
Abstract
Background:
Comparative effectiveness of prosthetic feet during ramp ambulation in unilateral transtibial amputees, who function at different Medicare Functional Classification Levels, has not been published.
Objective:
To determine differences in symmetry in external work between four categories of prosthetic feet in K-Level-2 and K-Level-3 unilateral transtibial amputees during ramp ascent and descent.
Study design:
Randomized repeated-measures trial.
Methods:
Ten subjects completed six testing sessions during which symmetry in external work was calculated using F-scan in-sole sensors. Between testing sessions 1 and 2, subjects received standardized functional prosthetic training. In Sessions 3–6, subjects tested four feet—solid ankle cushion heel, stationary attachment flexible endoskeleton, Talux (categories K1, K2, and K3, respectively), and Proprio-Foot (microprocessor ankle)—using a study socket and had a 10- to 14-day accommodation period with each foot.
Results:
During ramp descent, K-Level-2 subjects demonstrated higher symmetry in external work values with Talux and Proprio-Foot compared to the solid ankle cushion heel foot. K-Level-3 subjects also had higher symmetry in external work values with the Talux foot than the solid ankle cushion heel foot. Ramp ascent symmetry in external work values were not significantly different between feet.
Conclusions:
Prosthetic foot category appears to influence symmetry in external work more during decline walking than incline walking. K-Level-2 unilateral transtibial amputees achieve greater symmetry from K3 dynamic response prosthetic feet with J-shaped ankle and microprocessor ankles while descending ramps.
Clinical relevance
The findings suggest that K-Level-2 unilateral transtibial amputees benefit from K3 dynamic response prosthetic feet with J-shaped ankle. These results support the prescription of K3 feet for K-Level-2 amputees who frequently negotiate ramps.
Keywords
Background
In the United States, the governmental definition of foot/ankle assemblies (Table 1) defines five Medicare Functional Classification Levels (MFCL) for amputees (K-Level-0 through K-Level-4) with corresponding categories (K0–K4) for prosthetic feet.1,2 Prosthetic prescription and subsequent reimbursement frequently mandates that the amputee’s assigned MFCL correspond to a prosthetic foot that has the same class assignment. However, to date, there has been little objective data demonstrating the functional correlation between MFCL and the assignment of prosthetic components.
DMERC prosthetic policy definition of foot/ankle assemblies by Medicare Functional Classification Levels.
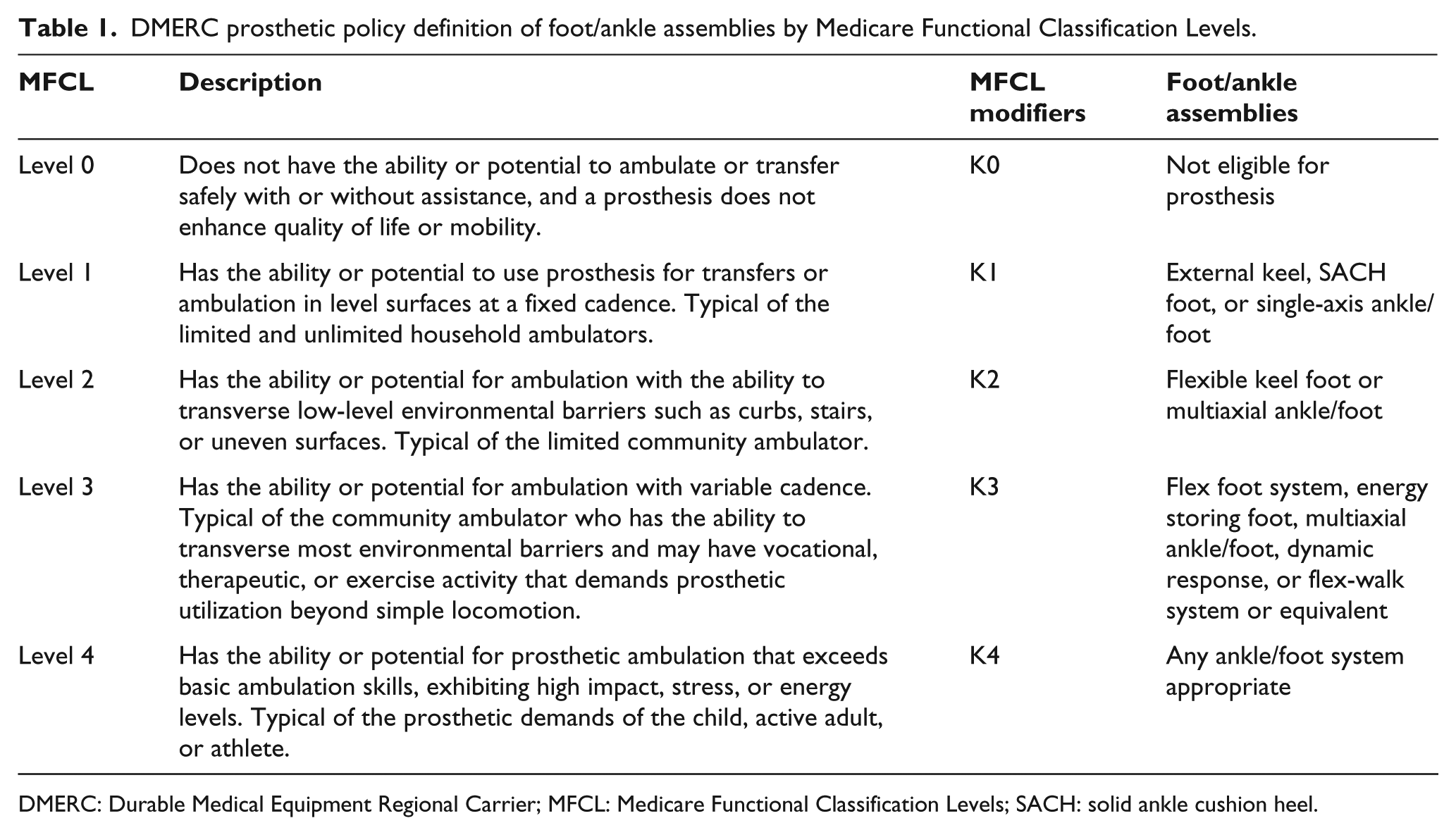
DMERC: Durable Medical Equipment Regional Carrier; MFCL: Medicare Functional Classification Levels; SACH: solid ankle cushion heel.
Unilateral transtibial amputees (TTAs) have a tendency to load the intact limb more than the prosthetic limb during level ground walking.3,4 The resulting kinetic asymmetry is influenced by prosthetic gait training 5 and the category of prosthetic foot used.5–7 Comparisons between level ground walking and incline/decline walking reveal higher demands on the musculoskeletal system and greater ground reaction forces (GRFs) during ramp ambulation in non-amputees. 8 If TTAs have higher intact limb loads during level walking and the non-amputee population experiences greater forces during incline/decline walking, it would stand to reason that during incline/decline walking TTAs would load their intact limb more than level walking and the asymmetry in forces would be magnified.
The only related study found on ramp GRFs with TTAs reported that elderly unilateral TTAs (K-Level-2) who used a solid ankle cushion heel (SACH) foot (category K1 foot) to negotiate ramps experienced significantly higher GRFs on the intact limb compared to the prosthetic limb. 9 They also exhibited a shorter single limb support time on the prosthetic limb than the intact limb. The authors attributed the kinetic and temporal asymmetry to the design features of the SACH foot, such as its limited stance phase ankle motion and lack of power generation. 9 Dynamic response (DR) prosthetic feet (category K3) have greater energy return and provide greater ankle dorsiflexion during stance period than the SACH foot because of their carbon fiber composition and “J-shaped” ankle design.10,11 A K3 prosthetic foot with a J-shaped ankle has been shown to promote greater symmetry in external work (SEW) during level walking in K-Level-2 amputees due to its ankle design and a heel-to-toe footplate. 5 To date, influence of foot design related to the prosthetic foot category on SEW during incline and decline walking in unilateral TTAs has not been investigated.
Traditional methods of assessing lower limb loading involve analyzing GRFs at discrete points during a gait cycle. Since the lower limbs experience variable GRFs during the stance period, assessment of forces at discrete points does not provide a complete picture of the consequences of loading throughout the entire stance period. Furthermore, traditional methods using direct comparisons of discrete events between prosthetic feet have not consistently demonstrated the sensitivity to detect significant differences between feet during level walking.12,13 The SEW measure has been employed as an alternative to traditional biomechanical measures for assessing kinetic and functional differences between prosthetic feet.5,14
External work is the change in energy of the body center of mass (CoM) that is brought about by GRFs. 14 External work can be calculated from the displacement of the CoM and the GRFs applied to the CoM during the entire stance period. 14 The SEW measure calculates external work by the intact and prosthetic limbs and generates an index of symmetry between the limbs. This measure determines collectively the similarities in GRFs, CoM displacement, and step time between the intact and prosthetic limbs. While the SEW measure has been successfully used to detect functional differences between prosthetic feet during level walking and stair negotiation, ramp ascent and descent would be another appropriate application.5,15
The purpose of this study was to determine the functional differences, as measured by SEW, between four categories of prosthetic feet during ramp ascent and descent in K-Level-2 and K-Level-3 unilateral TTAs. It was hypothesized that following standardized ramp training, unilateral TTAs will demonstrate differences in SEW values between four categories of prosthetic feet during ramp ascent and descent. Amputees classified with these functional levels were selected because they represent potential ramp ambulators who may benefit from the design proprieties of the four test prosthetic feet.
Methods
The study protocol was reviewed and approved by the Institutional Review Board at the Miami VA Medical Center and informed written consent was obtained from all subjects prior to study enrollment. The inclusion criteria for study participation were males and/or females between the age 40 and 65 years with limb loss related to dysvascular reasons, trauma, and tumor and who wore a comfortably fitting prosthesis for at least 6 months. All subjects were able to negotiate ramps independently without an assistive device. Potential subjects were screened by a physician and prosthetist and were excluded if they had any medical conditions or prosthetic limitations that would cause pain or a potential health risk during the study. Data collection was started upon physician and prosthetist clearance. The study was conducted in two phases: Phase I—Reliability study and Phase II—Intervention study.
Reliability study
Since the reliability of F-scan sensors (Tekscan Inc., Boston, MA, USA) has only been established for level walking in TTAs, 5 test–retest reliability of these sensors was determined during incline and decline walking with five unilateral TTA subjects (Table 2). The mean (standard deviation (SD)) age and time since amputation of the subjects were 55.84 ± 6.5 years and 22.4 ± 18.8 months, respectively. The median (range) age and time since amputation were 57.5 (43–64) years of age and 21 (6–72) months, respectively. The same team of researchers performed sensor calibration and data collection using previously validated procedures.16,17 During each testing session, a new F-scan sensor was individually prepared for each subject’s standardized shoe provided by the laboratory. Sensors were warmed up inside the shoes for 10 min. 16 They were then calibrated using the manufacturer recommended calibration and a force plate calibration with two Kistler force plates embedded in a 10-m-long level walkway. Vertical GRFs from force plates and F-scan sensors were compared and a calibration factor for F-scan sensors was calculated, as described by Mueller et al. 17 Data were collected for 10 s at a sampling frequency of 50 Hz. Subjects then ascended and descended a 24-foot-long custom fabricated wooden ramp, inclined at 5°—designed per the Americans with Disabilities Act guidelines—without using handrails. They were tested twice within a 48- to 72-h period using standardized shoes (Aetrex Ambulator, type T1220) and socks. Intraclass correlation coefficient (ICC) was used to determine the correlation between test–retest SEW values.
Demographic characteristics of subjects for the test–retest reliability study.
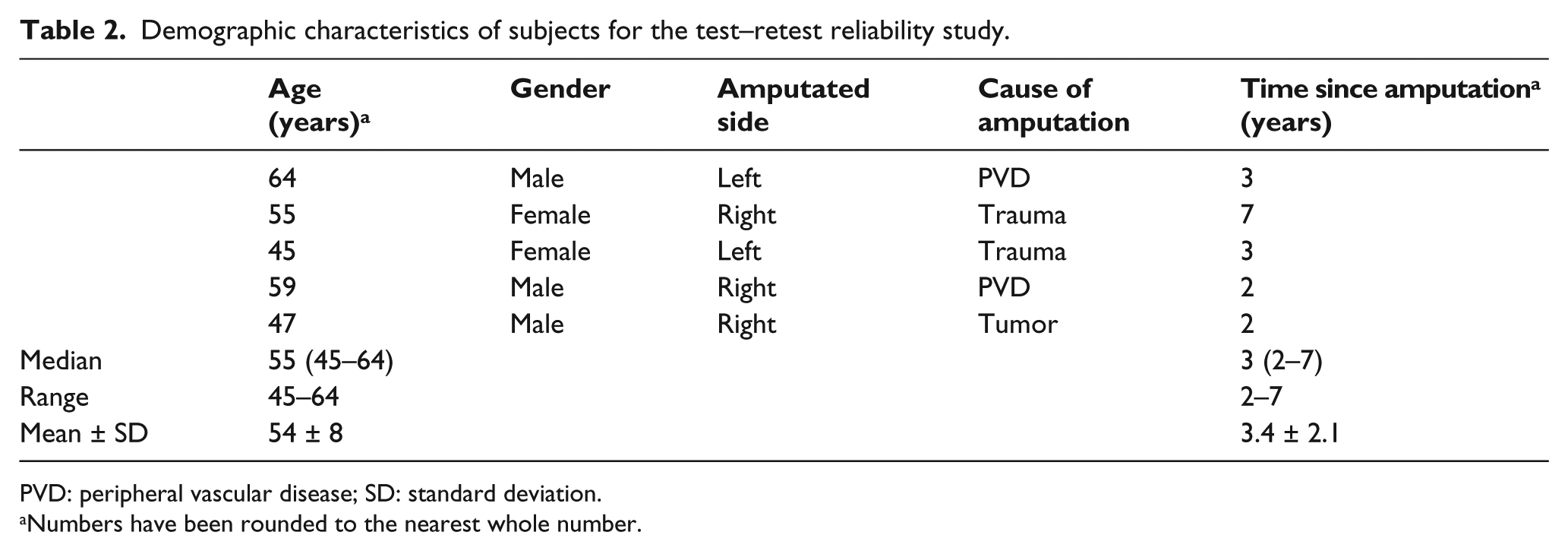
PVD: peripheral vascular disease; SD: standard deviation.
Numbers have been rounded to the nearest whole number.
Intervention study
Ten unilateral TTAs (five K-Level-2 and five K-Level-3 subjects) (Table 3) underwent six testing sessions to test four categories of prosthetic feet. The test feet were: (1) SACH foot (Kingsley Manufacturing Co., Costa Mesa, CA, USA), (2) Stationary Attachment Flexible Endoskeleton (SAFE) foot (Campbell-Childs Inc., White City, OR, USA), (3) Talux foot (Ossur hf, Reykjavik, Iceland) and (4) the Proprio-Foot (Ossur hf) (microprocessor ankle). These four prosthetic feet were selected to represent each category of foot as described in Table 1, that is, K1—the SACH foot identified by name in the Durable Medical Equipment Regional Carrier (DMERC) prosthetic policy definition of foot/ankle assemblies; K2—the SAFE foot a truly flexible keel foot; K3—the Talux foot because it is a Flex-Foot with a J-shaped ankle and DR design (also named by DMERC) combined with multiaxial capabilities because of the elastomer block. The Proprio-Foot, a K3 foot, was included as a microprocessor-controlled ankle (MPA) that provides active dorsiflexion and plantarflexion during ramp walking. Data collection procedures were identical to the reliability study described above.
Demographic characteristics of subjects for the intervention study.
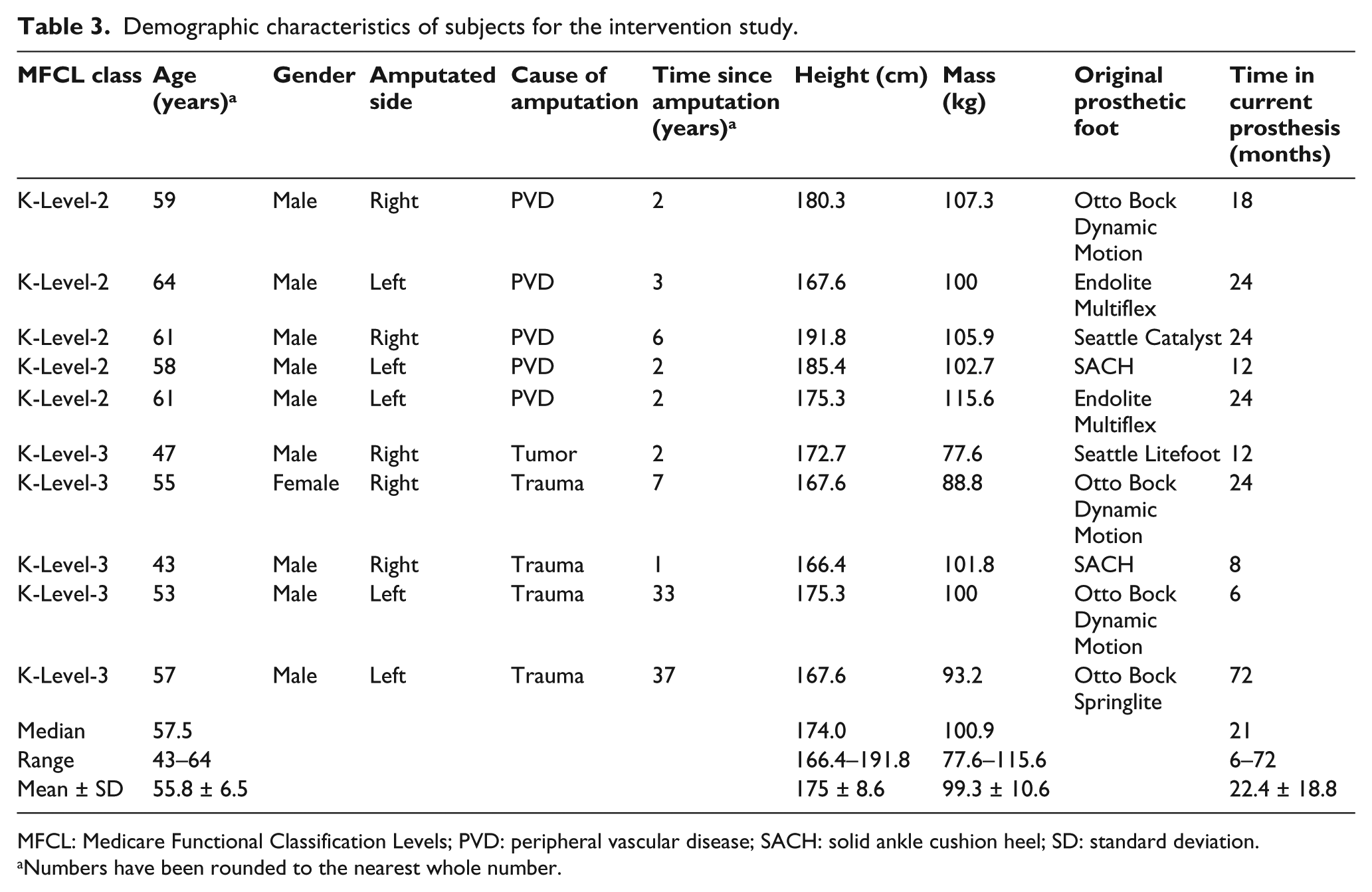
MFCL: Medicare Functional Classification Levels; PVD: peripheral vascular disease; SACH: solid ankle cushion heel; SD: standard deviation.
Numbers have been rounded to the nearest whole number.
At Session 1 (Baseline), subjects used their existing prosthetic socket and foot. There was a 2-week period between Sessions 1 and 2, during which subjects received up to 4 h of standardized functional prosthetic training, as described below. During this time period, their residual limb was also scanned to create a computer-aided design (CAD) image (BioSculptor; Maramed Inc., Miramar, FL, USA) which was used to fabricate a total surface bearing socket having suction suspension with an Iceross Seal-in liner (Ossur Inc.) or a cushion liner and external sleeve. The purpose of standardizing the socket design and suspension was to minimize the socket-related variables that could influence gait performance during testing. During Session 2 (Training), subjects were tested again in their existing socket and foot to determine the effects of training on their gait and were fit with the study socket and one of the four randomized test feet (F1). The same study socket was used for subsequent testing sessions and throughout the duration of the study. During the 10- to 14-day accommodation period with F1, they participated in 1–4 h of training to learn to maximize the use of this foot design. Any issues with socket fit or alignment were addressed within 48 h of notification and all prosthetic or training-related issues were resolved during one return visit. At testing Session 3, effects of F1 on subjects’ gait were measured. Following testing, subjects were fit with the randomly selected second test foot (F2) and again were given 1–4 h of foot-specific training during the 10- to 14-day accommodation period. The effects of F2 on subjects’ gait were determined in Session 4. The same testing and training procedure was repeated for the third and fourth test feet during Sessions 5 and 6, respectively. All socket fittings and prosthetic alignment procedures were performed by the same board-certified prosthetist.
Standardized functional prosthetic training was administered to minimize gait deviations resulting from habit or lack of training and also to maximize the use of each prosthetic foot’s functional properties. All subjects were able to ascend and descend the ramp leg-over-leg without the use of the handrail although they were instructed to hold onto the handrail if required for safety. For ramp ascent, subjects were instructed to place each foot flat on the surface in front of the other foot, keeping a width of approximately 10 cm between feet. During training, cues were given to assist with the maneuver when necessary, such as roll over the toe, keep the trunk flexed forward, and keep the movement continuous (i.e. do not hesitate). No cues were given during testing. During descent, the physical therapist used a gait belt to slow the transition of body weight over the prosthetic foot. Verbal cueing was provided to encourage more time over the prosthetic heel (for the cushion feet design) and over the forefoot for maximum deflection of the footplate. With all four prosthetic feet, a slow and controlled decent down the ramp with both limbs was promoted. During each 1-h training session, subject’s gait proficiency was assessed on predefined criteria. They were trained only in areas in which training was needed. When they satisfactorily met the predefined criteria, training was concluded. All training sessions were standardized and were administered by the same physical therapist.
Data analysis
After the subject’s third step with the prosthetic limb from ascent or descent initiation, the next three consecutive steps with both the intact and prosthetic limbs were utilized for work calculations. External work was calculated using the following equation
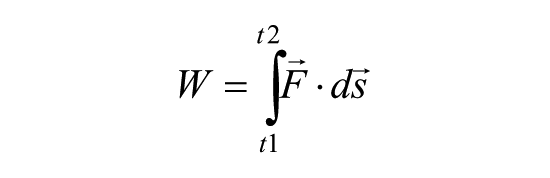
where W is the work in Joules,
where av is the acceleration in the vertical direction (m/s2), Fv is the vertical GRF (N), m is the body mass (kg), and g is the acceleration due to gravity (m/s2).
The acceleration thus calculated was integrated to obtain CoM velocity in the vertical direction. By integrating velocity and using the geometry of the ramp, vertical CoM displacement was calculated. Since F-scan sensors measure only the normal force, vertical force was obtained from normal force by using cosine of 5°, which was the angle of the ramp.
SEW between limbs was calculated for each stride using the following equation, 14 and a mean SEW value was obtained by averaging the three strides

where SEW is expressed in percentage; WI is the work done by the intact limb due to vertical GRF, in Joules; WP is the work done by the prosthetic limb due to vertical GRF, in Joules.
A SEW value of 100% indicates equal work by each limb, value greater than 100% indicates more work by the prosthetic limb, and a value less than 100% indicates more work by the intact limb. Shapiro–Wilk test for normality of SEW values was performed for the sample based on K-level, at Baseline, after initial prosthetic training, and after prosthetic foot prescription. The intraclass correlation coefficient (ICC) was calculated to determine the test–retest reliability of the SEW values using Model 1,3. A paired t-test was used to determine differences in gait symmetry between the Baseline and Training sessions to test the effect of standardized functional prosthetic training. Repeated measures analysis of variance (ANOVA) was used to determine differences between feet after completion of the training protocol. When ANOVA revealed significant differences, for post hoc analysis, pairwise comparisons using related pairs t-tests were used to identify the source of differences. The critical alpha was set at 0.05.
Results
Subject characteristics for the reliability and intervention studies are described in Tables 2 to 4, respectively.
Mean ± SD SEW values (in percentage) in K-Level-2 and K-Level-3 amputee subjects before and after standardized gait training for ramps.
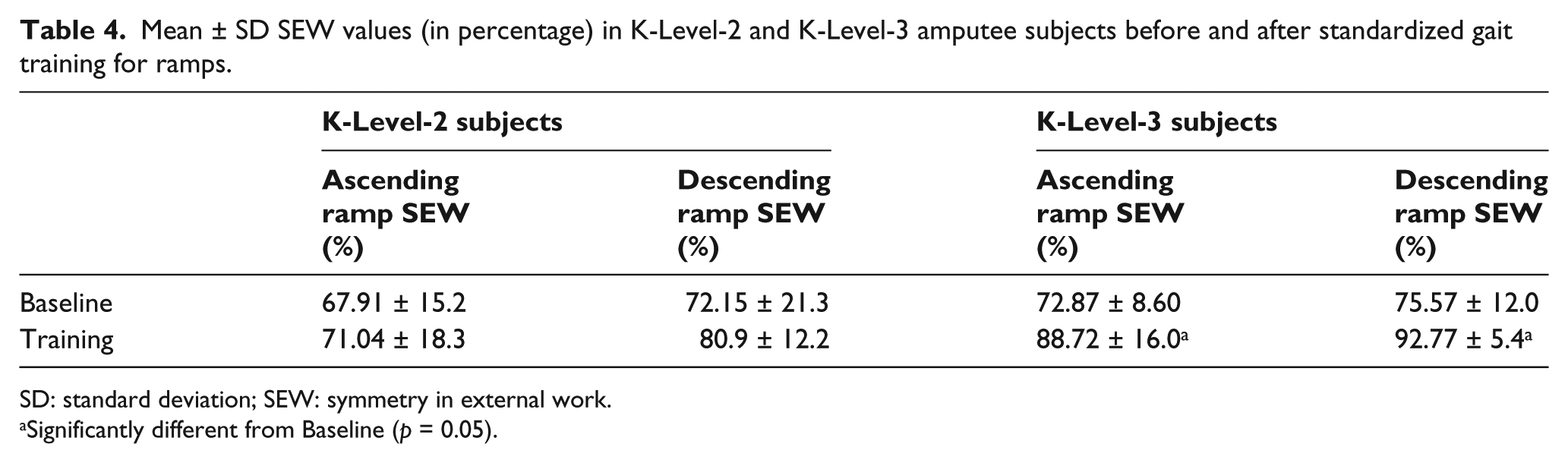
SD: standard deviation; SEW: symmetry in external work.
Significantly different from Baseline (p = 0.05).
Shapiro–Wilk test of normality
The results for the Shapiro–Wilk test for normality indicate that the SEW values were normally distributed for K-Level-2 subjects during decline walking and for K-Level-3 subjects during incline and decline walking. The SEW values for K-Level-2 subjects during incline walking were normally distributed for all conditions except for the SACH foot (p = 0.02).
Reliability study
The ICC for test and retest SEW values was 0.87 for ramp ascent and 0.89 for ramp descent. The high ICC indicated that SEW can be measured consistently using F-scan sensors with unilateral TTA’s walking on ramps and also corroborated the stability of subjects’ gait during ascent and descent.
Intervention study
Tables 4 and 5 show the mean (SD) SEW values during ramp ascent and descent for both groups at the six testing sessions.
Mean ± SD SEW values (in percentage) for K-Level-2 and K-Level-3 amputee subjects while ascending and descending a 24-foot ramp with four test feet.
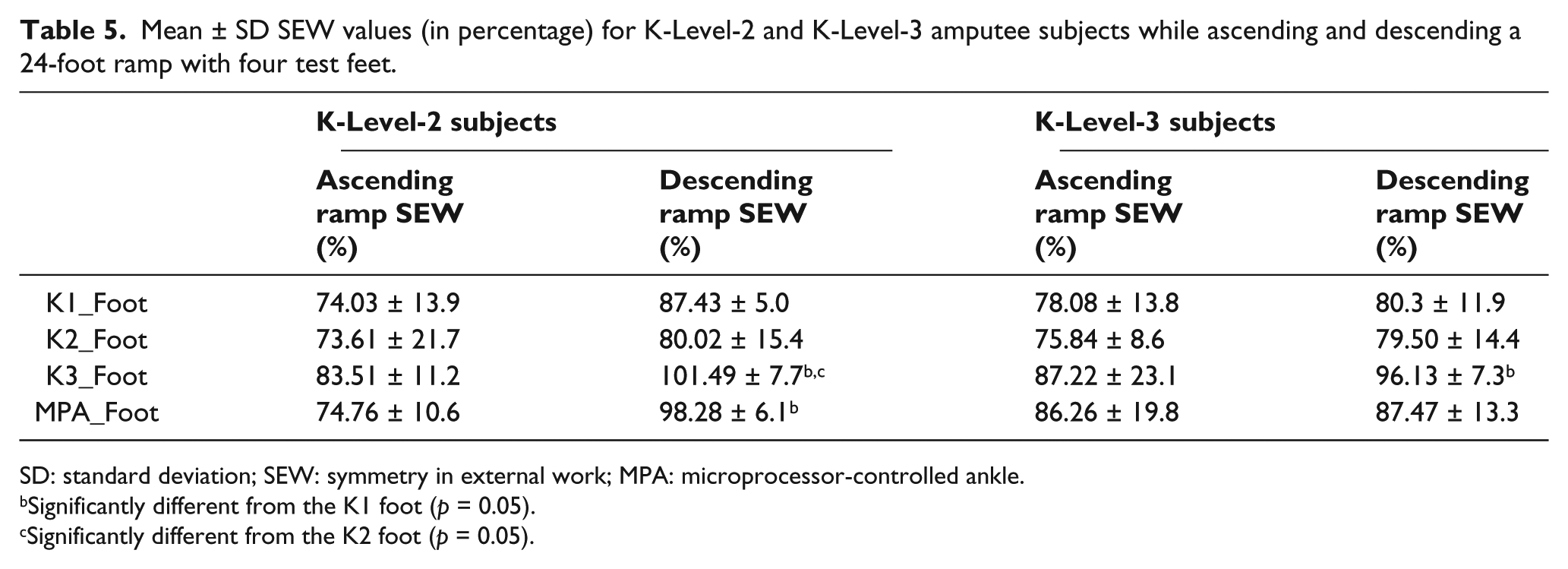
SD: standard deviation; SEW: symmetry in external work; MPA: microprocessor-controlled ankle.
Significantly different from the K1 foot (p = 0.05).
Significantly different from the K2 foot (p = 0.05).
Ramp ascent
After receiving standardized functional prosthetic training, K-Level-3 subjects had a significant (p < 0.05) increase in SEW values (16% increase over Baseline). In the K-Level-2 subjects, there was a 5% increase in SEW values following Training, which was not statistically significant (p < 0.05). There were no significant differences between any pair of test feet.
Ramp descent
Following prosthetic training, there was a significant increase in SEW values for the K-Level-3 group (23% over Baseline), while in the K-Level-2 group (12% over Baseline) increase in SEW was not statistically significant (p < 0.05). In K-Level-2 subjects, a higher SEW value with the Talux K3 foot (p < 0.05) was found when compared to both the K1 and K2 feet. The MPA foot had significantly higher SEW than the K1 foot (p < 0.05) and the difference in SEW between MPA foot and the K2 foot did not reach statistical significance (p = 0.06). In the K-Level-3 subjects, SEW values were significantly higher with the K3 foot (p < 0.05) when compared to the K1 foot. Again the K3 foot approached statistical significance, but was not significantly different from the K2 foot (p = 0.07). The Talux foot had the greatest SEW values in four of the five K-Level-2 subjects and in four of the five K-Level-3 subjects. There were no significant differences between the K3 foot and the MPA foot.
Discussion
Ramp ascent
During ramp ascent, there were no significant differences in SEW values between prosthetic feet in either K-Level-2 or K-Level-3 groups; however, the K3 and MPA feet resulted in greater SEW values in the majority of subjects in both groups. Vickers et al. 9 reported significant variations in GRFs during incline and decline walking, not only with the prosthetic limb but also with the intact limb. The results of this study demonstrate that adaptations that impact external work due to vertical force while ascending a 5° ramp are not influenced by the type of prosthetic foot used. Although not an original objective of the study, it was found that the prosthetic training administered to the subjects resulted in numerically higher SEW values for the K-Level-2 subject group and significantly higher SEW values for the K-Level-3 group. The methodology for this study ensured that all subjects received training, specific to each prosthetic foot’s design in order to maximize their performance with the foot’s functional properties. As a result, the improved symmetry following the ramp ascent was maintained with all test feet.
During incline walking, lower limb muscles generate power that is required to move the body’s CoM against the force of gravity. Since the test prosthetic feet were not designed to generate power, external work with the prosthetic limb may have been accomplished through the use of residual limb musculature. During the standardized prosthetic training, subjects were taught to appropriately contract the knee and hip extensor muscles as well as properly contract their residual limb muscles to maintain balance and use each prosthetic foot as designed for performing the activity. Therefore, following the completion of the training protocol, SEW values improved in both K-Level-2 and K-Level-3 subjects and the test feet were not found to be different during ramp ascent.
Contrary to the results of Fradet et al. 18 —who used a 7.5° slope—this study did not find a significant difference between the Proprio-Foot and other test feet during incline walking. The benefits of active dorsiflexion of the Proprio-Foot may become more apparent on ramps with higher incline angles (e.g. a 7.5° slope, as described by Fradet et al.) or a larger sample size may be needed to detect significant differences with the Proprio-Foot on a 5° incline.
Ramp descent
Both the K-Level-2 and K-Level-3 groups demonstrated highest SEW values with the K3 foot, with statistically significant differences between the K3/MPA feet and K1/K2 feet. Standardized training also resulted in statistically higher SEW for the K-Level-3 group and numerically higher symmetry in the K-Level-2 group. The differences in SEW values could be attributed to the design and functional properties of the K3 feet.
The K3 foot (Talux foot) used in this study has a dynamic heel that promotes plantarflexion during early stance and a J-shaped ankle design that simulates anatomical tibial advancement (or dorsiflexion) as the body progresses over the stationary foot in late stance. 19 Macfarlane et al. 20 reported that amputees capable of balancing over the forefoot during late stance with a Flex-Foot were able to take a slower and longer step with the intact limb resulting in greater symmetry during ambulation. The similarity in designs between the Flex-Foot and the Talux foot indicates that the temporal gait characteristics seen with these feet would be comparable. In this study, at the time of training, subjects were instructed to balance over the prosthetic forefoot and to take a controlled, slower step with the intact limb. The combination of training and functional properties of the prosthetic foot resulted in similar time needed to reach the peak force (loading time) with the intact and prosthetic limbs, in both subject groups (Table 6). Also, the forward deflection of the J-shaped ankle spring likely permits a systematic lowering of the CoM in terminal stance, which allows a smooth transfer of weight to the intact limb. This functional property of the K3 foot resulted in reduced loading of the intact limb as the first peak of the vertical GRF curve with the K3 foot found to be lower than K1 and K2 feet in both subject groups (Table 7). The symmetry in vertical GRF peak and loading times between the intact and prosthetic limbs further corroborates the high SEW values recorded with the K3 foot.
Mean ± SD time required to reach the first peak of vertical ground reaction force (expressed as percent of gait cycle) in K-Level-2 and K-Level-3 amputee subjects while descending a 24-foot ramp.
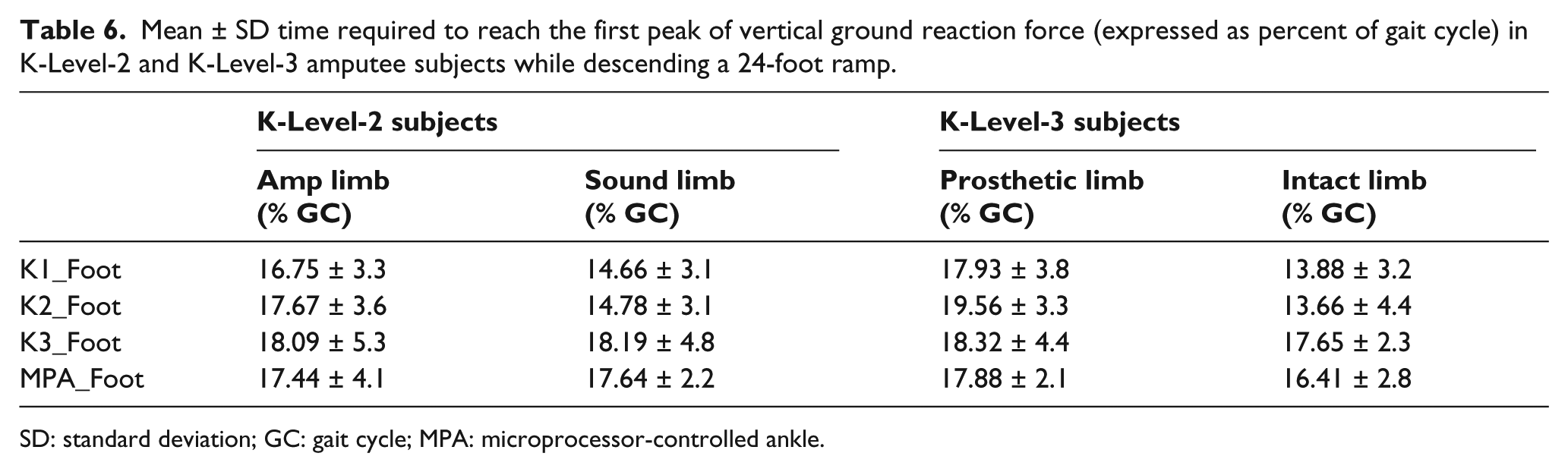
SD: standard deviation; GC: gait cycle; MPA: microprocessor-controlled ankle.
First peak of vertical ground reaction force (mean ± SD), in percent body weight of K-Level-2 and K-Level-3 amputee subjects while descending a 24-foot ramp.
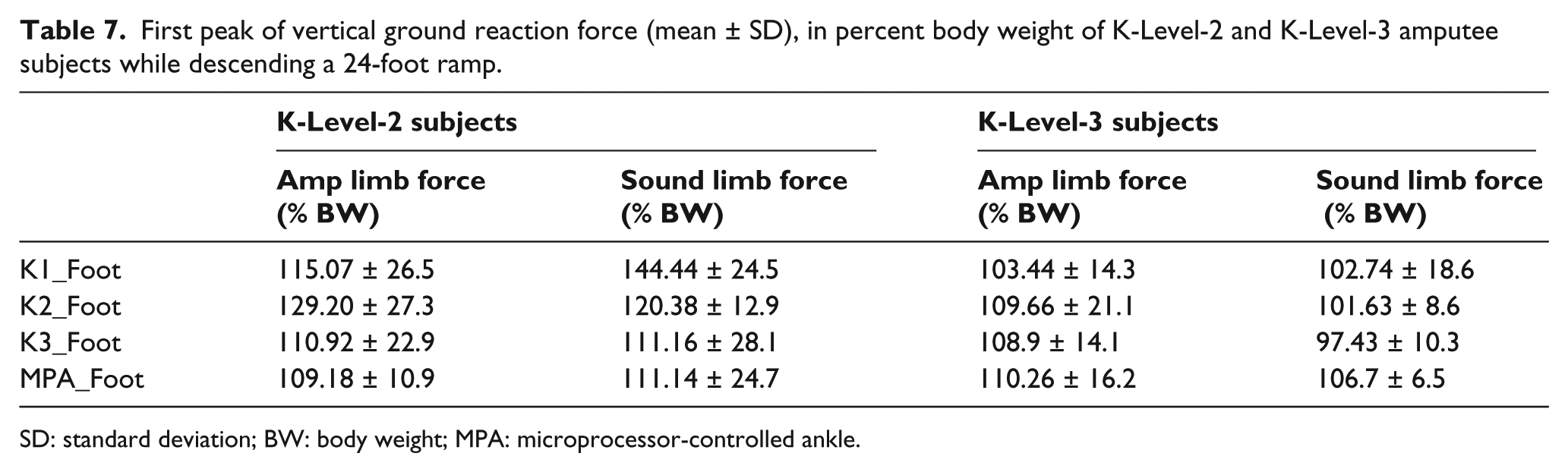
SD: standard deviation; BW: body weight; MPA: microprocessor-controlled ankle.
The MPA foot (Proprio-Foot) also has a heel–toe footplate design, which permits late stance stability, and an MCA joint that actively plantarflexes in late swing to match the grade of the slope. The Proprio-Foot’s ankle joint has limited dorsiflexion during the stance period which likely impacts the transition of body weight over the stationary foot during the late stance period. The differences in functional ankle dorsiflexion between the K3 and MPA feet may explain the observed differences in SEW values, vertical GRF peak values, and loading times between these DR feet (Tables 4 to 7).
In both the non-DR feet, the pylon is directly attached to the foot without a mechanical axis at the ankle. This rigid ankle design eliminates functional ankle dorsiflexion during the stance period of gait. The absence of dorsiflexion during stance causes premature knee flexion resulting in an early heel rise. 19 Because of the shorter, flexible keel, the body tends to progress more rapidly to terminal stance as the CoM essentially runs out of base-of-support. The maximum forward progression of the center of pressure (CoP) (expressed as a percentage (%) of foot length) was approximately 70% and 79% with the SACH and SAFE, respectively, compared to 85% with Talux/Proprio feet (Table 8). The resulting instability during late stance likely caused the contralateral limb to advance more rapidly to catch the body as it fell forward. The sudden deceleration of body CoM as it transitioned from the prosthetic to intact limb resulted in a greater vertical GRF peak on the intact limb—particularly in the K2 group—and a faster loading time on the intact limb (Tables 6 and 7). The functional properties of non-DR feet thus resulted in greater work by the intact limb and lower SEW values with K1/K2 feet in both groups. These results suggest that K3 prosthetic feet can have significant functional benefits for those K-Level-2 unilateral TTAs who frequently negotiate ramps, as the K3 feet promote greater SEW during decline walking.
Forward progression of the center of pressure (mean ± SD), expressed as a percentage of foot length in K-Level-2 and K-Level-3 amputee subjects while descending a 24-foot ramp.
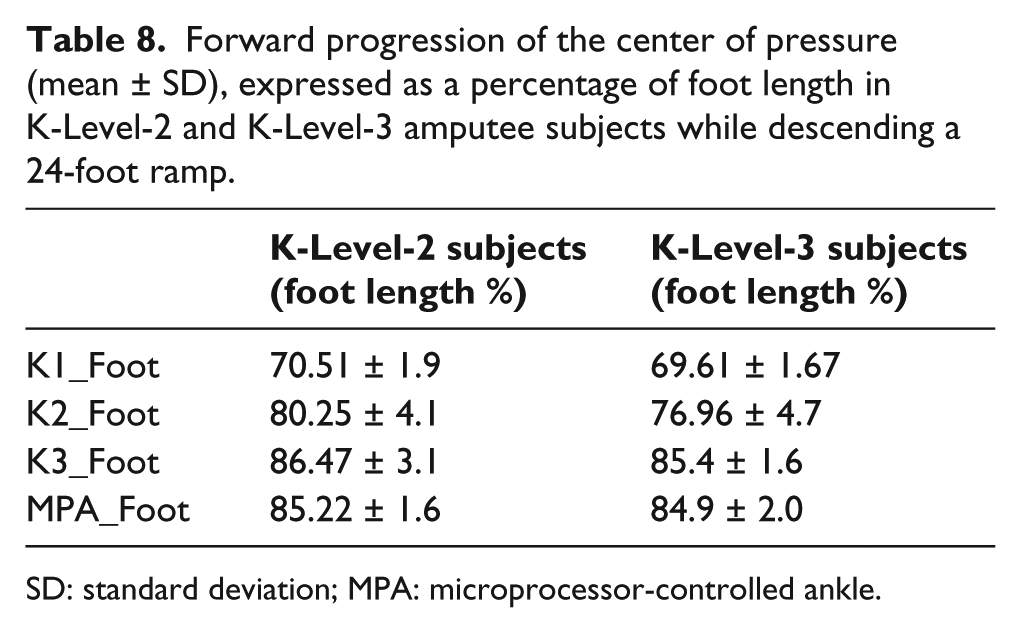
SD: standard deviation; MPA: microprocessor-controlled ankle.
The SEW measure determines the similarities in GRFs, CoM displacement, and step time between the intact and prosthetic limbs. Since these gait parameters are influenced by the design related to prosthetic foot category, the foot design that mimics the function of physiological foot/ankle during ramp walking would result in greater inter-limb symmetry. In addition to the contributions from the prosthetic foot, the use of residual limb musculature can significantly influence gait dynamics while ascending and descending a ramp. During ramp descent, the SEW measure is correlated with traditional methods of gait assessment, such as the vertical GRF peak (r = −0.5) and loading time of the intact limb (r = 0.9), as well as the maximum forward progression of the CoP on the prosthetic foot (r = 0.7). Subjects with low SEW values demonstrated greater vertical GRF peak and faster loading on the intact limb, as well as shorter CoP progression on the prosthetic foot. However, unlike these traditional methods—which assessed discrete points of the stance period and could only indicate trends about prosthetic feet—the SEW measure was able to detect statistically significant differences between feet. As the SEW measure combines different gait parameters during the entire stance period into a single value, it appears to have the sensitivity for detecting subtle gait differences between prosthetic feet on ramp incline and decline.
Since increased loading of the intact limb and high loading rates are associated with the higher prevalence of osteoarthritis in the TTA population, 21 the SEW measure could potentially be used as a measure for determining the efficacy of prosthetic feet in a clinical setting. Currently available self-report outcome measures only assess perceived difficulty associated with ramp ambulation and the performance-based measures do not quantify movement during incline and decline walking. Since the SEW measure can quantify gait asymmetry during ramp ambulation, it could be used to supplement existing clinical outcome measures. With the recent advancements in wireless in-sole technology and mobile computing, the SEW measure could potentially be implemented in a clinical setting relatively easily. Future research to test this measure on a larger population of subjects with different amputation levels is needed to further determine the clinical applicability of this measure with regard to different pathologies such as osteoarthritis or neuropathic foot disease.
Limitations
The study was underpowered in terms of sample size. While SEW values were significantly different between prosthetic feet during ramp descent, differences during ramp ascent may not have been evident due to a relatively small size. In addition, the accommodation time with prosthetic feet and minimal exposure to incline/decline ambulation during the accommodation period due to geographical topography of Miami may have reduced the opportunities for practice between testing sessions. Standardized prosthetic ramp training had an impact on performance because it was specific to the design of each foot and promoted use of each component, such as a cushion heel, rubber toes, heel-to-toe footplate, foot keel, J-shaped design, and microprocessor ankle. Since ramp-specific training is not always available in all clinical environments, the clinically observed differences between feet may vary as some feet could be more intuitive to use than others. Future work could examine the differences of SEW in TTAs who received training to maximize the use of a prosthetic foot’s design properties for ramp ambulation as opposed to those TTA who naturally adapted to prosthetic foot without formal training; that is, is there a prosthetic foot design that promotes SEW during ramp ambulation and does not require training?
Similar to other commercially available in-sole sensor systems, the F-scan sensors can only measure normal forces during gait. In able-bodied gait on sloping surfaces, the magnitude of normal and vertical forces is very similar—differing by less than 1%—while ascending and descending a 5° ramp. 20 The shear force also has a component in the vertical direction, which is the trigonometric sine of the angle of the slope. For a 5° ramp, this component of shear force has a negligible contribution to the vertical force, and hence was ignored in this analysis. Future studies could examine SEW differences between feet at higher grades of ramps, as the vertical and shear GRFs change appreciably with the angle of inclination. 8
The inability of F-scan sensors or any other currently available in-sole sensor to measure shear forces limits our ability to include shear values in the SEW calculation. Since the GRFs during ramp negotiation are three-dimensional in nature and the CoM moves in all three planes, total work during ramp ambulation could be computed using both the vertical and shear forces. Although the magnitude of shear GRFs is much lower than the vertical GRFs, 22 the contribution of work due to shear forces on the total work during ramp ascent and descent is unknown. Moreover, subjects were asked to walk at a self-selected speed and walking speed was not controlled during incline or decline walking. While walking speeds may have influenced SEW values, the effect of speed on normal and shear GRFs in unilateral TTAs walking on slopes is unknown. Future work to include shear forces in the SEW calculation may be beneficial for determining the aggregate effects of forces on the foot and lower limb during ramp ambulation.
Conclusion
SEW was found to be different between four categories of prosthetic feet during ramp descent of K-Level-2 unilateral TTAs. The design features of K3 DR prosthetic feet improved dynamic gait symmetry in K-Level-2 subjects, while descending a 5° ramp compared to K1 and K2 feet. The J-shaped ankle design of the K3 foot (Talux) resulted in significantly greater SEW values than both the K1 and K2 feet (SACH and SAFE, respectively), while the microprocessor ankle (Proprio-Foot) had a significantly greater symmetry than the K1 foot. The test feet were not significantly different in either K-Level-2 or K-Level-3 subjects while ascending the ramp. In K-Level-3 TTAs, SEW values increased significantly following standardized gait training for ramp ascent and descent. Study results suggest that both K-Level-2 and K-Level-3 amputees experience greater SEW from a K3 prosthetic foot with a J-shaped ankle and heel-to-toe footplate design as well as a microprocessor foot while descending ramps.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This material is the result of the work supported with resources and use of the Bruce W Carter Department of Veterans Affairs Medical Center, Miami, FL, USA. The authors would like to thank Ossur® Americas for their support of this research study and the South Florida Veterans Affairs Foundation for Research and Education, Miami, FL, USA, for administering the research project.