out-patients) and three (4%) patients went home without rehabilitation treatment.
Of the 61 discharged knee-disarticulation amputees (trans-femoral amputees (n = 9) and patients deceased in hospital (n = 10) were not included in this analysis), 36 (59%) patients were provided with a prosthesis and 11 (18%) were not. For 14 (23%) patients these data were not available. In total 34% (21 of 61 discharged knee-disarticulation amputees) became household walkers, 11 (18%) were wheelchair-bound. Four patients were able to walk more than 500 m with the aid of walker or crutches. For four patients data on ambulation status were not available (Table II).
Discussion
Patients with a bilateral KD had a poorer survival using sagittal flaps after 1, 6 and 12 months (87%, 65% and 52%, respectively) compared to those amputated unilaterally. Delayed wound healing (29%, n = 22) was significantly related to two or more concomitant diseases. Wound healing occurred in 84% of the patients. Of the discharged knee-disarticulation amputees, 36 (59%) were provided with a prosthesis. Twenty-one (34%) patients became household walkers.
Our survival of 87% one month after KD was favourable compared with the 80% survival found previously for a similar procedure,28 also because in the latter study the mean age of the patients was 72 years whereas in the current study the mean age is 79 years. Our results seem to be comparable with the literature regarding the in-hospital 48-day survival after gastrocnemicus flap procedures (ranging from 78–91%)3,19,23,28 Twelve months survival of 52% in our study could not be compared, because previous studies used different follow-up periods.19,23-25,29,30 A survival rate of 48% after 26 months in the study of Kock et al. was more favourable than our results, but the mean age (66.7 ± 11.3) of their sample (n = 66) was statistically significant (p < 0.001) lower than our sample.23 Clinically, our data indicated that 52% of the patients survived after 12 months who would otherwise have been deceased because of gangrene. These patients were critically ill and an amputation was their only hope to extend their lives.
Survival after bilateral KD was considerably poorer compared to survival after unilateral KD (Figure 1). Presumably, these patients were more ill; the contra-lateral KD after a median period of 2.1 months and their poor survival were a consequence of this illness.
Primary wound healing rate of 71% in the current study was identical with the rates found previously,23,28 but as mentioned before, the mean age of amputation in those studies was considerably lower. Two or more concomitant diseases influenced wound healing considerably. Diabetes as a single concomitant disease did not influence wound healing as was found previously.31
For many years, TFA was recommended because of the supposed better wound healing compared to that at a more distal level.5,13 However, pooled data from large series showed a total healing rate of approximately 85% in TTA procedures, which was better than rates found previously for TFA procedures.5 In comparable samples sizes for KD procedures, different wound healing rates ranging from 40–80% are described.13,19,23-25,29,30 Comparatively, a primary healing of 71% and a secondary healing rate of an additionally 13% in this study were identical with results in other KD procedures and almost equal with those found for TTA procedures. Thus, assumed delayed wound healing is not a reason for performing an initial TFA to be sure of better healing at a more proximal level than KD.
Re-amputation at a trans-femoral level was necessary in only nine (12%) patients. Compared to re-amputation rates after conventional KD procedures (ranging from 19–40%),24,30,32 our results seem favorable. Compared to KD procedures using a gastrocnemicus flap, our results are similar to Klaes and Eigler (1985)19 and Kock et al. (2004).23
At present, no established test can predict the optimal level of amputation, related wound healing and level of ambulation after amputation. Predicting whether an amputation wound is likely to heal is challenging, since patients who are predicted to have adequate wound healing could be ambulatory immediately after surgery, which is likely to improve both their physical and psychological state.33 Skill and experience of the surgeon are still important factors in determining level of amputation. It is notable, that of the six patients who had a KD after TTA, none developed an infection or wound healing problem requiring further revision to TFA, thus the amputation level was appropriate.
Advancing recovery, post-operative rigid dressings are strongly recommended, because of local protection of the wound and the prevention of oedema and knee-flexion contractures.34,35 However, the optimal stump dressing method after KD is not well studied. Nevertheless, some reviews reveal a trend in favour of rigid and semi-rigid dressings for achieving stump healing and reduction of stump volume. Primary wound healing after TTA occurs earlier in case of rigid dressings.34,35 In the current study, no significant difference in wound healing between patients postoperatively treated with soft dressings and patients treated with rigid dressings was found.
Only a limited percentage (45%) of the original 80 amputees could be provided with a prosthesis and only 26% became ambulatory. These results do not seem too favourable at first glance compared to patients in other studies (29–77%).23,24,28 However, our patients were considerably older compared to other studies. Furthermore, other studies relate the rates of prosthesis provision and ambulation to the number of patients discharged. If we calculate our data accordingly 59% of the patients were provided with a prosthesis and 58% of those became household walkers. After this calculation our data still remain somewhat less favourable.
A limitation of our data was that data of 14 patients with respect to prosthesis provision and four with respect to ambulation level could not be retrieved. Our results only remain less favourable if all missing data concern patients who are not provided with a prosthesis and are wheelchair-bound.
Another limitation of our study was the retrospective design. Medical records of four patients were not complete. Nursing home records of the rehabilitation facilities were of moderate quality. Many data were missing as mentioned above. Further, the data from the medical records and the nursing home records had to be interpreted and some times arbitrary decisions had to be made. In case of such decisions two observers in consensus decided what was to be entered in the data base.
Clinically, amputation should be regarded as a reconstructive procedure that is designed to restore function and attempt to allow the patient to return to an independent lifestyle. Ambulation after amputation, with or without the use of aids, represents a major achievement. Whenever the knee joint cannot be saved a TFA should be avoided in favour of KD. There are no grounds for performing an initial TFA to spare the patient an additional operation. Although quality of medical care and therapeutic options are improving every year, the one year survival of knee-disarticulation amputees is low.
Footnotes
Acknowledgements
The authors thank the Department of Surgery of Nij Smellinghe Hospital Drachten for conducting this study. They would like to express their gratitude to the rehabilitation centres and nursing homes for the provision of data.