
Abstract
Background:
The important purpose of a powered gait orthosis is to provide active joint movement for patients with spinal cord injury.
Objectives:
The aim of this study was to clarify the effect of a powered gait orthosis on the kinematics and temporal–spatial parameters in paraplegics with spinal cord injury.
Study Design:
Quasi-experimental.
Methods:
Four spinal cord injury individuals experienced gait training with a powered gait orthosis for a minimum of 6 weeks prior to participating in the following walking trials: walking with an isocentric reciprocating gait orthosis and walking with both separate and synchronized movements with actuated orthotic hip and knee joints in a powered gait orthosis. Specific parameters were calculated and compared for each of the test conditions.
Results:
Using separate and synchronized actuated movement of the hip and knee joints in the powered gait orthosis increased gait speed and step length and reduced lateral and vertical compensatory motions when compared to the isocentric reciprocating gait orthosis, but there were no significant differences in these parameters. Using the new powered gait orthosis improved knee and hip joint kinematics.
Conclusions:
The powered gait orthosis increased speed and step length as well as hip and knee joint kinematics and reduced the vertical and lateral compensatory motions compared to an isocentric reciprocating gait orthosis in spinal cord injury patients.
Clinical relevance
This new powered gait orthosis has the potential to improve hip and knee joint kinematics, the temporal–spatial parameters of gait in spinal cord injury patients walking.
Background
Mechanical orthoses such as hip knee ankle foot orthoses (HKAFOs) that include the walkabout, 1 the hip ankle-linked orthosis (HALO), 2 the prime walk, 3 para walker and hip guidance orthosis (HGO), 4 the advanced reciprocal gait orthosis (ARGO), 5 and the isocentric reciprocal gait orthosis (IRGO) 6 have all been used for patients with spinal cord injury (SCI) in their therapeutic treatment in providing standing and walking activities. Although the positive effects of mechanical orthoses are well demonstrated,7 –11 there are several reasons why an optimal level of walking for SCI patients has not been achieved, especially due to the high energy consumption and overloading on upper limb joints when walking with mechanical orthoses.11 –15 Paraplegic patients usually demonstrate high energy consumption when walking with an orthosis because they use compensatory motions of the upper limb and trunk for forward propulsion and swinging of the lower limbs.16 –18 The use of a powered lower limb orthoses may offer a solution to resolving these drawbacks. 19
Powered lower limb orthoses can be useful devices for walking and standing in SCI patients. 20 The purpose of these orthoses is to provide torque to targeted joints (e.g. the ankle, knee, or hip) during walking. 21 Ideally, this mechanical assistance is designed to produce overall kinematic patterns similar to that of normal walking. The use of a powered orthosis has been shown to provide better function in terms of gait parameters compared to a mechanical orthosis.22 –25
The effectiveness of this type of orthosis has been demonstrated in previous studies in this field. Kang et al. 23 reported that hip flexion angles and the pelvic angle were both reduced during walking with a powered orthosis, but walking speed was increased compared to an reciprocal gait orthosis (RGO). Ohta et al. 22 demonstrated that both gait speed and the step length increased when the knee and hip joints were actuated by a powered RGO. The cosmesis of walking may be improved, and lateral and vertical compensatory motions reduced when hip joint actuators are activated. Arazpour et al. 24 reported that a powered hip orthosis provided positive effects on the kinematics and temporal–spatial parameters of gait during level-ground walking trials as compared to an IRGO. Kawashima et al. 25 showed that the weight-bearing control orthosis (WBCO) enabled SCI patients to walk with a higher speed than mechanical orthoses when using similar energy expenditure. Walking with the WBCO also leads to improvement of the energy cost of walking in a paraplegic patient, even though they only provided power to one joint (e.g. the hip or ankle). A powered gait orthosis that has synchronized powered movement between the hip and knee joints has recently been designed and developed, and its effectiveness on the gait of a single SCI subject has been reported. Arazpour et al. demonstrated that improvements in step length, speed of walking, and cadence were observed in walking with the new powered gait orthosis as compared to the standard IRGO. Maximum hip flexion and extension angles, as well as the maximum knee flexion and extension angles, all increased. In addition, lateral and vertical compensatory motions were reduced with powered gait orthosis compared to an IRGO. 26 In this study, we aimed to evaluate the effect of a similar powered gait orthosis with synchronized actuated movement between knee and hip joints on the temporal–spatial parameters and kinematics of orthotic gait on a series of volunteer SCI patients.
Methods
Subjects
Four patients, who were recruited from a referring consultant, with a thoracic level SCI participated in this study. Three subjects had an incomplete and one had a complete motor paralysis in the lower limb muscles based on the American Spinal Injury Association (ASIA) classification, 27 grade A or B. Inclusion criteria included no evidence of cardiovascular or pulmonary disease, contractures, severe spasticity, obesity, nor asymmetric hip positions, and at least a period of 6 months postinjury before the commencement of the study. Table 1 shows the characteristics of the patients who participated in this study. All subjects had experience of walking with an IRGO with a walking frame with the wheels positioned anteriorly and had undergone at least 6–10 weeks of orthotic gait training using the powered gait orthosis before the testing period. Each patient gave written informed consent for the experimental and training approach, which was approved by the Ethics committee of the University of Social Welfare and Rehabilitation Science. The Ethics Committee of University approved the performance of this study.
Characteristics of the SCI subjects.
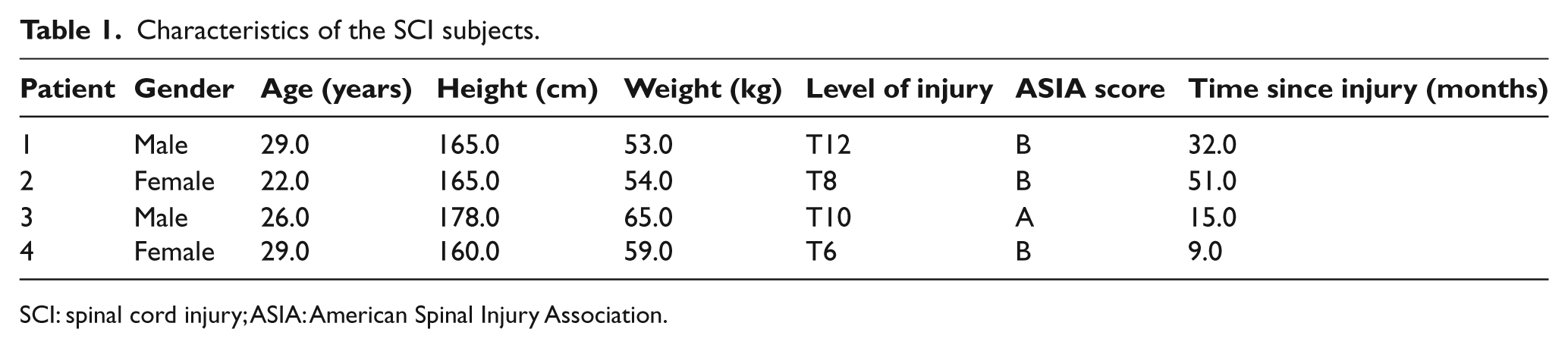
SCI: spinal cord injury; ASIA: American Spinal Injury Association.
Orthotic gait
The patients performed orthotic gait training with a powered gait orthosis for a minimum of 6 weeks, at 1 h/day for 5 days/week prior to the walking trials. After the prescribed training times with the new powered gait orthosis, each patient could walk with the new powered orthosis independently and were able to walk continuously. The mechanical features of the powered gait orthosis have been fully explained in a previous study. 28 In short, the new orthosis provides synchronized and powered motion to the hip and knee joints but is also capable of generating movement when only the hip actuator or knee joint actuator is activated separately. 26 With this orthosis, the torque provided by the knee and hip joint actuators is designed to actively move the orthotic hip and knee joints of the orthosis.
This powered design therefore potentially enables a SCI patient walk at a faster speed and with less compensatory motions when compared to a mechanical IRGO. 26 The powered gait orthosis that was used in this study is shown in Figure 1.

The new powered gait orthosis used in this study.
Motion analysis
Patients performed orthotic walking along a 6-m walkway in the gait analysis laboratory five times with a comfortable and self-selected speed in four test conditions when wearing each of the two gait orthoses (IRGO, powered IRGO with synchronized knee and hip joints, IRGO with only powered hip joints, and IRGO with only powered knee joints). In order to obtain the kinematic parameters during gait, the gait analysis was assessed with a three- dimensional motion analysis system (VICON 370; Vicon Motion Systems Ltd, Oxford, UK). The motion analysis system included a video analysis system with six cameras and force plates (Kistler, Switzerland). A total of 18 markers were put to the trunk of the patients and on the orthosis as close as possible to the positions where they would be located on the patient’s skin at the following positions: bilaterally over the position of the greater trochanter, the lateral condyle of the femur, the head and lateral malleolus of the fibula, the second metatarsal, anterior superior iliac spine (ASIS), calcaneus, and over the jugular notch, the spinous process of the seventh cervical vertebrae and the acromioclavicular joints.
Two step cycles were chosen for the gait evaluation (i.e. one right and one left to replicate a complete stride) that were averaged from the five walks for each condition. There were no significant differences between left and right.
The temporal–spatial and kinematic parameters that were assessed following the gait analysis included cadence, step length, speed of walking, hip and knee joint ranges of motion (ROMs), and vertical and lateral compensatory motions. The compensatory motions were analyzed by measuring the maximum horizontal excursions of the shoulders and the maximum vertical excursion of the C7 vertebral body using markers placed on these positions.
Statistics
The Kolmogorov–Smirnov technique was used to confirm the normality of data, a one-way analysis of variance (ANOVA) was used for comparing means of parameters in walking with the orthotic conditions. SPSS statistical software was used for the analysis of the data. The level of significance was set at 0.05. One-way ANOVA was completed for each spatiotemporal and kinematic gait parameter that was measured, that is, one for cadence, step length, speed, hip flexion, hip extension, knee flexion, and lateral and vertical compensatory motions. Each ANOVA consisted of a single within-subject–dependent variable (i.e. condition) with four levels corresponding to each of the four orthotic conditions. This produced a main effect for the variable “condition” for each of the eight parameters (ANOVAs). When there was a significant main effect between orthotics using conditions, Bonferroni post hoc analysis was performed to determine which conditions were significantly different.
Results
Gait speed, step length, and cadence
Between IRGO and actuators operations situations
The mean of walking speed, cadence, and step length calculated during walking in the motion analysis laboratory in four conditions of orthosis is shown in Table 2. There was no significant difference between and IRGO and new powered orthosis and isolated activation of knee and hip joint actuators in speed of walking, step length, and cadence (Table 3).
Mean ± SD of gait parameters when comparing the actuator operating conditions and the IRGO.
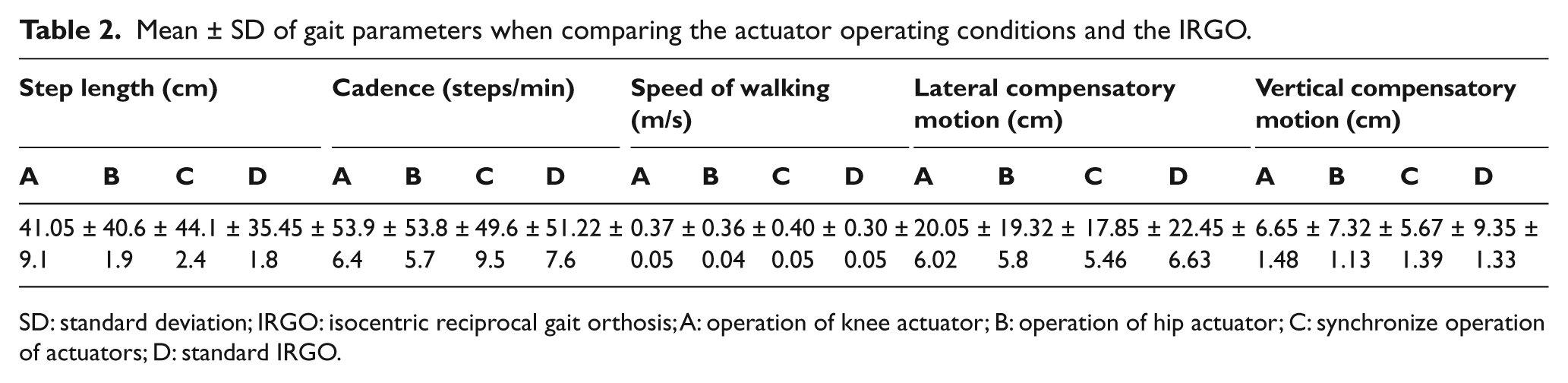
SD: standard deviation; IRGO: isocentric reciprocal gait orthosis; A: operation of knee actuator; B: operation of hip actuator; C: synchronize operation of actuators; D: standard IRGO.
Comparison of gait parameters between comparing the actuator operating conditions and the IRGO.

IRGO: isocentric reciprocal gait orthosis.
Differences between actuator operation situations
In comparing the resulting effects on step length, cadence, and speed of walking when activating the hip or knee actuators in isolation compared with synchronized activation, there was no significant difference between the synchronized condition and isolated activation of knee and hip joint actuators in speed of walking, step length, and cadence. When comparing isolated activation between hip and knee actuators, there were no significant differences between them in speed of walking, step length, and cadence (Table 3).
Lateral and vertical compensatory motions
Between IRGO and actuators operations situations
Table 2 shows the mean and standard deviation (SD) of these parameters during orthotic walking. Isolated and synchronized activations of the powered gait orthosis improved lateral and vertical compensatory motions compared to when walking with the IRGO, but similar to spatial–temporal parameters, there was no significant difference between orthotic walking conditions (Table 3).
Comparison of actuator operation conditions
In comparing between the synchronized condition and the isolated activation of knee and hip joint actuators, there was no significant difference demonstrated between isolated activity of the knee joint actuators and synchronized activation of the actuators in the new powered gait orthosis in lateral and vertical compensatory motions. Significant differences were not observed between isolated activation of the hip joint actuators and synchronized activation of both actuators in the new powered gait orthosis in vertical and lateral compensatory motions. In addition, there were no significant differences demonstrated between isolated activation of the knee joint actuators and the hip joint actuators in these two parameters (Table 3).
Kinematics
Hip angle
Table 4 shows mean ± SD of hip flexion/extension during orthotic walking. The maximum hip flexion and extension angles were 18.75° ± 2.36° and 7.75° ± 0.95°, respectively, when walking with the new orthosis, but average flexion and extension angles were 9.25° ± 0.95° and 5.5° ± 0.57°, respectively, in walking with the standard IRGO. There were therefore significant differences in flexion and extension parameters between orthotic walking conditions with regard to one-way ANOVA analysis (Table 4).
Mean ± SD of the hip and knee ROMs when comparing the actuator operating conditions and the IRGO.
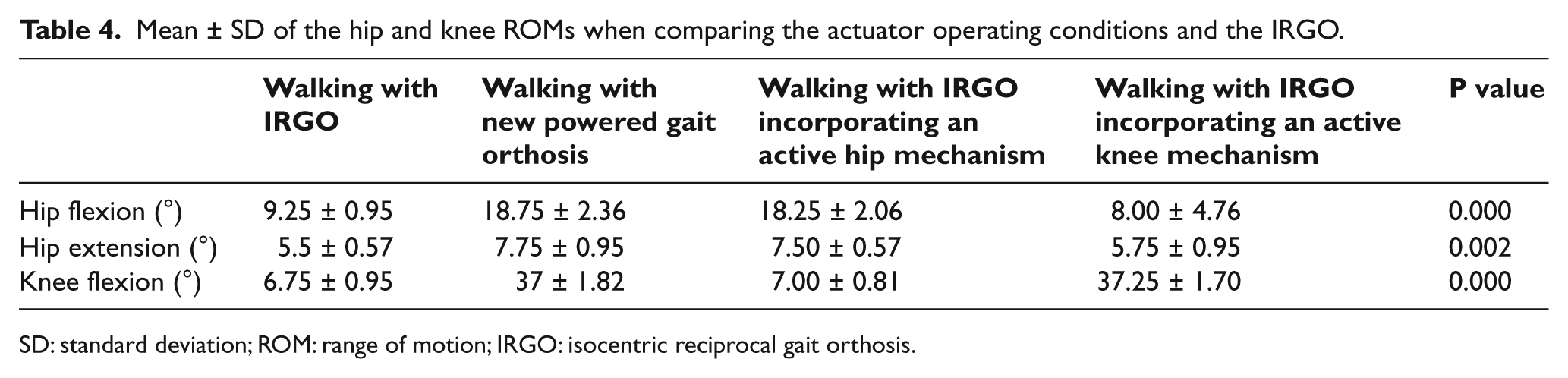
SD: standard deviation; ROM: range of motion; IRGO: isocentric reciprocal gait orthosis.
In hip extension, there was a significant difference between new orthosis and IRGO (P = 0.010). In comparison of this parameter between IRGO and IRGO incorporating an active hip mechanism (isolated operation of hip joint actuator), there was a significant difference (P = 0.023). However, there was no significant difference between IRGO incorporating an active hip mechanism (isolated operation of hip joint actuator) and IRGO incorporating an active knee mechanism (isolated operation of knee joint actuator) (P = 0.052).
According to a significant effect between orthotics using conditions in hip flexion/extension, Bonferroni post hoc analysis was used. In hip flexion, there was a significant difference between new orthosis and IRGO (P = 0.003). In comparison of this parameter between IRGO and IRGO incorporating an active hip mechanism (isolated operation of hip joint actuator), there was a significant difference (P = 0.005). In addition, there was a significant difference between IRGO incorporating an active hip mechanism (isolated operation of hip joint actuator) and IRGO incorporating an active knee mechanism (isolated operation of knee joint actuator) (P = 0.002).
Knee angles
Table 4 shows the mean ± SD of knee joint flexion during orthotic walking. Walking with powered gait orthosis showed maximum knee flexion angles of 37° ± 1.82°, which was much improved compared to the maximum knee flexion angle of 6.75° ± 0.95° during the swing phase of gait, which was achieved when walking with the standard IRGO. There was therefore a significant difference between the orthotic walking conditions in this parameter (P < 0.001) (Table 4).
In knee flexion, there was a significant difference between new orthosis and IRGO (P < 0.001). In comparison of this parameter between IRGO and IRGO incorporating an active knee mechanism (isolated operation of knee joint actuator), there was a significant difference (P < 0.001). In addition, there was a significant difference between IRGO incorporating an active hip mechanism (isolated operation of hip joint actuator) and IRGO incorporating an active knee mechanism (isolated operation of knee joint actuator) (P < 0.001).
Discussion
The present study demonstrates the orthotic gait performance when walking with a powered gait orthosis by patients with spinal cord lesions ranging from T6 to T12 level. Provided adequate aerobic capacity is available for the SCI patients, walking with orthosis allows safe walking. The high energy consumption experienced and fatigue in upper limbs by this patient group have been shown to be problematic when walking with an orthosis.11,12 Using a powered orthosis appears to be one solution to decrease these problems. 19
During walking with a mechanical orthosis (e.g. the ARGO or IRGO), contraction of the trunk muscles and compensatory motions are important for providing hip flexion in SCI subjects, which can cause high loads on upper limb joints.16,18 Patients with an upper level lesion at thoracic level will have excessive loads applied to the upper limb joints and limited ROM of their hip joints. 29 In our study, based on activated motions of hip and knee joints, patients demonstrated smaller compensatory motions than when walking with the IRGO, but these did not reach a significant level. In addition, patients anecdotally stated than they perceived having to use less effort when walking with the new powered gait orthosis. This may have been due to power application to the hip and knee joints.
SCI patients with higher levels of thoracic injury demonstrated smaller hip ROMs when compared to patients with lower thoracic lesion levels when walking with the IRGO and also the powered orthosis. Due to paralysis of the trunk muscles and muscles around the hip joint, the power produced by trunk muscle contractions for providing compensatory motion and leg swing is insufficient in high thoracic level patients, which may explain the slower gait speed and shorter step lengths evidenced when using an IRGO. Using actuators in the hip and knee joints and adding synchronized movement using these actuators in the new gait orthosis caused active motions in hip and knee joints, which were effective in replacing the loss of function caused by paralysis of muscles, which resulted in small increases in speed and step length during the walking tests, but these did not reach a statistically significant level. Compensatory motions also reduced when walking with this active mechanism, but again, not significantly.
When compared to the previous studies in this field, where the temporal-spatial parameters and kinematics were measured in walking with powered orthoses and mechanical orthoses (e.g. the IRGO and ARGO), our results showed faster gait speeds and improved step lengths. The walking speed and step length demonstrated in walking with motorized ARGO by Ohta et al., 22 with powered hip orthosis Arazpour et al., 24 and with WBCO by Kawashima et al. 25 were all slower and shorter, respectively, than that shown in this study. The walking speeds reported in the studies by Leung et al., 30 Massucci et al., 11 and Ijzerman et al., 18 which used IRGOs and ARGOs, were initially slower than that shown in this study. Patients in this study initially had a slower walking speed. Following their initial period of gait training with new orthosis, they had acquired walking skills with the new orthosis and thus improved their kinematics and temporal–spatial parameters when walking with new orthosis during the walking trials.
Gait training of SCI patients is essential and an important activity for them. Therefore, it is important to find an approach to decrease the high loads on the upper limbs during ambulation and to reduce energy consumption, by providing a gait training effect during walking with an orthosis. Many studies have been performed in this field for these purposes and have utilized functional electrical stimulation (FES) 31 and the application of external power sources (e.g. pneumatic, hydraulic, and motor).22,23,32 The effectiveness of FES in combination has been shown to reduce energy cost, but rapid muscle fatigue remains to be a problem. 31
Walking with an orthosis produces a high energy cost. A direct relationship between orthotic gait function and the level of lesion in SCI patients has been demonstrated. 29 Walking with a mechanical orthosis produces a slow speed of walking and high energy consumption in SCI patients, especially those with a high thoracic level of injury. Limited hip motion can contribute in causing these problems and also can result in high loading to the upper limb joints. 29 In this study, hip and knee activation produced reduced compensatory motions when walking with the new orthosis. According to these results, the new orthosis may be capable of reducing the energy consumption and fatigue in walking with powered orthosis in SCI patients. While this has not been evaluated or proven, assessment of it would be beneficial in the future studies.
Robotic devices (e.g. the Locomat and the Gait trainer) assist stepping in SCI patients in a clinical environment. 33 These robots can actively assist and guide the lower limbs of patients based on applying preprogrammed physiological gait patterns in the hip and knee joints. These robotic devices are capable for use in a clinical situation, but using them out of the clinical environment is not possible. The advantage of this new powered gait orthosis is programmable movement in hip and knee joints, the ability to use it both in a clinical environment and at home. The main effects of walking with this new powered orthosis by SCI subjects were that it increased maximum knee flexion angles and hip extension and flexion angles and increased step length and walking speed. It also reduced compensatory motions. These effects could prove to be advantageous in helping SCI subjects to walk more efficiently with a powered RGO. One disadvantage of this orthosis is that it only assists the hip and knee joints. The ankle joints also have an important role in walking. 34 Feedback from the ankle joint afferent feedback is critical to the control of walking. 35 Because of its relative importance to the mechanics and control of walking gait, providing assistance at the ankle joint during walking with a new gait orthosis may be important. In this study, we used a solid ankle joint, but design and fabrication of a powered gait orthosis with movable ankle joints would be beneficial in walking with a powered orthosis in a future design.
There were several limitations to this study. The number of participants recruited was low, and it was therefore not possible to represent the patient sample in this study as being typical of that for the general SCI subject population. Second, the low number of participants meant that no statistical differences were found for the stride parameters or compensation motion, although these outcome parameters showed high effect sizes. A larger sample size may have demonstrated more additional significant differences between the test conditions for the parameters analyzed. In addition, energy consumption, heart rate, and perceived effort were not measured during this study, which would be needed to compare the efficacy of the devices tested for SCI subjects.
Conclusion
The important aim of a powered gait orthosis is to provide active joint motion for patients with SCI and a standing support for these individuals. A powered gait orthosis enables SCI patients with thoracic level injuries to walk at relatively higher speed and increased step length than when compared to an IRGO. The special powered gait orthosis used in this study demonstrated reduced vertical and lateral compensatory motions during walking. Separate activation of the hip or knee actuators was more effective than the IRGO in improvement of the speed of walking, step length, and joint kinematics and reduced compensatory motions. The most effective improvement of kinematic and temporal–spatial parameters was achieved when synchronized movement of hip and knee joints was performed. Therefore, the new powered gait orthosis could be an effective orthosis in rehabilitation for thoracic level SCI patients.
Footnotes
Conflict of interest
The authors have no conflict of interest in this study.
Funding
We thank the Iranian National Science Foundation (INSF) for financial support (grant number 91001980) for this research.