
Abstract
Background: The aim of this case study was to identify the effect of a powered hip orthosis on the kinematics and temporal-spatial parameters of walking by a patient with spinal cord injury (SCI).
Case Description and Methods: Two orthoses were evaluated while worn by an incomplete SCI subject with a T-8level of injury. Gait evaluation was performed when walking with an Isocentric Reciprocating Gait Orthosis (IRGO) and compared to that demonstrated by a newly powered version of the orthosis; based on the IRGO superstructure but incorporating powered hip joints using an electrically motorized actuator that produced active hip joint extension and flexion.
Findings and Outcomes: The powered hip orthosis, when compared to the IRGO, increased the speed of walking, the step length and also the cadence demonstrated by this subject. Vertical and horizontal compensatory motions with new orthosis decreased. Hip angles when walking with this orthosis were comparative to those demonstrated by normal walking patterns.
Conclusions: The hip actuator produced positive effects on the kinematics and temporal-spatial parameters of gait during level-ground walking trials, resulting in an alternative approach to walking by SCI patients.
This orthosis has the potential to improve hip joint kinematics, the temporal-spatial parameters of gait in SCI patients walking.
Background
The development of powered orthoses has produced a new generation of orthoses which could potentially overcome some of the limitations of those currently available. 1 Mechanical devices, such as reciprocating gait orthoses (RGOs), incorporate reciprocating mechanisms (albeit passive), which can allow a functional range of motion in the hip joints if the anatomical joint range is present. This does not represent a mechanical restriction. However, the application of power to the hip joints offers the opportunity to tailor the range of motion (ROM) provision at the hip during locomotion by programming the actuators to provide a bespoke prescription for each individual patient depending on the results of their preliminary assessment. The main purpose of current devices is to compensate for the biomechanical functions that have been lost. 2 Development of powered orthoses could allow patients, such as those with spinal cord injury (SCI), to walk in a controlled clinical environment and so is useful in playing a facilitative role to improve motor function in rehabilitation. 3 In addition, a powered orthosis would have implications out with the clinical environment for SCI subjects by allowing them to achieving a more functional gait, as well as having the potential to have implications out with the clinical environment by achieving a more functional gait. The ultimate goal of rehabilitation in these patients is to increase motor functional performance for those patients who are unable to walk without an orthosis. For this to succeed, lower extremity orthoses should have the facility to provide adequate amounts of power to facilitate ambulation; be it via direct muscle activation using functional electrical stimulation, or alternatively, based on the use of externally-applied forces.
The initial designs of powered orthoses utilized exoskeletons. 4 However, RGOs have since formed the basic structure upon which most powered orthoses are designed today.3,5-7 The externally-applied force has previously been installed on the mechanical structure or exoskeleton using pneumatic, motorized, electric or hydraulic actuators. The high efficiency, smoothness and fast response of motor-activating actuators makes them more suitable for the application of power to RGO-type devices than other forms of force application. 8
Powered orthoses have been developed for walking by SCI patients since 1960. Ruthenberg et al. built an orthosis with two degrees of freedom of movement. 9 They developed a lightweight orthoses (approximately 10 kg) which resulted in an improved gait pattern which instigated further development in this area. Ohta and colleagues also developed an orthosis, but it was not suitable for activities of daily living (ADL) situations experienced by spinal injury patients because of its large bulk. In addition, the motor used to pull the pelvic cable required unacceptably high force expenditure.
The Sogang University- powered orthosis consists of a combination of a lower limb orthosis and a specially designed walker which houses the battery and electronic components. Although the weight of the orthosis may be decreased with this design, a disadvantage is the need for the patient to walk at a fixed distance from the walker. Also, access to a narrow environment is not possible with this design. 10
To resolve the disadvantages presented by previous devices, we proposed the design and construction of a prototype motorized orthoses that included a single actuator positioned in the posterior aspect of the pelvic section of an isocentric reciprocating gait orthosis (IRGO) to drive and control sagittal plane hip rotation. To provide a reciprocal pattern of movement for the hip joint, the actuator was connected to the reciprocal link of the IRGO. The hypothesis of this study was that the provision of motorized hip joint movement via external force to the orthosis would improve the speed of walking, step length and reduce compensatory vertical and horizontal motions at the pelvis level demonstrated by the patient during ambulation. The purpose of this study was therefore to evaluate the effect of a new motorized hip orthoses, on specific gait parameters when worn by a single paraplegic patient.
Case Description and Methods
Subject and experimental protocol
A single SCI subject (female age 22 years, weight 54 kg and height 165 cm, with a lesion level of T8 and 51-months post-injury) participated in this study. The inclusion criteria to assign a volunteer patient to this study were existence of a thoracic level SCI of at least six-month post-injury duration (for neurological and emotional stability), a capability to achieve a full range of motion in the hips, knees and ankle joints, and the ability to use a walking frame or elbow crutches for walking with an IRGO. The existence of cardiovascular or pulmonary disease, contractures, severe spasticity or obesity, were exclusion criteria for this study. The subject had previously learned to use a mechanical IRGO for three months prior to this study while using a walking frame with the wheels anteriorly positioned, and the subject also had an additional three-month period of familiarity in walking with the powered orthosis prior to the walking trials using the same method.
A Vicon digital motion capture system with a frequency of 100 HZ (Oxford Metrics, UK) was used for capturing the locations of reflective markers that were placed on the orthosis and trunk. Fifteen markers were used in the lower extremity and four markers were placed on the trunk. Markers were placed bilaterally over the position of the greater trochanter, lateral condyle of the femur, head and lateral malleolus of the fibula, the second metatarsal, ASIS, calcaneus, and over the jugular notch, spinous process of the seventh cervical vertebrae and the acromio clavicular joints. Lower extremity markers were placed on the uprights as close as possible to the considered points.
Walking experiments were performed in the Biomechanics Laboratory of Ergonomic department of University of Social Welfare and Rehabilitation Science. The subject volunteered for the study and was allowed to exclude herself at any time. Before participation in the study, the subject read and approved a statement acknowledging informed consent. The Ethics Committee of University of Social Welfare and Rehabilitation Science approved the performance of this study.
Orthosis considerations
The IRGO formed the main structure of the new orthosis. Due to the relatively low friction in the hip connection link in IRGOs, they have a potentially effective role in reducing energy consumption in users compared to other RGOs currently available. Patients have an acceptable posture with this type of orthosis and its structure is simple, lightweight and is suitable for use by SCI patients.11-12
The powered orthosis was designed with the intention to provide an exoskeleton capable of producing walking patterns closer to that of healthy subjects than currently available in RGO designs. This new orthosis was designed to be portable and easy to don and doff as well as to wear by the patient during ambulation.
Due to the suitability of electrically powered actuators, which have the potential advantage of offering suitably rapid feedback and control linked to convenient routine maintenance programs, it was decided to use this type of actuator in the orthosis. The mechanical orthosis was manufactured for the volunteer subject by utilizing casts of the lower extremity, lumbar and pelvic areas. The total weight of IRGO was 5.6 kg, while total weight of powered hip orthosis with batteries, sensors, cabling and electronics was 8.4 kg. Gait parameter data were calculated under two test conditions; walking with mechanical IRGO and walking with new powered orthosis (Figure 1). Prior to data capturing, the subject performed practice walks along a straight 6-m long walkway while wearing the powered hip orthosis. The subject ambulated with a walking frame in this study. She walked along the walk way five times. The subject walked with both the knee and ankle joints locked within the orthosis for both test conditions. The means of the resulting data were calculated from both left and right sides for the five walks using each device.

Posterior and lateral views of the new powered hip orthosis used in this study showing the position and mounting arrangement of the actuator.
The electronics and motor included a Maxon Motor EC30 (Maxon, Switzerland) (Figure 2) with a planetary gearbox with reduction of 156, encoders, motor drivers, power and a programmable controller. The motor sequencing was based on models optimized by software specifically designed and built for this purpose. The orthotic joint motion patterns could then be programmed into the microcontroller to the main system. According to this approach, actuators were capable of generating appropriate movement patterns at specified intervals during the complete gait cycle (Figure 3).

Actuator positioning in new orthosis.
Patterns of generating movement by hip actuators during the gait cycle.
One rechargeable 24 V (Lipo Battery, Thunder Power RC G6 Pro Lite 25C 5400mAh 6-Cell/6S) was used in this orthosis (Figure 4). This rechargeable battery was capable of providing two hours of continuous walking with the powered orthosis when initially fully charged. The batteries and control board were placed within the backpack which was worn by the subject with the orthosis donned. The operation of the new powered hip orthosis during walking was instigated using a switch. This switch was put on the handle of the walker, and was pushed by the patient when she unloaded the desired leg. The patient unweighted the desired leg by transferring weight to the walker and contralateral leg. The hip actuating motor was activated by pressing a switch on the handle of the walker which produced hip flexion on the same side. The opposite lower limb was also provided with a hip extension assist via the reciprocal link. Power was added to primarily flex the hip joint to give a powered swing phase.

Battery used in new orthosis.
Findings and Outcomes
During level-ground walking, both the volunteer SCI subject and the orthotist who fitted the device were satisfied with the function of the powered orthosis. The SCI subject had previously trained for three months with the standard mechanical orthosis to ensure that she could more easily adapt to, and feel comfortable with, the powered hip orthosis during the period of rehabilitation and the walking trials themselves.
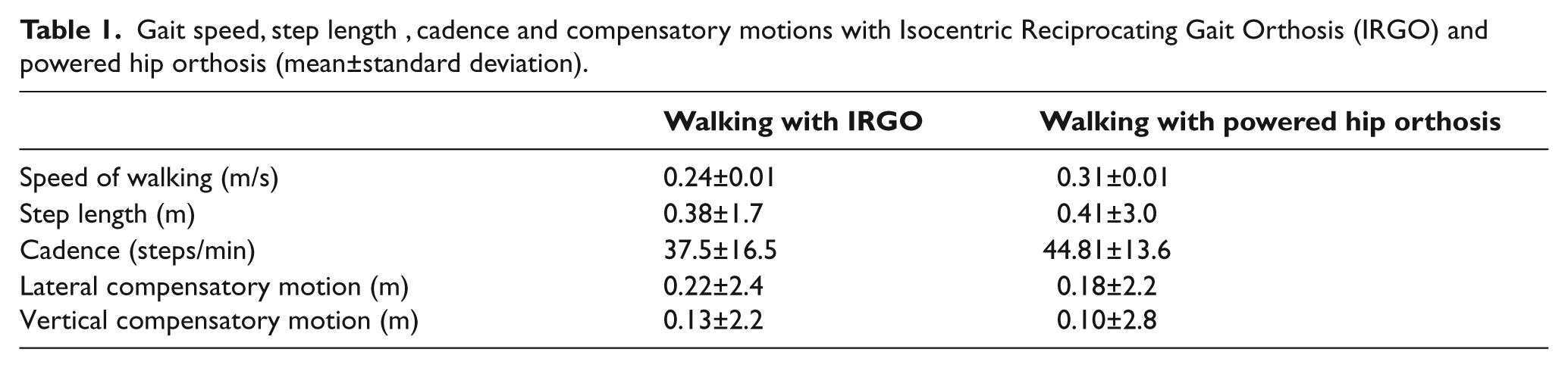
The new orthosis performed robustly throughout the experimental evaluation. Table 1 shows the speed of walking and step length of the subject in the two experimental situations. The powered hip orthosis increased all relevant parameters (speed of walking and step length) in this subject. Vertical and horizontal compensatory motions with hip powered orthosis decreased (Figure 5).These compensatory motions were evaluated from the trajectory of the marker placed on the ASIS.
Gait speed, step length, cadence and compensatory motions with Isocentric Reciprocating Gait Orthosis (IRGO) and powered hip orthosis (mean±standard deviation).
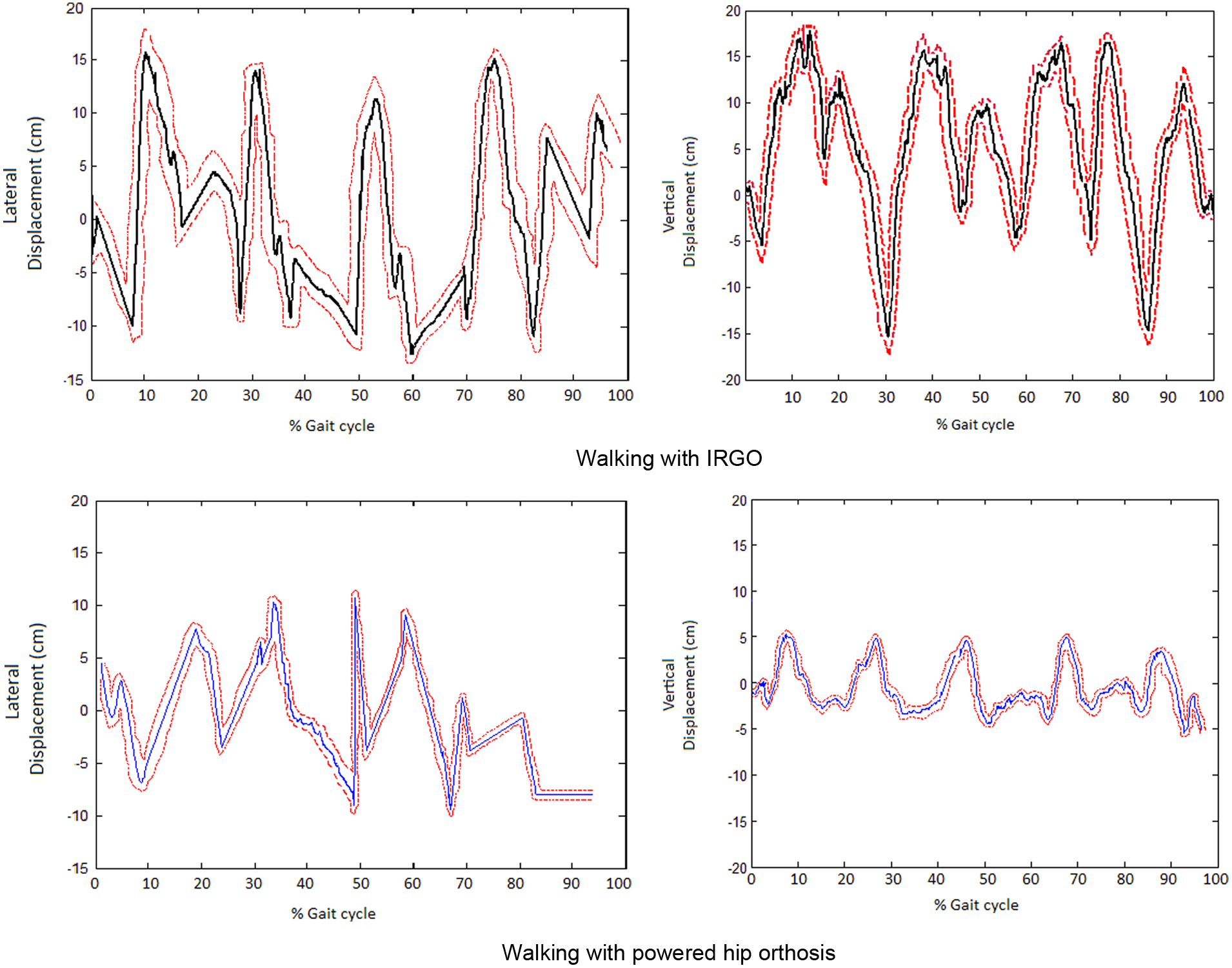
Lateral and vertical compensatory motion for a spinal cord injury (SCI) patient walking with mechanical Isocentric Reciprocating Gait Orthosis (IRGO) and new hip-powered orthosis.
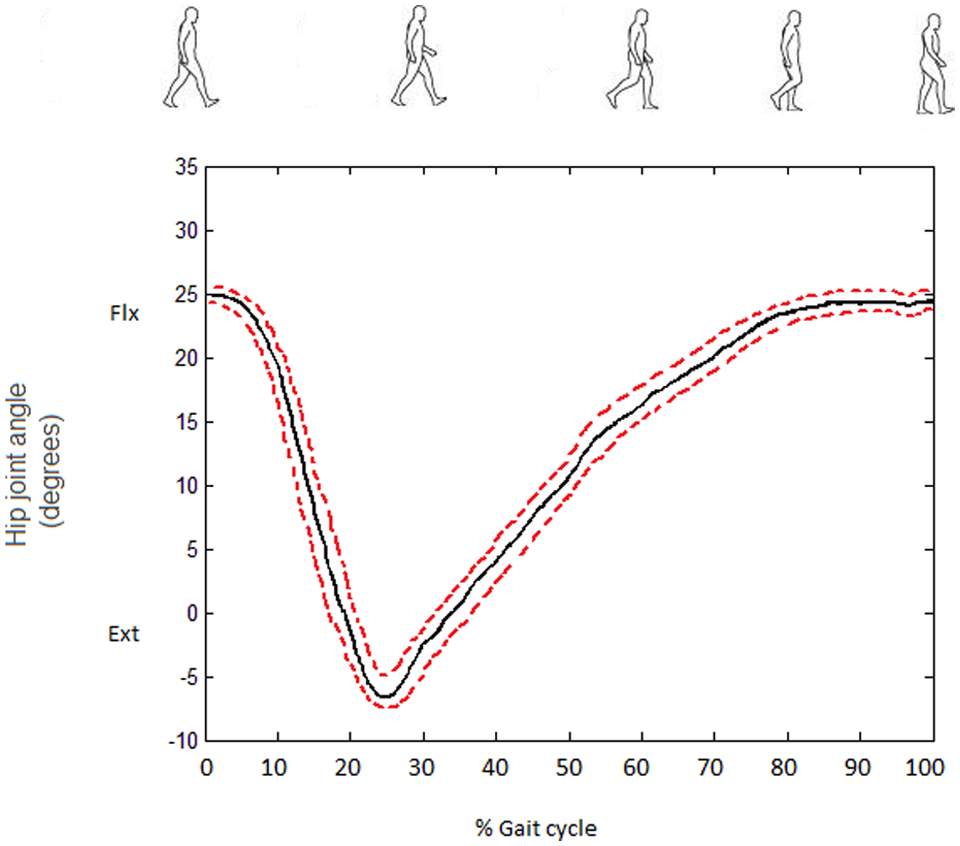
Table 2 and Figure 6 show means of hip angle in walking with IRGO and the powered hip orthosis. Both of the orthoses showed reduction of flexion and extension rates as compared to normal gait.
Hip angle (degree) with Isocentric Reciprocating Gait Orthosis (IRGO) and powered hip orthosis.

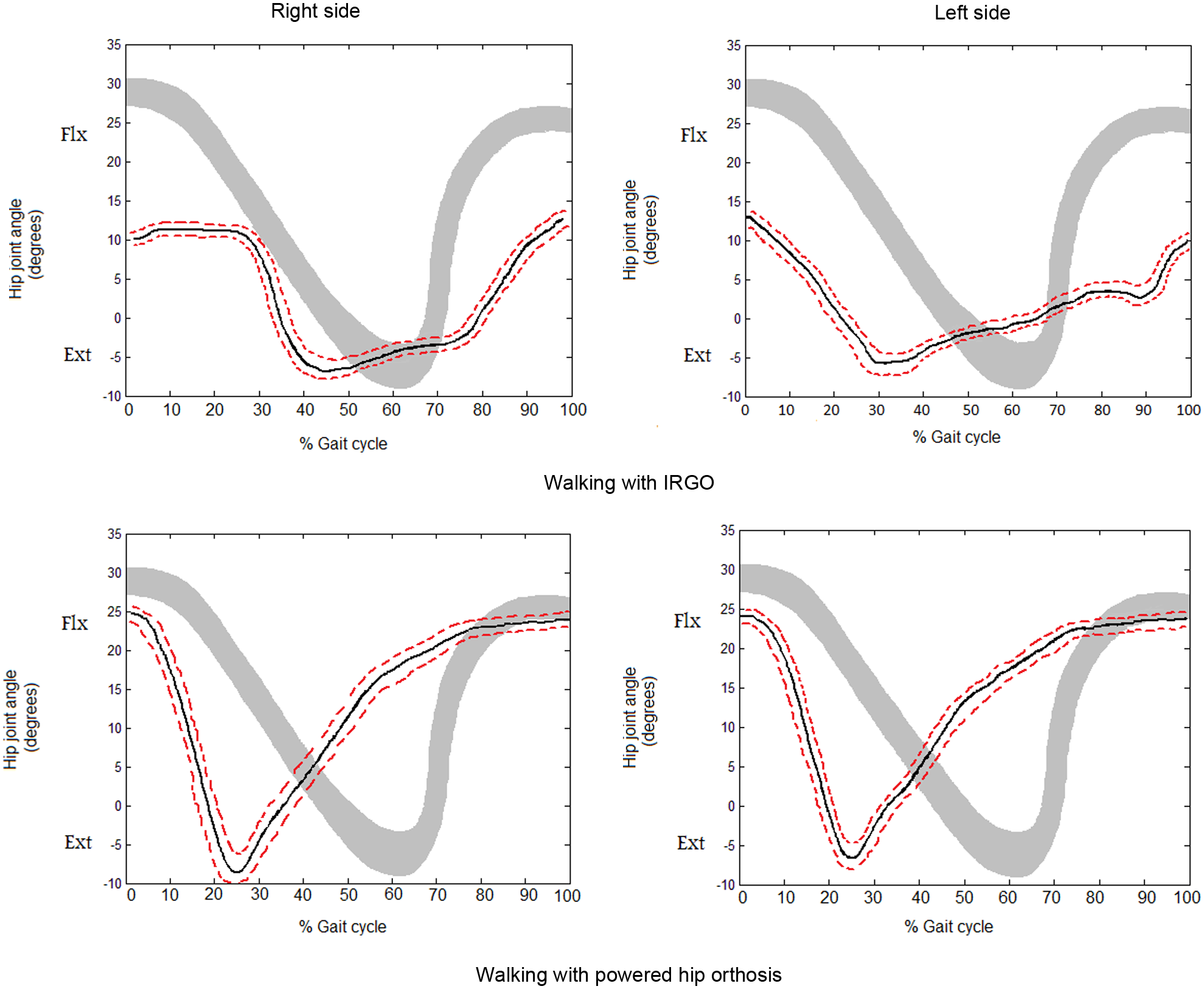
Flexion and extension of hip joint for a spinal cord injury patient walking with mechanical Isocentric Reciprocating Gait Orthosis (IRGO) and new hip-powered orthosis.
Discussion
In this study, we introduced a powered hip orthosis that was suitable for level-ground walking. Current approaches to the design of powered orthoses have typically focused on the use of pneumatic actuators or DC motors systems directly coupled to the hip joint.3,5,7,13 Ohta et al., who motorized an advanced reciprocal gait orthosis (ARGO), needed a high electrical power consumption to pull the mechanical cable of the hip joint reciprocal link even during level-ground walking. It may not be feasible for patients to participate in ADL with the Ohta powered hip orthosis, because of the bulky design of the motorized hip actuation mechanism. 5 Audu et al., who designed the variable constraint hip mechanism (VCHM) powered orthosis, produced a low walking speed relative to normal walking when utilizing the device. In addition the orthosis weight was 22 kg and so was very heavy. 14 Kang et al., used a pneumatic actuator to apply external forces for ambulation by subjects with a powered hip orthosis, but of the power generation by this type actuator as compared to DC motor is low. 7 In this case study, we proposed the design and construction of a powered hip orthosis that involved reciprocal movements using power applied to an existing design of rotating connector, which performed as a reciprocal link during stance and swing phase. The addition of the actuator added extra bulk to the orthosis but only to one limited area. The development of smaller-sized electrically-powered actuators for this application would help to alleviate this disadvantage in the future; particularly since the power requirements have been confirmed by this study (albeit for a single SCI patient). In addition, the method of attachment may be altered to give a more cosmetic appearance via additional gearing. Development of more advanced techniques in measuring the power requirements of individual patients when walking in a powered RGO and matching that to a convenient and repeatable power application for individual subjects would be a distinct advantage in the future.
In this case study, we evaluated kinematics and temporal-spatial parameters of walking by a SCI patient with the orthosis. Based on our results, walking speed and step length as compared to the un-adapted IRGO increased, resulting in a potentially more appropriate hip orthosis for level-ground walking. Our results were similar to those reported in previous studies in this field. The mean walking speed with a powered hip orthosis designed by Audu et al. using pneumatic actuators in healthy subjects was 0.8 m/s. The excessive weight of the orthosis was one drawback of this system as it was the main reason for a decrease in walking speed when worn. 14 One effect demonstrated when walking with any of the previous mechanisms was a decrease in the hip extension angle during late stance compared to normal walking. In this study, the IRGO and the powered hip orthosis had an extension angle of 5.5±1.6° and 8±1.5°, respectively, while the mean is 13° for the normal walking subject. The maximum hip flexion angle in the IRGO and powered hip orthosis were 12.5±2.2° and 25±1.8° respectively. These means in walking with IRGO were also less than normal human gait, but the overall hip motion demonstrated that it more closely resembled that of a normal human pattern (Figure 6).
However, the maximum hip extension angle was reached much earlier than during normal gait when walking in the powered orthoses (25% +/-2.2SD of the gait cycle for both sides), compared to 32% +/-1.8 (left side) and 42% +/-1.6 (right side) with the standard IRGO. The powered RGO therefore demonstrated a symmetrical timing of the peak hip extension timing point during gait while the standard IRGO did not. The timing of maximum hip extension for the IRGO was, however, closer to that of normal gait (approximately 62% of the gait cycle). This would indicate the need to adjust the power application rate in the powered RGO to reduce the velocity of hip extension induced by the motors and increase the rate of hip flexion while maintaining this within safe limits and also while maintaining the hip ROMs achieved. The alteration to hip flexion/extension timing ratio demonstrated in both the orthoses compared to normal gait may be attributed to the fact that both knees were fixed in extension and ankles were also fixed, meaning more ground clearance was needed and therefore an increase in the time to reach the maximum extension attainable was required. While the inclusion criteria to participate in the study stated full hip ROM for the patient, this was not necessarily needed following analysis of the results. It was, however, included initially to ensure that the hip was not forced past its passive full ROM while walking in the orthosis. It is feasible that future studies may be able to more accurately define the inclusion criteria to a definitive flexion and extension range.
When activated, lateral and vertical compensatory motions reduced with the powered orthosis due to the fact that the actuator induced flexion and extension of the hip joint (Figure 5). Instead of the patient using trunk muscle, the powered hip orthosis assisted in swinging the paralysed lower limbs which may have been responsible for the reduction of compensatory motions demonstrated, and which could potentially reduce the effort required to walk. The results of this study were similar to those reported by Ohta et al. 3 which is in contrast to those reported by Saito et al. where lateral motion using the medial single hip joint knee ankle foot orthosis (MSH-KAFO) increased. An anterior trunk position with the knees in full extension was thought to have caused an increase in lateral motion in walking with this type of orthosis. 15 This may have also resulted in more loading to the upper limbs, but this hypothesis needs to be tested on a larger sample of SCI subjects than has been previously reported.
Cadence was increased with the newly developed orthosis along with speed and stride length. This was also reported in a different study involving the Korean powered hip orthosis. 7
A limitation of the case study was that the results were only representative of a single subject. A series of walking trials with an appropriate number of SCI subjects with differing levels of functional ability would need to be performed in order to gain further insight into the repeatability of the results. We also used a walking aid during the walking trials which was wider than usual in order to accommodate the actuator which was positioned on the lateral aspect of the pelvic section of the orthosis. This may be addressed during future development work by reducing orthosis bulk. Nevertheless, the development team was sufficiently encouraged by the results from this initial testing to confidently continue testing and development of the device for use by SCI subjects.
Conclusions
A powered hip orthosis with bi-directional movement by a single actuator was proposed. The hip employs one actuator component which was designed to minimize weight of the orthosis and to help the kinematic efficiency of level-ground walking when utilizing the orthosis. The hip motor performed positive effects on the gait parameters (speed, step length and lateral sway) during level-ground walking trials, resulting in an alternative approach to walking in SCI patient’s gait.
Future work with this powered hip orthosis design will include development of the hip control, and also the need to reduce orthosis bulk by utilizing a more compact motor and a more cosmetic method of mounting it onto the device. Development of more advanced techniques in measuring the power requirements of individual patients when walking in a powered RGO and matching that to a convenient and repeatable power application for individual subjects would be a distinct advantage in the future.
Additionally, future work should be performed on the incorporation of a motorized knee joint to improve orthosis effectiveness to gait parameters. This new design will permit better knee joint movement and improved gait parameters and gait patterns for paraplegic gait. The lower limb muscles of SCI patients tire easily. For increased muscle endurance, it is appropriate for subjects to undertake treadmill training prior to orthosis use.
We hope that this case study will motivate additional research focused on the advancement of powered lower limb orthoses for walking in SCI patients. Simultaneous activity of knee and hip joints to provide near normal walking and improvements in control technology should be performed in future investigations.
Footnotes
Funding
This material was based on work supported by the Deputy of Research and Technology of the University of Social Welfare and Rehabilitation Science (grant number 90.801.1.7296).