
Abstract
Background:
Despite increasing knowledge about the potential benefits of advanced user-controlled technology, the decision about switching an individual prosthesis user from a non-microprocessor prosthetic knee to a microprocessor prosthetic knee is mainly based on clinician’s experience rather than empirical evidence.
Objectives:
To demonstrate the utility of single-subject design and data analysis for evaluating changes in temporal-spatial gait characteristics between walking with a non-microprocessor prosthetic knee and microprocessor prosthetic knee.
Study design:
Single-subject ABA/BAB design.
Methods:
Seven non-microprocessor prosthetic knee users (all men, age 50–84 years, 3–40 years post-amputation) were transitioned through the ABA or BAB phases (A-NMPK, B-MPK, 5 weeks each). Four weekly gait evaluations were performed at three self-selected speeds with an electronic walkway. The non-microprocessor prosthetic knee–microprocessor prosthetic knee differences in stride length–cadence relationship, prosthetic weight acceptance, single-limb support, and step width were evaluated for each subject using the “non-overlap of all pairs” statistical method.
Results:
Most subjects improved temporal-spatial gait while on the microprocessor prosthetic knee; in only one subject, none of the 10 gait parameters were in favor of the microprocessor prosthetic knee. In the BAB group, longer use of the microprocessor prosthetic knee was associated with shorter prosthetic weight acceptance and longer single-limb support times across three speeds. Step width either improved with the microprocessor prosthetic knee or remained unchanged in most subjects.
Conclusion:
The evidence of individual subject improvements in gait coordination, greater reliance on the prosthetic side, and better stability with the microprocessor prosthetic knee than non-microprocessor prosthetic knee over a range of walking speeds demonstrate the practical utility of the single-subject method in clinical decision-making.
Clinical relevance
The results demonstrate the use of the single-subject method for examining person-specific differences in temporal-spatial gait characteristics between walking with a non-microprocessor prosthetic knee and microprocessor prosthetic knee at three self-selected speeds. The method proved feasible and reliable for documenting changes in gait at the individual level, which is relevant for clinical practice.
Keywords
Background
Microprocessor prosthetic knees (MPKs) offer many advanced features over non-microprocessor prosthetic knees (NMPKs), particularly the ability to adapt the control of stance and swing to different speeds. A growing body of literature suggests that MPKs are superior to NMPKs in terms of improving level and slope walking, stair climbing, and balance as well as reducing energy expenditure, cognitive effort, and risk of falls, with overall better user satisfaction (for a summary, see reviews1,2 and recent original reports3–6). These conclusions emerged out of studies that employed group designs that may be prone to different biases. For example, some studies used a cross-sectional between-subject design in which a group of NMPK users was compared to a group of MPK users. 7 This approach requires that samples of NMPK and MPK users are matched on key factors possibly affecting outcomes (e.g. age, duration of prosthesis use, acclimation time, activity level, cognitive capacity, medical co-morbidities), which is not easy without randomization and larger sample sizes. Recent studies employed a within-subject crossover design where the same group of subjects was examined with NMPK and then switched to MPK,3–5 which overcomes many drawbacks of the between-group design and provides more confidence in conclusions. However, in both between- and within-subject studies, data are analyzed for the entire group, producing results that are not readily translated into clinical practice for several reasons. First, studies with small samples are often underpowered and known to exaggerate the effect of intervention both in individual reports and meta-analyses. 8 Second, large inter-subject variability in results 4 often prompts post hoc sub-group or even individual level analyses5,9 that lead to conclusions of questionable validity. 10 Finally, the aggregate results reported for the group reflect an “average” outcome of an “average” subject, in terms of demographic and clinical characteristics, that is rarely encountered in real-world practice, making conclusions hardly transferable to a specific client.
An alternative to a group design is the single-subject or “N-of-1” design that is gaining increased recognition in the rehabilitation field.11,12 The main characteristics of single-subject designs are one or more phases of exposure to and withdrawal of intervention with serial assessments in each phase. This method allows for studying only one case or a series of cases with the same or different phase patterns. The single-subject method is preferred over underpowered group studies and recommended when reasonably expected recruitment or retention is less than 30, and particularly less than 10. 11 The relevance of this method is strengthened by advancing approaches to single-subject data analysis, which are well established in the literature and easy to perform. 13 Familiarity with this method is relevant for practitioners because the backbone of the single-subject design, systematic exposure-withdrawal of intervention and serial assessments, resembles clinical practice.
Thus, the objective of this study was to demonstrate the utility of the single-subject method in prosthetic research and clinical practice by evaluating temporal-spatial characteristics of gait over a range of self-selected speeds. Based on the potential advantages of MPKs, we hypothesized that the short-term use of an MPK, in comparison with an NMPK, would improve gait coordination and stability in above-knee prosthesis users. This would be evident by a stronger stride length–cadence relationship, lower percentage of the gait cycle spent in prosthetic weight acceptance (early double-support), greater percentage of the gait cycle spent in prosthetic single-limb support, and reduced step width. These hypotheses were tested in the framework of the single-subject method, using the ABA or BAB design for data collection and the “non-overlap of all pairs” statistical technique, in order to familiarize researchers and clinicians with this well established but not as much utilized approach in the field of orthotics and prosthetics.
Methods
Participants
Participants were recruited from the clinical population served by our institution under the supervision of one of the authors (C.W.). The inclusion criteria were age of >18 years; unilateral above-knee amputation; exclusive use of an NMPK for at least 1 year; comfortable socket fit with no skin breakdown; Medicare Functional Classification Level 2 (K2) or 3 (K3) (assigned by an experienced clinician and subsequently confirmed based on the Amputee Mobility Predictor (AMP) 14 ); and no cognitive dysfunction (based on the Mini Mental Status Examination) or general health problems that would prevent compliance with the study protocol. The planned sample size was 8 for the pragmatic reason of completing the study within the a priori scheduled time; of which 7 subjects were recruited and completed the entire study. The study was approved by the Methodist Rehabilitation Center’s Institutional Review Board for human research, and all subjects signed informed consent.
Study design
A single-subject experimental withdrawal protocol was used, 12 with either an ABA or BAB design. The subjects used their own NMPK during the A-phase and the study MPK during the B-phase (Rheo Knee® 3, supplied by Ossur ehf.). As such, the performance on their own NMPK, to which they were well adjusted, served as the baseline for evaluating changes after switching to the MPK. Three new Rheo 3 knees were made available by the manufacturer, and they were randomly allocated to the subjects. Rheo 3 offers both active stance and swing control that was predicted to impact the selected outcome measures. The same type of MPK was used in all subjects to avoid confounding the results with MPKs offering different functions.
Prior to data collection, subjects were evaluated by a certified prosthetist to ensure proper fit and alignment of their own NMPK. Any changes required to improve the current fit or later accommodate the MPK (e.g. alignment change, new socket coupling) were made at this time allowing at least 2 weeks to adapt before proceeding with the study. The socket, suspension, and foot were kept consistent throughout the study to limit additional confounding factors. Efforts were made to maintain consistent alignment for each knee throughout the study, with all changes documented, to reduce potential biases.
The baseline gait performance was evaluated while subjects used their own NMPK (initial evaluation session). Subsequently, each subject was allocated at random to either the BAB group (n = 4, heretofore designated as S1–S4) or ABA group (n = 3, S5–S7). The duration of each phase was 3 weeks, followed by a 2-week transition period. Each phase consisted of four weekly gait evaluation sessions. After the fourth evaluation session, the subject was switched to the other knee and entered another 2-week transition period. During this time, subjects were seen by a prosthetist and physical therapist as needed to ensure proper fit and facilitate accommodation. When first transitioning to the MPK, each subject was scheduled for one or more visits at the discretion of the physical therapist to ensure the safe use of the prosthesis. The entire study period was 13 weeks for the ABA group and 15 weeks for the BAB group (due to the additional 2-week transition period at the beginning of the study).
Data collection
A 6 m electronic walkway (Zeno Walkway®; ProtoKinetics, Havertown, PA) was used to record temporal and spatial footfall data during steady-state gait.15–17 A minimum of 1.2 m was allowed on each end for acceleration/deceleration. At each weekly session, subjects were instructed to walk first at their normal self-selected speed, which was followed by fast and slow self-selected speeds presented in random order (four passes at each speed). Subjects S1, S2, and S4 used their usual walking aid during assessments (Table 1).
Subject characteristics.
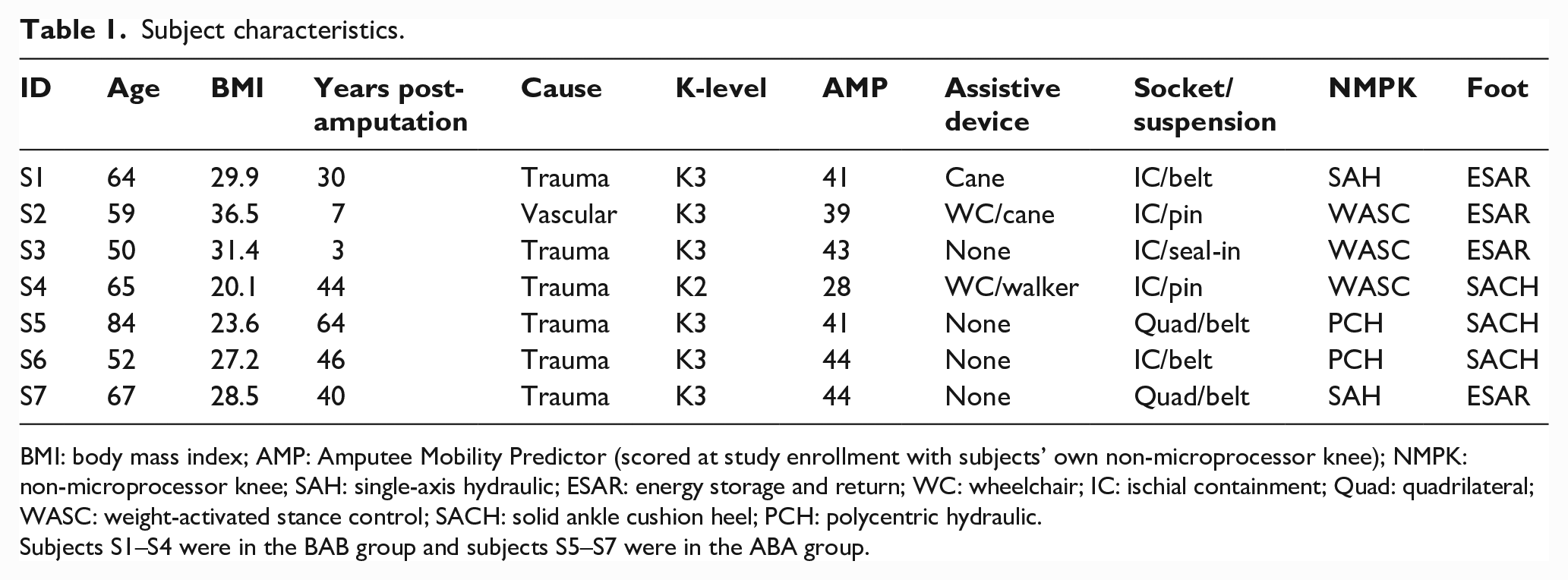
BMI: body mass index; AMP: Amputee Mobility Predictor (scored at study enrollment with subjects’ own non-microprocessor knee); NMPK: non-microprocessor knee; SAH: single-axis hydraulic; ESAR: energy storage and return; WC: wheelchair; IC: ischial containment; Quad: quadrilateral WASC: weight-activated stance control; SACH: solid ankle cushion heel; PCH: polycentric hydraulic.
Subjects S1–S4 were in the BAB group and subjects S5–S7 were in the ABA group.
Data processing
The data from the electronic walkway for each weekly session were processed using a custom program written in MATLAB® (Mathworks Inc., Natick, MA) to derive stride length (cm), instantaneous stride cadence (strides/min), step width (cm), and the percent of the gait cycle spent in early double-support and single-limb stance. Instantaneous stride cadence was calculated from individual stride times. Parameters were calculated with the prosthetic side as the lead foot. In addition to providing evidence of altered gait in prosthesis users, these parameters were selected because they are minimally affected by changes in speed, incorporate all speeds, or could be normalized to either speed or gait cycle. This limited the impact of differences in the self-selected speeds over multiple assessment sessions.18–21
For each session, the stride length–cadence relationship was calculated by plotting each stride length and cadence data pair across the three self-selected speeds and then deriving the coefficient of determination (R 2 ) of the regression line to evaluate the goodness of fit of the linear relationship. 18
Statistical analysis
The “non-overlap of all pairs” (NAP) method was used to assess differences between phases A and B (i.e. NMPK vs MPK). NAP is a non-parametric, statistical method that builds on earlier percent overlap analysis methods developed for single-subject studies and is considered a promising new approach to classic small-n analysis.11,22–24 NAP differs from previous percent overlap methods by making comparisons between each data point rather than comparisons based on summary data or selected points. In leveraging the entire data set, the calculation relates more closely to common effect size calculations providing stronger statistical support for the results than other single-subject analysis methods. 22
NAP determines the percent of data points from one phase that has larger values (ranks) than data points in adjacent phase. The final metric is the NAP percent, which is calculated in a few simple steps (Figure 1). First, each individual data point in the given phase (e.g. B, intervention) is compared to each data point in the adjacent phase (e.g. A, baseline). The score is assigned depending on whether the B point is higher (1), lower (0), or identical (0.5) to each A point (the score values can be reversed if the decrease in outcome is of interest). Next, scores for each B point are summed into a point non-overlap score and all point non-overlap scores are summed into the non-overlap total (see table in Figure 1). The non-overlap total is divided by the total number of comparisons to arrive at the NAP percent (typically reported as 50%–100%). Interpretation of the NAP percent is analogous to the area under the curve from a receiver operating characteristic curve. 22
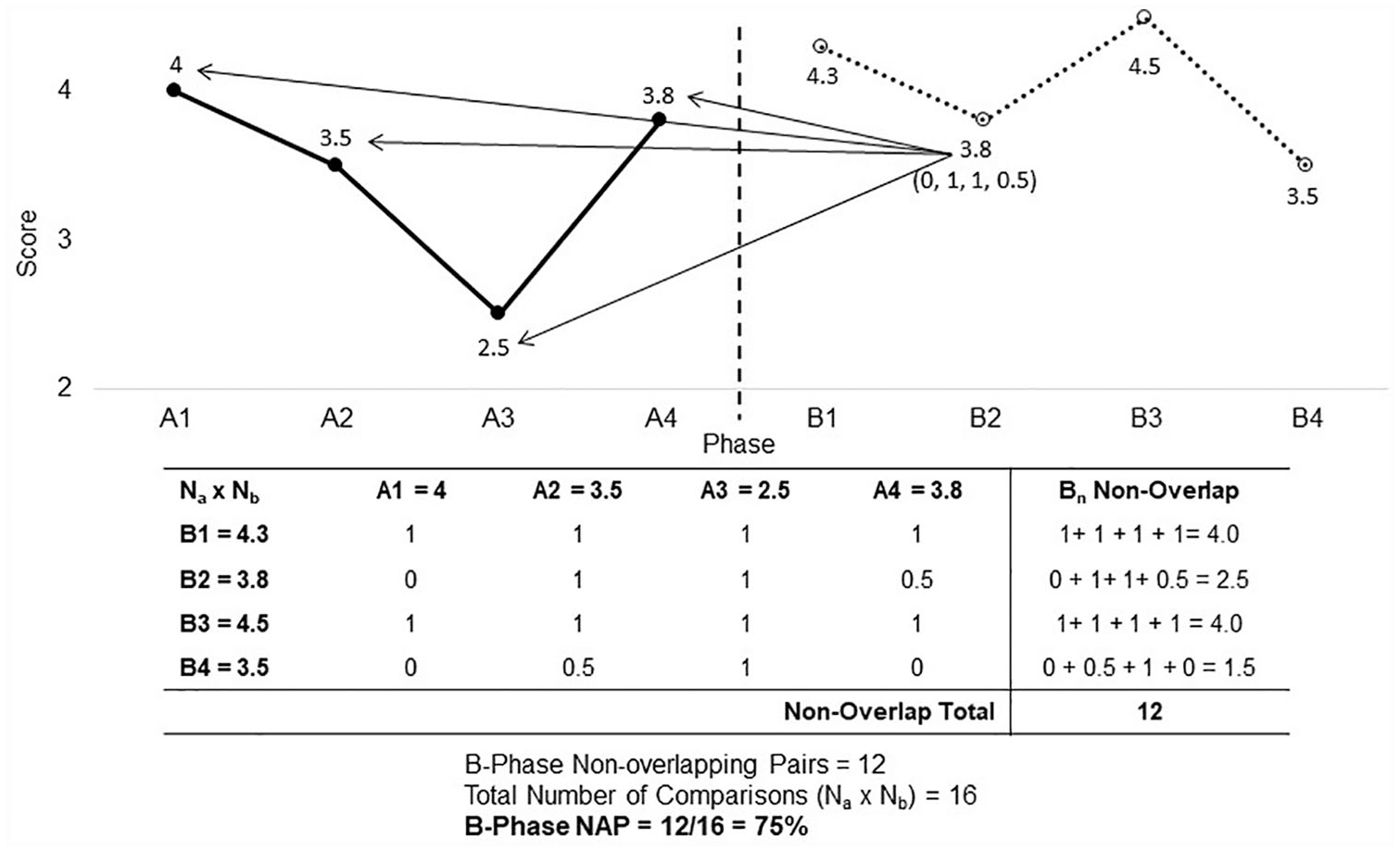
Non-overlap of all pairs (NAP) calculation. This illustration and table provide an example of the NAP calculation between two phases A (e.g. baseline) and B (e.g. intervention). First, a comparison is made between each point in the B-phase and each point in the A-phase by assigning a value of 1 if B higher than A, 0 if B smaller than A, and 0.5 if B equals A (see the table with crosstab of all A-B pairs and the illustration for graphic comparison of B2 point to all A points). In the next step, the non-overlap for each B-phase point is determined by summing values in each row. The non-overlap total is the sum of values in the last column (12 in this case). Dividing the non-overlap total (12) by the total number of pairs (16) results in the percent of non-overlap (75% here). A larger NAP percentage indicates in this case superior results in the B-phase over the A-phase, leading to the conclusion that intervention resulted in better outcomes in comparison to baseline.
The comparisons were made between all adjacent phases (e.g. B to A1 and A2) gait parameters (R2 of the stride length–cadence relationship across three speeds and, at each of three speeds, prosthetic early double-support percent, prosthetic single-support percent, and step width). In determining the comparison outcome, we rounded the stride length–cadence relationship to two decimal places and other parameters to whole integers before assigning the higher (1), lower (0), or tie (0.5) NAP score. In the BAB group, the baseline data point was treated as a standalone A-phase and compared to B1. In the ABA group, the baseline data point was added to A1 data (comprising five data points) because the subjects continued on their NMPK. Weighted NAP percent scores 23 were calculated to account for the repeated use of the middle phase in comparisons.
We designated the MPK as the intervention of interest and referenced all results with respect to the B-phase. Given the possibility of deteriorated performance on the MPK, we made the appropriate adjustment to extend the NAP range from 50% to 100% to from 0% to 100%. 22 Thus, the NAP percent larger than 50% indicates better performance with the MPK and the NAP percent smaller than 50% indicates worse performance with the MPK (better with the NMPK). Since the NAP percent also corresponds to Cohen’s d calculation, Cohen’s effect size was used for interpretation of results. On the 50%–100% scale, small, medium, and large effects from Cohen’s d (0.2, 0.5, 0.8, respectively) correspond to NAP values of 56%, 63%, and 70% (by analogy, 44%, 37%, and 30% were used as cut-offs in favor of the NMPK). 22 We considered NAP values of medium and large effects an indication of significant difference between the NMPK and MPK. Since the minimum acclimation time to the MPK is unknown, the secondary analysis in the BAB group explored whether the repeated exposure to the MPK affected the results. For this purpose, the data from the four BAB subjects were contrasted between phases B1 and B2 using the same NAP analysis.
Results
The studied sample included seven male subjects, six classified as K3, and one as K2 (Table 1). The individual gait speeds were previously reported. 25 Table 2 graphically summarizes the individual NAP results for 10 gait parameters with filled and open symbols representing overall significantly better performance with the MPK or NMPK, respectively.
MPK versus NMPK comparison for each subject and outcome using the NAP analysis.
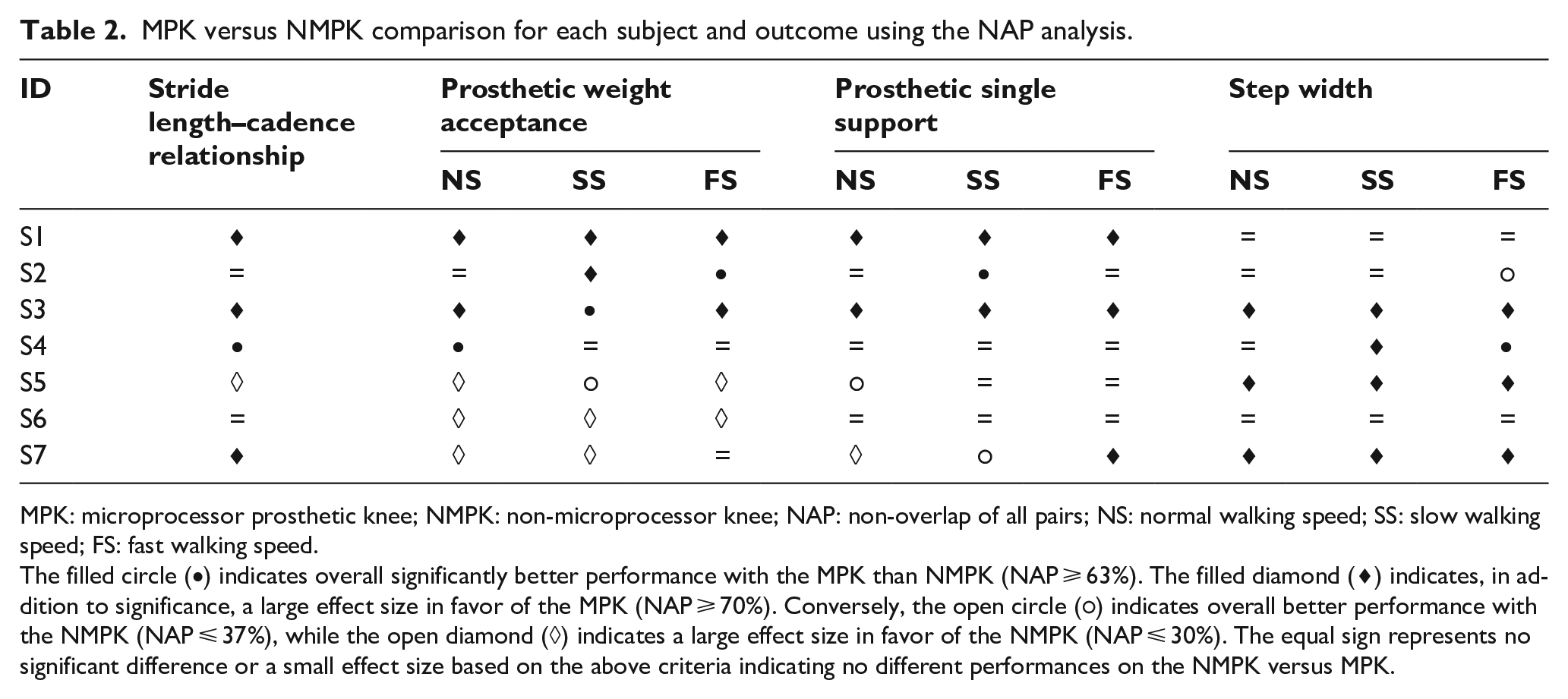
MPK: microprocessor prosthetic knee; NMPK: non-microprocessor knee; NAP: non-overlap of all pairs; NS: normal walking speed; SS: slow walking speed; FS: fast walking speed.
The filled circle (•) indicates overall significantly better performance with the MPK than NMPK (NAP ⩾ 63%). The filled diamond (
Two subjects (S1, S3) walked better overall during the MPK phases (improvement on 7 and 10 gait parameters, respectively). In three subjects (S2, S4, S6), most outcomes showed no difference between the MPK and NMPK phases. Only one subject (S5) had better outcomes in the NMPK phase (5/10 parameters). In terms of the group assignment, the outcomes were better during the MPK phase in the BAB group (S1–S4), whereas in the ABA group, the outcomes were either equivocal (S4, S6) or better in the NMPK phase (S5).
Stride length–cadence relationship
A significantly stronger linear relationship between stride length and cadence was found during the MPK phase in four of seven subjects (NAP 66%–92%; Figure 2) and during the NMPK phase in one subject (NAP 15%; Figure 2). The results were considered equivocal in the other two subjects because of the lack of significance (NAP 53%) or the small effect size (NAP 58%).
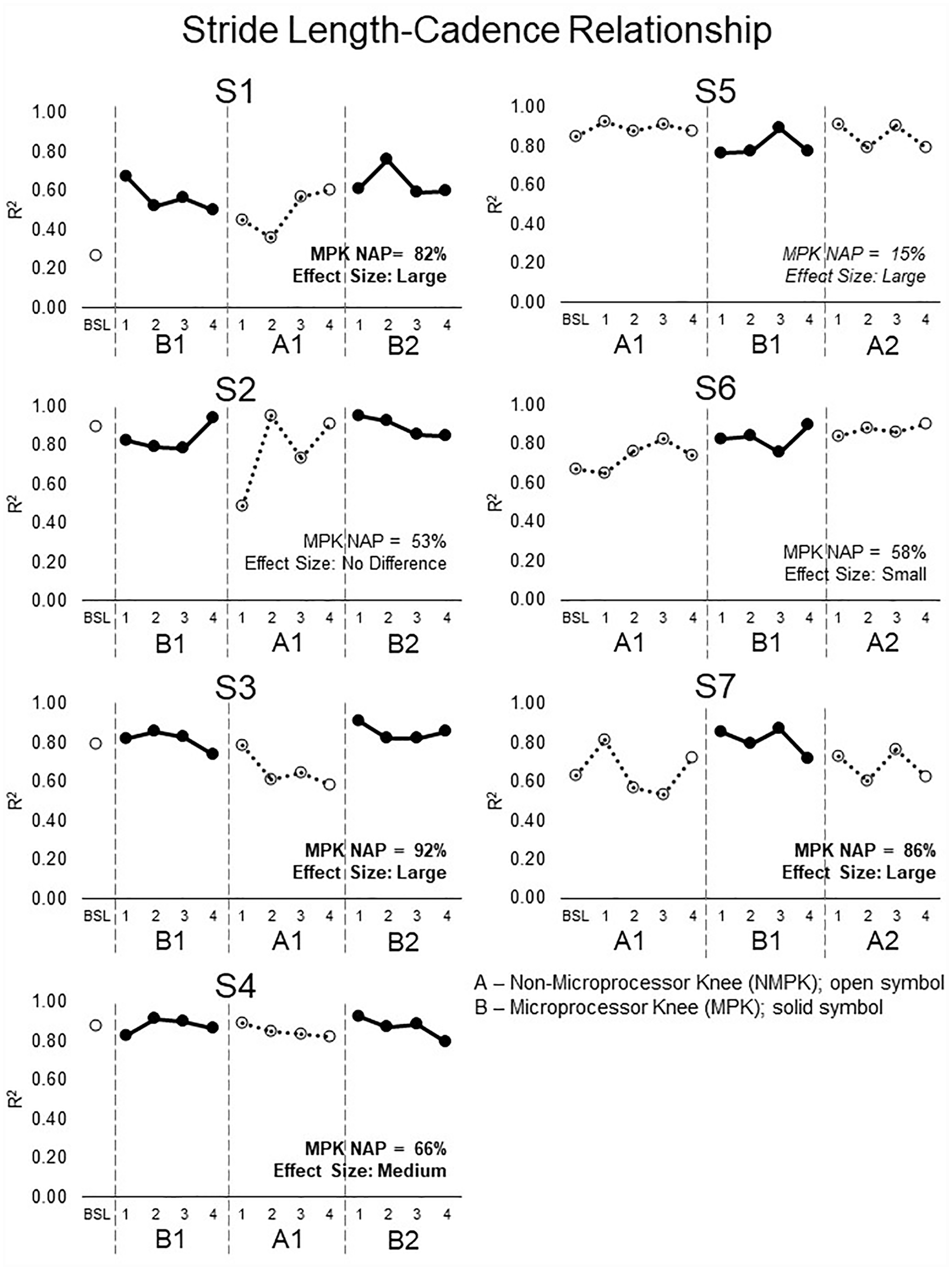
Stride length–cadence relationship across three speeds for each session. Higher R2 values indicate better performance. Four of seven subjects (S1, S3, S4, S7) showed higher NAP percent values with the MPK (bold), that is, a stronger (better) stride length–cadence relationship on the MPK (solid symbol) than the NMPK (open symbol). Subject S5 showed the better performance with the NMPK (italics), that is, stronger stride length–cadence relationship with the NMPK than the MPK. Subjects S2 and S6 showed either a small effect size or no difference between the knees.
Prosthetic limb weight acceptance
Four subjects (S1–S4) significantly decreased early double support on the prosthetic side for at least one speed during the MPK phase (Figure 3); S1 and S3 at all three speeds (NAP 64%–95%), S2 at the slow and fast speeds, and S4 at the normal speed only. Conversely, three subjects (S5–S7) significantly decreased the prosthetic early double-support during the NMPK phase (Figure 3); S6 at all three speeds (NAP 43%–10%), and S5 and S7 at two speeds. The BAB group showed better outcomes in the MPK phase and the ABA group in the NMPK phase.
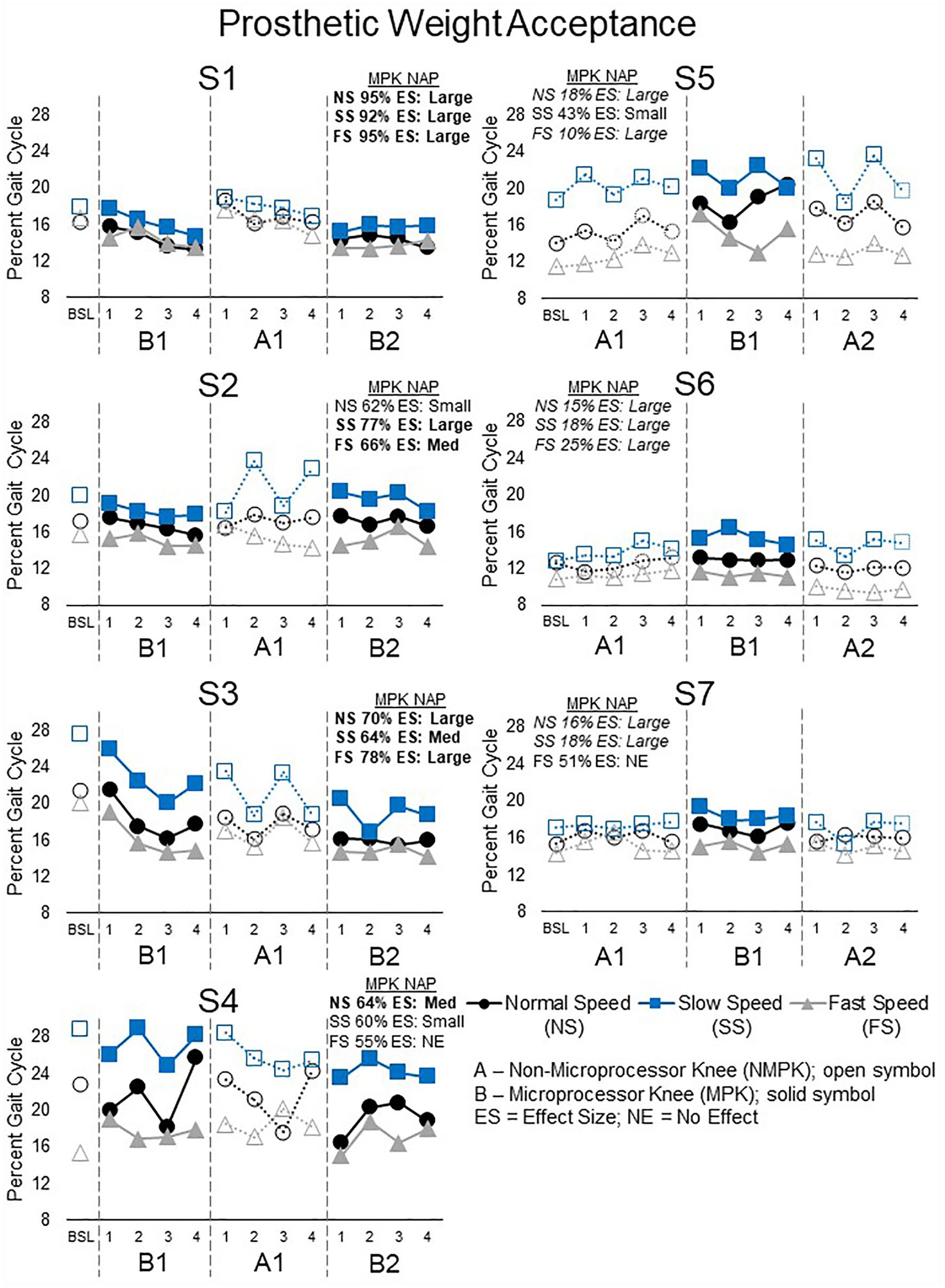
The percent of the gait cycle spent in prosthetic weight acceptance (double-limb support) for each session and speed (normal, black circles; slow, blue squares; fast, gray triangles). A reduction in the percent of the gait cycle spent in prosthetic weight acceptance indicates better performance. Four subjects (S1–S4) spent less time when transitioning to the prosthetic side with the MPK (solid symbol) than NMPK (open symbol), which had a medium-to-large effect size (bold) at all three speeds in subjects S1and S3. Three subjects (S5–S7) had quicker transitions to the prosthetic side with the NMPK. The NMPK had a medium-to-large effect size (italics) for all three speeds for subject S6.
Prosthetic limb single support
Three subjects increased the prosthetic single-limb support during the MPK phase for at least one speed (Figure 4): S1 and S3 at all three speeds (NAP 70%–100%) and S2 at the slow speed (NAP 64%). Conversely, one subject (S5) stayed longer in single-limb support in the NMPK phase at the normal speed (NAP 31%). Subject S7 showed mixed significant results that were better in the NMPK phase at the normal (NAP 26%) and slow speeds (NAP 34%) and in the MPK phase at the fast speed (NAP 85%). Two subjects had equivocal results (S4, S6).
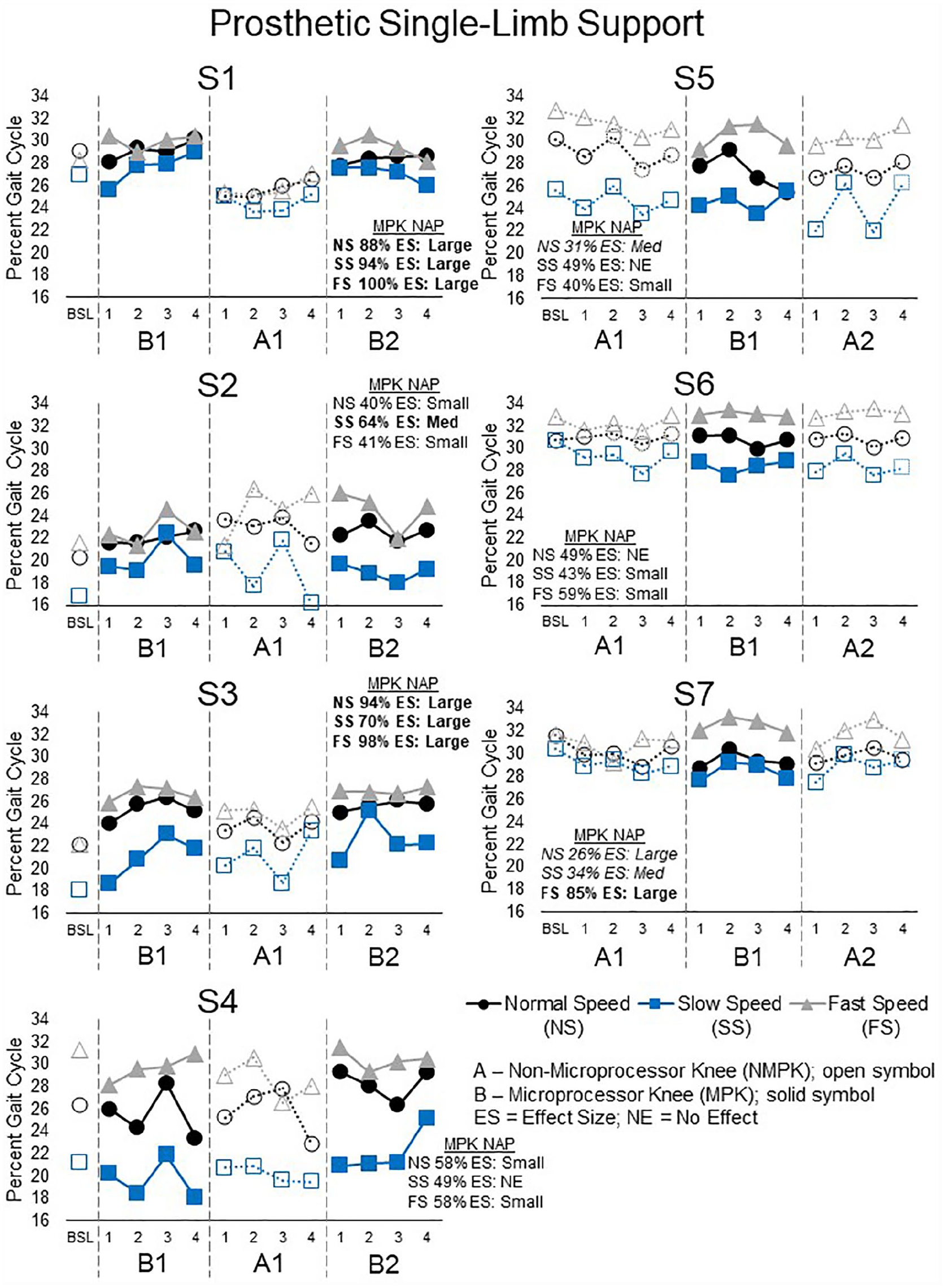
The percent of the gait cycle spent in single-limb support on the prosthetic side for each session and speed (normal, black circles; slow, blue squares; fast, gray triangles). Greater time spent in prosthetic single support indicates better performance. Three subjects (S1–S3) spent more time in prosthetic single support on the MPK (solid symbol) than NMPK (open symbol), which was has a large effect size (bold) for all three speeds in subjects S1 and S3. Conversely, 1 subject (S5) spent more time in the prosthetic single support on the NMPK than MPK at the normal speed (italics). Subject S7 showed better performance with the NMPK at normal and slow speeds (italics) but better performance with the MPK fast speed (bold). Subjects S4 and S6 had no difference between the knees at any speed.
Step width
Four subjects decreased step width during the MPK phase (Figure 5): S3, S5, and S7 across all three speeds (NAP 70%–100%) and one (S4) at the slow (NAP 74%) and fast speeds (NAP 66%). One subject (S2) had a smaller step width during the NMPK phase at the fast speed only (NAP 36%). The remaining two showed no significant difference between the two phases.
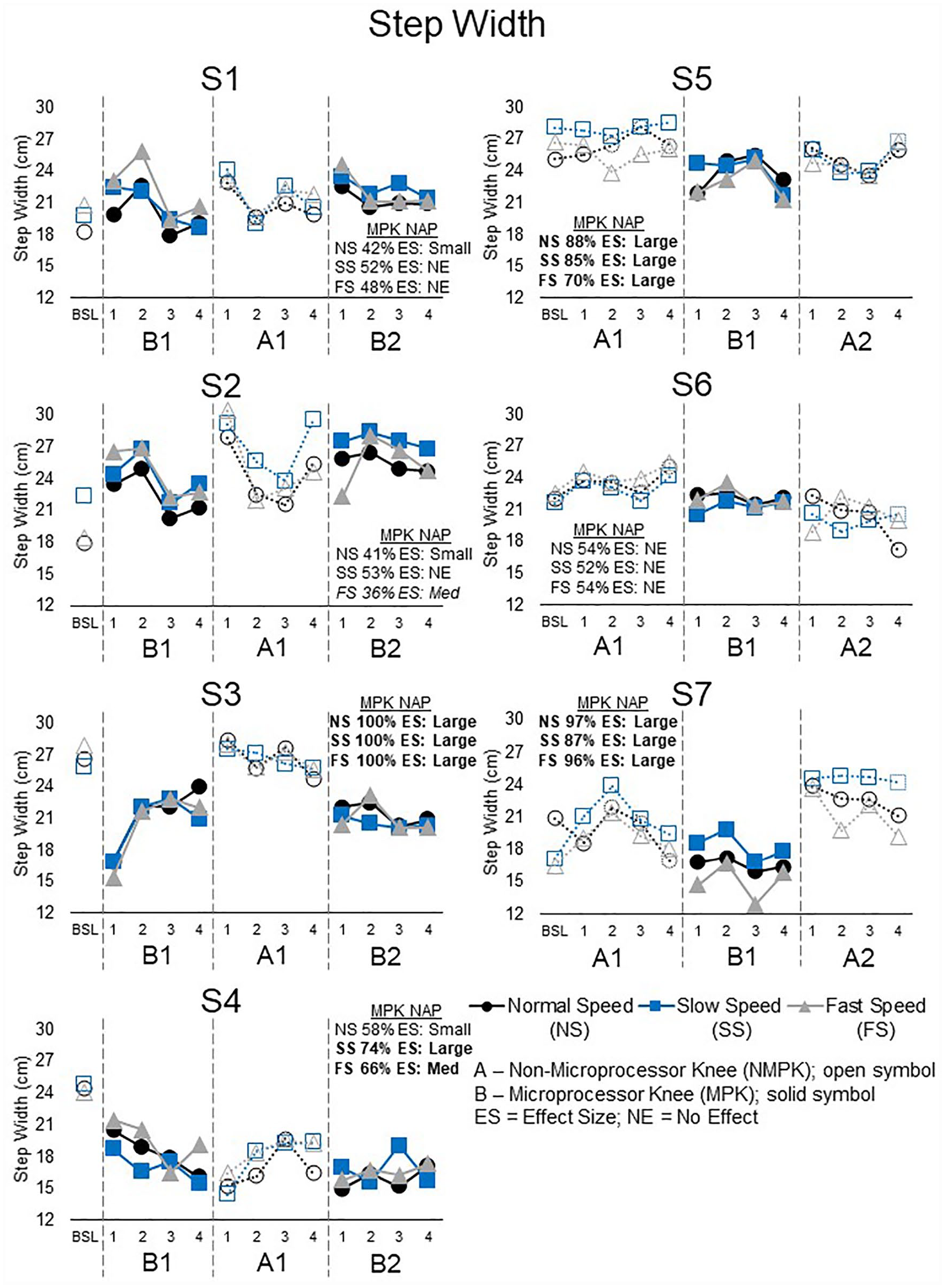
Step width for each session and speed (normal, black circles; slow, blue squares; fast, gray triangles). A smaller step width indicates better performance. Four subjects (S3, S4, S5, S7) had a smaller step width with the MPK (solid symbol) than NMPK (open symbol). The MPK had a large effect size (bold) for all three speeds in subjects S3, S5, and S7. Subject S2 had a smaller step width while walking with the NMPK at the fast speed (italics). Subjects S1 and S6 had no difference between the knees at any speed.
Duration of MPK exposure
The NAP values were more often in favor of the B2 than B1 phase. Two of four subjects improved more gait parameters in the B2 phase (7/10 and 9/10) than the B1 phase (0/10 for both). The other two showed slightly better results in the B1 than B2 phase (4/10 vs 3/10 and 5/10 vs 3/10, respectively). The stride length–cadence relationship, prosthetic weight acceptance, and prosthetic single-limb support more often improved during the second MPK phase.
Discussion
Our study demonstrated the practical application and the utility of the ABA/BAB single-subject method for evaluation of outcomes during the several weeks-long use of the MPK. This approach revealed that most subjects improved many temporal-spatial gait parameters while using the MPK in comparison with the NMPK. Improvements in gait coordination over the three walking speeds (stride length–cadence relationship) and step width at the slow and fast speeds occurred most frequently with the MPK. Aside from improvements with the MPK, no difference between the MPK and NMPK was most often seen. The results in favor of the NMPK were limited to the prosthetic weight acceptance and the ABA group. Collectively, this confirms our main hypothesis that the MPK would improve gait coordination and stability and also supports the single-subject design and data analysis used.
The single-subject design proved valuable for appreciating individual changes in gait when switching to the MPK. Exposure and withdrawal of the MPK and NMPK in two ways (ABA, BAB) and serial assessments provide confidence in the conclusions. The same approach revealed changes in mobility assessed by standard clinical measures in the same subjects. 25 These individual changes in gait and clinical mobility measures with the MPK would have been masked by evaluating outcomes with the group statistics.
The value of repeated evaluations in the single-subject design should not be overlooked. Some subjects showed comparably higher within-phase variability, which may have reflected well-known “good” and “bad” walking days in prosthesis users. This is unlikely due to relatively short acclimation to MPK since variability was greater in the NMPK than the MPK phase (e.g. S2 and S3 in Figure 2). The impact of variability can be controlled by serial evaluations and repeating of phases, as done here.
Moreover, the single-subject design allowed a closer look into possible reasons for different performance between the two knees. It appears that subjects S5 and S6 benefited the least from the MPK. Based on their characteristics (Table 1), they seem to share some common features. Both were long-time NMPK users with high AMP scores who did not use an assistive device. They also had similar prosthetic setups and reported very active lifestyles. This suggests they adjusted well to an NMPK, if not reached the peak, so it was hard to gain more from an MPK. In contrast, subjects who tended to improve the most with the MPK used an assistive device and the weight activated stance control type of NMPK. The most salient features of the strongest responder to the MPK here (S3) were comparably young age, recent amputation, and high AMP, suggesting a profile that is more likely to benefit from switching to an MPK and considered most suitable for inclusion in future group studies. Although the apparent profiles of the non-responders and responders may be intuitive to clinicians or implied by sub-group analysis in previous studies, the approach presented here shows how this can be derived empirically from bottom up and used for building future hypotheses.
The stride length–cadence relationship and step width improved most often in favor of the MPK. The observed increase in the stride length–cadence relationship over three speeds suggests improved gait coordination, presumably due to the ability of a user to benefit from the MPK when faced with the need to change speeds. In the absence of impairments, this relationship is near or above 0.9 (range 0–1.0).18,26 A stronger stride length–cadence relationship has been associated with lower fall risk and decreased sensory–motor demands in non-amputee populations.26–29 It also proved sensitive in distinguishing below-knee prosthesis users from controls. 18 Thus, this measure can be recommended in future studies of prosthetic gait.
Changes in step width were found more often with the MPK and, notably, at the slow and fast speeds. In conjunction with the improved stride length–cadence relationship, this further implies the superiority of MPKs over NMPKs at speeds other than normal. Since the above-knee prosthesis users walk with a wider base of support, 30 presumably to compensate for reduced lateral stability,31–33 the findings suggest that gait stability can be improved with the MPK.
Lower limb prosthesis users typically walk with less reliance on the prosthetic side34–37 and spend relatively more time in the early double-support prior to weight acceptance.38,39 The use of the MPK resulted in a shorter early double-support and longer single-limb stance on the prosthetic side, presumably because the controlled stiffening of the knee joint provided by the MPK increased stability throughout the stance. These results were more prominent in the BAB group and more apparent in the second MPK phase than the first MPK phase. Among the other potential factors that inadvertently turned out to be different between the two groups (use of assistive device, the NMPK type, other prosthetic componentry, Table 1), the most plausible explanation for better weight acceptance in the BAB than ABA subjects is the twice as long exposure to the MPK. Thus, acclimation time longer than 5 weeks seems necessary to observe a greater reliance on the prosthetic side when switching from the NMPK to MPK.
Study limitations
While NAP analysis is a useful statistical method for single-subject analysis, it does not account for the actual magnitude of difference between each phase due to its non-parametric (rank) nature. As such, even small numerical differences, if consistent, could result in a large effect size but potentially have little clinical relevance. However, consistently larger NAP values in favor of MPK suggest real changes in performance. Thus, while further work is needed to establish if the changes observed here are clinically meaningful, the overall results demonstrate how the single-subject method can distinguish differences between the compared conditions. To avoid confounding factors in the prosthetic set-up, some subjects were fit with the MPK with components not recommended by the manufacturer. While this may accurately reflect real-life situations in clinical practice, utilizing less ideal components, such as a solid ankle cushion heel (SACH) foot, may have limited the performance of the MPK. While subjects were randomly assigned to the ABA and BAB groups to account for potential learning effect and bias, we did not recruit long-term MPK users to examine the impact of switching to an NMPK and return to an MPK. Thus, it may be beneficial to examine in the future bi-directional exposure and reversal in both long-term NMPK and MPK users.
Conclusion
This study demonstrates that the single-subject method can objectively and reliably document changes in temporal-spatial gait characteristics while using an MPK in comparison with an NMPK. The results suggest improved gait coordination and stability with the MPK. Due to easy practical application in clinical settings, the single-subject method is recommended for prosthetic research and clinical practice.
Footnotes
Author contributions
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Wilson Research Foundation at Methodist Rehabilitation Center, Jackson, MS, USA, and Ossur ehf., Reykjavik, Iceland. Ossur ehf. had no role in the design, analysis, or decision to publish this study.
Trial registration
Evaluation of Transfemoral Amputees When Transitioning from a Mechanical to a Microprocessor Prosthetic Knee Registered with ClinicalTrials.gov NCT03829202.