
Abstract
Background:
Powered orthoses are a new generation of assistive devices for people with spinal cord injury, which are designed to induce motion to paralyzed lower limb joints using external power via electric motors or pneumatic or hydraulic actuators.
Objective:
Powered gait orthoses provide activated movement of lower limb joints to limit the forces applied through the upper limb joints and trunk muscles during ambulation due to the need to use an external walking aid, while simultaneously improving the kinetics and kinematics of walking in subjects with spinal cord injury. This article reviews their walking efficacy when used by people with paraplegia.
Study design:
Literature review.
Method:
A literature search was performed in ISI Web of Knowledge, PubMed, Google Scholar, ScienceDirect, and Scopus databases.
Results:
Efficacy was demonstrated in producing activated motion of lower limb joints. Powered gait orthoses have a beneficial effect on the kinetics, kinematics, and temporal–spatial parameters of gait, but their effect on muscle activity in individuals with spinal cord injury is still unclear.
Conclusions:
Further research is needed regarding the design and construction of powered gait orthoses using significant power application to the ankle joints and their effect on lower limb muscle activity and gait patterns in spinal cord injury subjects.
Clinical relevance
Powered orthoses is a new generation of orthotic intervention that could potentially be significant in assisting in improving the walking parameters and energy consumption of spinal cord injury subjects.
Background
Subjects with incomplete spinal cord injury (SCI) experience severe limitations in walking. 1 Rehabilitative gait training has been shown to decrease the risk of osteoporosis, improve cardiovascular health, and decrease urinary tract infections in patients with SCI. 2 Powered gait orthosis (PGO) may offer potential as an alternative intervention for SCI patients, by being used to retrain individuals to walk without the use of external assistance, such as the application of partial bodyweight offloading or use of a treadmill, which are used in other protocols (such as use of the Lokomat system). The advantages that the newly developed PGOs potentially offer are provision of a gait training system to enable SCI subjects to ambulate in different settings such as the clinical situation and also in the home and in the community via an external power supply using electric motors, pneumatic, and/or hydraulic actuators. 3 Many PGOs are not currently commercially available to the public and therefore would not be able to be used in the home. The aim is also to attempt to reduce the high energy expenditure experienced when walking with more conventional orthoses and to improve the efficacy of such devices by facilitating improved gait patterns compared to non-powered orthoses.
The development, design, and construction of powered orthoses started in the mid-1970s. 3 Vukobratovic et al. 3 developed one of the first powered orthoses by using pneumatic actuators at the hip, knee, and ankle joints, although walking with this powered orthosis was reported as being slow. Seireg and Grundmann 4 fabricated a powered orthosis using hydraulic actuators at the hip, knee, and ankle joints, and use of this orthosis by an SCI patient demonstrated its capability in providing walking and stepping actions. Both Belforte et al.5,6 and Kang et al. 7 developed powered orthoses with pneumatic actuators, which demonstrated a positive effect on walking by persons with paraplegia, and further developments were subsequently reported by Ruthenberg et al., 8 Ohta et al., 9 and Arazpour et al.10,11 In recent years, new designs of commercially available powered orthoses such as the exoskeleton lower extremity gait system (eLEGS) and the hybrid assistive limb (HAL) orthosis have been developed.
The following sections give an evaluation of the walking performance provided by PGOs and the evidence in the literature, in order to define their clinical efficacy.
Methods
A literature search was performed in ISI Web of Knowledge, PubMed, Google Scholar, ScienceDirect, and Scopus databases. Papers were selected from peer-reviewed journals, which demonstrated or reported temporal–spatial, kinematics, and kinetic effects or clinical efficacy by the use of relevant tests, such as the 6-min walk test, 10-m walk test, and self-efficacy measures, or by assessing physiological cost index (PCI) when SCI subjects used powered orthoses after being screened for relevance. Papers were excluded if the key words of the search were temporal–spatial, kinetics, kinematics, muscle activity, powered orthosis, exoskeleton, SCI patient, paraplegia, and paraplegic. Papers were excluded if testing involved any means of external support except the orthosis and a walking aid. To be included in the review, the research had to meet the following criteria:
The intervention involved a powered reciprocating gait orthosis (RGO), but without the use of partial bodyweight relief;
The subjects were all diagnosed with SCI;
The assessment of gait was undertaken using recognized tests.
Review findings
The isocentric reciprocating gait orthosis
Kang et al. 7 in a post-test design demonstrated improvements in walking speed, pelvic tilt, flexion and extension angles of the knee and hip joints, and in stance and swing phase times in three subjects with SCI after a period of approximately 3 months of gait training with a powered isocentric reciprocating gait orthosis (IRGO) using pneumatic actuators acting at the hip joints when compared to a mechanical IRGO. Walking speed was increased by 26%, and the percentage of swing phase during walking increased by 25% when walking with the PGO.
In a comparative study of SCI patients (n = 4) with injury levels T6–T12, when walking with a new PGO compared to an IRGO, Arazpour et al. 12 reported that after 6 weeks of orthotic gait training with the new PGO, patients had increased their gait speed by 33%, step length by 24%, cadence by 3%, and reduced lateral and vertical compensatory motions by 20% and 39%, respectively, when compared to walking with the IRGO.
Arazpour et al., 13 during a comparative evaluation of a PGO, IRGO, and a hip–knee–ankle–foot orthosis (HKAFO) on five SCI subjects (2 females and 3 males), reported that walking speed, the distance walked, plus the PCI all improved with both the new PGO and the IRGO as compared to the HKAFO (Table 1). In a further study, Arazpour et al. 10 evaluated the effect of a powered hip orthosis on walking by a SCI subject with a lesion level at T8, 51 months post injury. The kinematics and temporal–spatial parameters (walking speed, step length, cadence, and compensatory motions) were analyzed. Walking speed (29%), step length (7%), and cadence (18%) all increased in walking with the powered orthosis when compared to walking with a mechanical IRGO. Both lateral and vertical compensatory motions were again reduced (by 18% and 23%, respectively) with the new powered hip orthosis.
The effect of PGOs on gait parameters (studies investigating the effects of powered orthosis on parameters by SCI subjects).
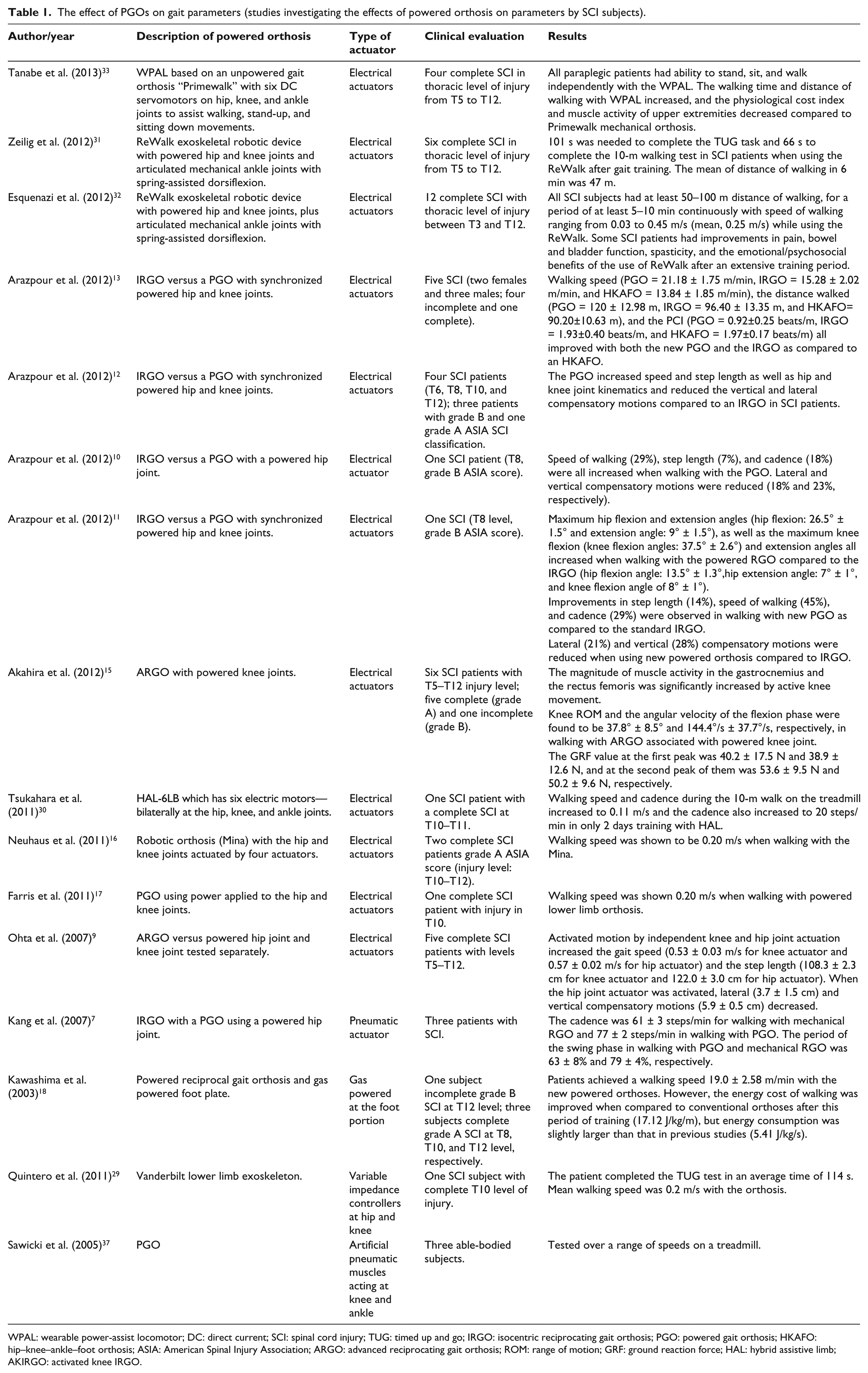
WPAL: wearable power-assist locomotor; DC: direct current; SCI: spinal cord injury; TUG: timed up and go; IRGO: isocentric reciprocating gait orthosis; PGO: powered gait orthosis; HKAFO: hip–knee–ankle–foot orthosis; ASIA: American Spinal Injury Association; ARGO: advanced reciprocating gait orthosis; ROM: range of motion; GRF: ground reaction force; HAL: hybrid assistive limb; AKIRGO: activated knee IRGO.
Arazpour and colleagues also demonstrated the design and simulation of a PGO with synchronized movement between the knee and hip joints 14 and evaluated its effect against separate isolated movement of either the hip or knee joint actuators when used by a SCI subject with an injury level of T8. 11 Maximum hip flexion and extension angles and the maximum knee flexion all increased by 96%, 28%, and 368%, respectively, and extension angles all increased when walking with the PGO compared to the IRGO. Improvements in step length (14%), speed of walking (45%), and cadence (29%) were also observed in walking with the new PGO as compared to the standard IRGO. In addition, both lateral (21%) and vertical (28%) compensatory motions were reduced.
The advanced reciprocating gait orthosis
Ohta et al. 9 in a study of SCI subjects (n = 5) with complete lesions at levels T5–T12 compared the effects of walking with a powered advanced reciprocating gait orthosis (ARGO), in which both the hip and knee joints were activated separately, to those demonstrated by a standard ARGO. Activated motion by the knee and hip joint actuators separately increased both the gait speed (23% for knee actuator and a maximum of 9% for the hip actuator) and the step length (7% for knee actuator and a maximum of 5% for the hip actuator). When the hip joint actuator was activated in isolation, lateral (maximum 18%) and vertical compensatory motions (maximum 25%) were decreased.
Akahira et al. 15 also evaluated an ARGO (but this time with powered knee joints only) and compared the resultant gait parameters attained to those of a standard non-powered ARGO on six SCI patients, five with a complete lesion and one with an incomplete lesion. They reported that the magnitude of muscle activity in the gastrocnemius and the rectus femoris muscles was significantly increased by active knee movement. No significant difference was noted between the two peaks of the ground reaction force (GRF) between two orthoses. Knee range of motion (ROM) and the angular velocity of the flexion phase were found to be 37.8°/s ± 8.5°/s and 144.4°/s ± 37.7°/s, respectively, when walking with the ARGO with powered knee joints. There were no significant differences between the two orthoses in hip and ankle ROMs. The angular velocity of the hip joint in walking was greater in the powered orthosis.
In a study on SCI subjects (n = 2; complete American Spinal Injury Association (ASIA) classification-A), Neuhaus et al. 16 evaluated the Mina, a robotic orthosis for assisting mobility in persons with paraplegia, by measuring walking speed when using actuation to power the hip and knee joints only. The walking speed measured was low at 0.2 m/s.
Farris et al. 17 in using a PGO with electrically actuated hip and knee joints demonstrated that again the walking speed attainable was 0.2 m/s by one SCI patient with a complete lesion level at T10. The authors only evaluated the feasibility of this new orthosis in assisting a single SCI subject, but did show that both the hip and knee trajectories had a high degree of step-to-step repeatability during ambulation.
The weight-bearing control orthosis
In a study of persons with paraplegia (n = 4) with traumatic spinal cord injuries between T8 and T12, Kawashima et al. 18 demonstrated that after 3 months of orthotic gait training with a weight-bearing control orthosis (WBCO), which used a powered foot plate, they achieved a walking speed of 19.0 ± 2.58 m/min with the new powered orthoses. The energy consumption was improved when compared to conventional orthoses after this period of training (17.12 J/kg/s) but was still larger than that in previous orthoses (5.41 J/kg/s).14,19–25
The variable constraint hip mechanism
Audu et al. 26 evaluated a newly developed RGO with a variable constraint hip mechanism (VCHM), in terms of walking speed, step length, hip knee ankle joints moment, and ROMs on six able-bodied subjects. They demonstrated a 25% decrease in mean speed of walking with the powered hip orthosis as compared to normal walking. Magnitudes of the muscle activity of tibialis anterior, quadriceps, and hamstrings were higher with the new orthosis as compared to a mechanical IRGO and normal walking.
The HAL orthosis
Powered lower limb orthoses such as the HAL-5 Type-C, which has five electric motors, the ReWalk-powered orthosis (Argo Medical Technologies), the wearable power-assist locomotor (WPAL), and the eLEGS powered orthosis (Berkeley Bionics) are all examples of commercially developed powered orthoses designed for walking by persons with paraplegia.
Some authors have described development of new powered devices. Suzuki et al. 27 proposed an algorithm to develop the HAL-5 Type-C device to potentially support a patient with paraplegia to walk. More recently, Uchiyama et al. 28 described the development of an orthosis with five actuators using a simulation technique. Quintero et al. 29 described the development of a PGO that consisted of controllers bilaterally at the hip and knee with ankle supports, which when tested by a person with paraplegia with a complete injury at T10 level produced a mean walking speed of 0.2 m/s. Tsukahara et al. 30 evaluated the effect of gait training with the HAL-6LB device (which was developed to support the whole weight of complete SCI patients) by a single SCI subject with a complete T10–T11 level of injury for 8 days, for 2 h/day. They reported that walking speed and cadence during treadmill walking were 0.11 m/s and 20 steps/min, respectively.
The ReWalk orthosis
Zeilig et al. evaluated the effect of the ReWalk exoskeleton (which contains independently controlled bilateral hip and knee joint motors and extension-assist orthotic ankle joints) on safety and tolerance in six subjects with complete SCI and demonstrated that using the ReWalk was well tolerated and safe with no significant increase in pain and fatigue after training in individuals with SCI. The mean time to complete a 10-m walk test for those participants with lower lesions (T9–T12) following training when using the device was 47 s. 31 Esquenazi et al. also analyzed the effect of ReWalk-powered exoskeleton on ambulatory function in 12 subjects with SCI. All SCI patients could walk without human support for 50–100 m for between 5 and 10 min continually. The mean walking speed with this powered exoskeleton was 0.25 m/s. 32
The WPAL orthosis
Tanabe et al. analyzed the effect of the WPAL on walking, PCI, and muscle activity of the upper extremities in four people with paraplegia. They demonstrated that all subjects walked independently with the new powered device. The walking duration and distance of walking with the WPAL increased seven-fold compared to that achieved using the Primewalk orthosis, and the PCI and muscle activity of upper limbs were both reduced. 33
Discussion
Previous review papers, such as those published by Ferris et al., 34 Dollar and Herr, 35 and Bogue, 36 have analyzed in general terms the advances in PGO design for gait rehabilitation and ambulation. Ferris et al. evaluated a newly developed powered lower limb orthosis for assisting treadmill stepping in disabled individuals, using a bodyweight-supported treadmill system for gait rehabilitation in a clinical environment. The ability to start, turn, stop, and avoid obstacles during overground walking was reported as the main advantages of using PGOs in gait rehabilitation following neurological injury. 34 In a separate review paper, Dollar and Herr 35 noted the history of “active” lower limb orthoses. They described an overview of the design of hardware, actuation, sensory, and control systems for most of the powered orthosis that have been fabricated up to 2007. Within this particular literature set, the authors considered powered orthoses to include lower limb exoskeletons, modular active orthoses, single joint active orthoses, and other orthotic devices. They concluded that the research directions in the future would need to focus more on the development of lightweight exoskeletons and active orthotic devices. 35 In another review, Robert Bogue explored and reviewed recent developments in exoskeletons and robotic prosthetics within the fields of military, civil, and medical applications. He also noted the role of brain–computer interface technology and the use of robotic prosthetics. 36 However, this article analyses the effect of PGOs as evidenced in the literature on specific gait parameters such as kinetics, kinematics, muscle activity, walking speed, and other gait parameters such as energy consumption. These are important parameters because the main drawbacks of non-powered orthoses include the high energy expenditure experienced by SCI subjects and the low walking speed which may be attained.
Lower limb kinetics and kinematics
Various studies have reported on the kinetics and kinematics of walking by SCI subjects while using a PGO.7,9–11,15–17 Some authors have chosen to use able-bodied subjects in their study design.5,6,26 Recent studies have reported that powered orthoses with pneumatic, motorized, or hydraulic actuators have surprisingly little effect on the kinetics and kinematics of walking in subjects with SCI. The most predominant improvements have been noted in hip and knee joint sagittal plane ROMs via actuation (either separately or when synchronized), which more closely resemble walking patterns demonstrated by able-bodied people. Design and simulation of new powered orthoses with active ankle joints are needed to further develop the design of such orthoses.
Effect on lower limb muscle activity
Studies have demonstrated that the amplitude of muscle activation around the ankle joint does not alter when walking with either a mechanical or powered ankle–foot orthosis (AFO). When using a powered AFO when either a therapist or the subject has controlled the actuation in those SCI subjects with incomplete lesions, there was again no significant difference noted, except that the amplitude of tibialis anterior was 31% lower in walking with the therapist control condition. 37 Audu et al. 26 evaluated the effect of an RGO with a VCHM on the muscle activity of three lower limb muscles in able-bodied subjects.
One study has evaluated the effects of a mechanical orthosis (ARGO) on muscle activity of the lower limb. 38 Very-low-amplitude muscle activity was demonstrated in the early stages of orthotic gait training. Their analysis proposed that the provided modulation in the soleus (SOL) activity could be contributing to the alteration in the pattern of the orthotic gait pattern. They concluded that gait training with an orthosis could provide “locomotor-like” activity of paralyzed lower limb muscle in subjects with SCI. In another study, Kawashima et al. 39 in 2008 evaluated the effect of gait training in electromyographic (EMG) activation of the SOL and biceps femoris muscles. They reported that the locomotor-like muscle activity in gait training with an orthosis is not a response of reflex, but caused by the central pattern generator (CPG) activation and its interaction with afferent inputs. They concluded that gait training with an orthosis can have the benefit of simulating the spinal locomotor center in patients with SCI. Tanabe et al. 33 when evaluating the effect of the powered WPAL orthosis on muscle activity of the upper extremity in four people with paraplegia reported that they all had less muscle activity in the upper limbs compared to walking with the unpowered Primewalk orthosis, indicating that powered orthoses may reduce such loading.
Although Dietz et al. 40 demonstrated that knee movement did not have an important role in providing locomotor-like EMG activity in SCI patients, Akahira et al., 15 while assessing gait with an ARGO adapted with a powered knee joint, showed that patients had remarkably increased muscle activity of the gastrocnemius muscle at the end of swing phase (for knee extension phase) and the rectus femoris muscle during mid-to-late swing phase. There is, therefore, variance in the literature.
Effect on walking speed and other gait parameters
The effect of PGOs on walking speed, cadence, and step length exhibited by SCI subjects is dependant on which joints are actuated in an orthosis (e.g. the hip or knee actuated separately or by being synchronized). Few studies have directly compared these parameters between separately or synchronized movement of the hip and knee joint conditions during walking with PGOs. One study demonstrated improvement in walking speed and step length when walking with synchronized and actuated motion at the hip and knee joints compared to separate activation of the joint actuators. 11 However, studies found improvement in temporal parameters following the addition of external power using different combinations.9–11,16–18 However, the evidence to date suggests that powered orthoses have the capability to improve specific gait parameters whencompared to non-powered mechanical orthoses such as the IRGO,7,10,12,13 a conventional HKAFO, 19 and the ARGO.9,15 Nevertheless, there is no clear evidence as to which combination of power application is the most effective in powered devices. In addition, devices which have powered ankle joints are yet to be tested, and these need to be compared to equivalent devices without powered ankle joints to confirm any positive effect that these may have.
Effect on energy consumption
Evidence has shown that SCI subjects habitually abandon use of their mechanical orthoses, with abandonment rates of 61%–90% for children with myelomeningocele 41 and 46%–54% in adults with SCI42–46 due to the high level of energy expenditure needed to ambulate. One of main reasons for the development of PGOs was to potentially reduce energy consumption when walking with an orthosis. 47 Three papers have analyzed the effect of this type of orthosis on energy consumption during walking in SCI patients.13,18 The energy consumption of walking has been quoted as being 0.176 mL/kg/m for healthy persons. 41 When walking with the WBCO, this figure was 5.41 J/kg/s 18 although these cannot be directly compared. The difference between able-bodied subjects and walking with a powered orthosis is substantial, but is still improved when compared to that noted when people with paraplegia walk with mechanical orthoses. Arazpour et al. 13 demonstrated that a PGO can improve walking speed and the distance walked and reduce the PCI of walking as compared to mechanical orthoses, probably due to the activated movements of the lower limb joints. Tanabe et al. 33 when comparing the WPAL and Primewalk orthoses demonstrated that the PCI exhibited by four people with paraplegia was reduced when using the WPAL. One other paper reported that the effort of walking was decreased when using a powered motorized ARGO in SCI patients. 9 The literature on energy cost of walking with powered orthoses is therefore limited. A further understanding of the energy cost of powered orthosis ambulation is therefore required for patients with SCI. PGOs should incorporate active ankle joints, because these have the potential to not only aid propulsion, but also help to lift the center of gravity of the body upward and potentially reduce energy consumption during ambulation, as well as providing clearance during swing phase of gait.
Walking speed
Walking speed has varied between orthoses, but still remains significantly low compared to that exhibited by able-bodied subjects. This parameter is thought to be adversely affected by the need to maintain balance and the need in some devices for people with SCI to continually activate the powered orthotic joints themselves during ambulation when previously designed mechanical orthoses, such as those with reciprocal links, are adapted with powered orthotic joints. Commercially developed powered orthoses (exoskeletons), which have been designed for walking by people with paraplegia, without them having to be continually activated by the wearer, have demonstrated the potential to significantly improve this parameter.
Conclusion
In summary, PGOs provide assistance during ambulation by provision of external force via actuators to provide active motion in specific joints of the lower limbs. They are also a helpful clinical assistive device in regeneration of stepping and gait training in SCI patients. However, this positive effect has only been reported by the WBCO on muscle activity in people with paraplegia, and more research is required to confirm any beneficial effect.
There is some evidence of an increase in step length and increase in cadence when walking with powered orthoses. More research is required in terms of the effect on kinetics, kinematics, and spatial and temporal parameters of gait following the addition of external power to a mechanical orthosis and in particularly how to improve walking speed when using these devices. Evaluation of how powered orthoses can change muscle activity stimulation in the lower limbs and a specific method of gait training sessions with this type of orthosis is needed in further studies. Powered orthosis has the potential to decrease energy consumption, and further work is required to analyze this effect, for example, in an attempt to decrease upper limb demand in people with paraplegia. This is therefore a new generation of orthotic intervention that could potentially be significant in assisting in improving the walking parameters of SCI subjects.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.