
Abstract
Background: The aim of this case study was to analyze the effect on gait parameters of a new design of powered gait orthosis which applied synchronized motions to both the hip and knee joints when utilized for walking by a spinal cord injury (SCI) patient.
Case Description and Methods: Two orthoses were evaluated while worn by an incomplete SCI subject. Gait evaluation was performed when walking with an isocentric reciprocating gait orthosis (IRGO) and compared to that demonstrated by a newly developed powered version. This new orthosis was based on the IRGO superstructure but incorporated powered hip and knee joints using electrically motorized actuators.
Findings and Outcomes: These gait parameters were improved when compared to standard IRGO and initial testing with the orthosis with only the hip or the knee joints activated in isolation. Maximum hip flexion and extension angles, as well as the maximum knee flexion and extension angles all increased when walking with the powered RGO compared to the IRGO.
Conclusions: Gait evaluation of this newly developed orthosis showed improvement in measured parameters when compared to walking with an IRGO.
This case study gave the authors confidence to extend the research to a more extensive study with a group of SCI patients.
Background
Walking ability is important for enhancing the quality of life and the ability to participate in social and economic life for spinal cord injury (SCI) patients. Upright ambulation has psychological, physiological and therapeutic benefits for lower limb paralysis.1-5 Many approaches have been developed to assist people with SCI in standing and walking, such as the use of passive mechanical orthoses, hybrid mechanical orthoses in conjunction with functional electrical stimulation (FES) and active powered orthoses. 6
Different systems using passive mechanical orthoses have been introduced in the rehabilitation of SCI patients, such as hip knee ankle foot orthoses (HKAFOs), hip guidance orthoses (HGOs) and reciprocal gait orthoses (RGOs). Studies have demonstrated that the walking ability of paraplegic subjects may be improved using these devices. Despite the benefits of ambulation provided by passive mechanical orthoses, the evidence suggests that regular or continued long-term use of this type of orthosis is low.4,7-14 There are many compounding factors for this, such as increased mechanical load experienced on upper limb joints and the high metabolic expenditure experienced during ambulation.4,8,12,15-16 If active hip motion could be provided by an actuator acting on the hip and knee joints of such orthoses, patients would feasibly not require as much effort or trunk movement to facilitate propulsion during paraplegic ambulation compared to non-powered (passive) orthoses.
Unlike passive orthoses, active powered orthoses can control the mechanical joints used in an orthoses. 17 This has potential benefits for SCI subjects. For instance, using active flexion provided by an actuator attached to an orthotic knee joint may provide an improvement in foot clearance during swing phase leading to more normal walking patterns in SCI patient gait. 18 In addition, power generation using actuators during paraplegic patient walking with active powered gait orthoses, has demonstrated that less effort is needed by subjects to walk with lower mechanical forces being inferred on the upper limb joints. 18
Recently, powered gait orthoses have been introduced as a new rehabilitation approach for training and walking of SCI patients, which have produced more functional gait patterns compared to passive mechanical orthoses.13,18,19 Pneumatic actuators using artificial muscles have been developed since the mid-1970s, 20 but their effect on gait parameters when added to orthoses designed for SCI subjects has demonstrated the achievement of low walking speeds with the need for additional support via assistive devices. 20 Yano and colleagues developed a mechanical reciprocal gas-powered orthosis acting at the foot and ankle region. This orthosis enabled SCI patients to walk with lower energy costs compared to conventional orthoses. 21 Belforte et al. also proposed a pneumatic active gait orthosis which was intended to assist walking in paraplegic subjects including those with high level lesions. 22 Rutenberg et al. designed a powered gait orthosis with single degree of freedom by using DC motors, 23 and Kong et al. designed a tendon-driven power assistive device for elderly patients. The tendon connecting the motors to the pulleys which were positioned at the hip and knee joints generated the required assistive power. 24
Ohta and colleagues developed a two degree of freedom motor-powered gait orthosis for use by five volunteer SCI patients using actuators acting on the knee and hip joints of the device. However, these actuators were not synchronized and could only be used separately. The results from walking with only the knee actuators acting demonstrated an increased gait speed and step length in all subjects, 18 along with a decrease in compensatory motions in both the lateral and vertical directions. This resulted in a more cosmetic gait compared to previous designs. Sung Jae Kang and colleagues more recently developed a new powered orthosis using pneumatic actuators.16,19
Most powered gait orthoses have historically been designed as part of research projects in academic centers, meaning currently there are no commercially-developed powered orthoses available which administer active assistance for ambulation by SCI patients. These patients ideally need powered orthoses to offer assistance during daily activities and to facilitate more normal walking patterns.
Great advancements in robotic technology have occurred in recent decades (e.g. improvement in control methods, development of lighter weight devices and use of smaller actuators with high power, and more effective sensors), meaning robotic technology could be used to power lower limb orthoses for walking and facilitate the possibility of them becoming commercially viable. DC motors have been used to power mechanical orthoses by being applied to the hip and knee joints in recent years, but co-activation of these joints in one gait cycle has not been achieved in reciprocal orthotic devices. Performance and improvement of this function could feasibly advantageously affect walking patterns in SCI patients.
In this study we developed a novel powered isocentric reciprocal gait orthoses (IRGO) to improve the walking of SCI patients. To achieve this aim, a mechanical IRGO was fitted with electric motors to simultaneously assist hip and knee joint movements. The hypothesis was that the simultaneous application of power to both the hip and knee joints bilaterally to an IRGO would advantageously alter specific gait parameters when used by a SCI patient compared to an un-adapted version of the orthosis.
Case Description and Methods
Experimental protocol
A female patient (age 22 years, weight 54 kg and height 165 cm, with an incomplete lesion at T8 level) participated in the study. She was an experienced IRGO user with normal upper limb strength. She had no cardiovascular or pulmonary disease, contractures, severe spasticity, obesity, nor asymmetric hip positions, which would have negated her participating in the study. The study was approved by the Ethics committee of the University of Social Welfare and Rehabilitation Science. A standard IRGO and a single prototype powered gait orthosis equipped with electrically powered motors were analysed when used for walking by the volunteer subject.
The patient walked through a 6-m long calibrated space monitored by a 16-Camera Vicon digital motion capture system (Oxford Metrics, UK) using a capture frequency of 100 Hz when wearing each of the two gait orthoses in turn. Fifteen retro-reflective markers were used on the lower extremity and four were placed on the trunk. Markers were placed bilaterally over the position of the greater trochanter, the lateral condyle of the femur, the head and lateral malleolus of the fibula, the second metatarsal, both ASIS, the calcaneus, and over the jugular notch, the spinous process of the seventh cervical vertebrae and the acromio-clavicular joints. The cameras captured the locations of reflective markers placed on the orthoses. The markers of lower limb joints were placed on the uprights of the orthoses as close as possible to the positions where they would be located on the patient’s skin. The patient walked in a straight path along the walkway, and performed practice walks in the gait laboratory to acclimatize to the orthosis before data capture commenced. For all experimental walks with each orthoses, the volunteer SCI subject walked with a walking aid for stability and safety. For each test condition, the subject walked along the walkway five times.
Orthoses and orthotic configurations
The standard IRGO (Ortho-system – in motion) which was adapted to produce the prototype powered gait orthosis used in this study is shown in Figure 1. The novel powered gait orthosis was designed to achieve upright posture and ambulation for patients with SCI, and utilized finite state robot-based electrically actuated motors attached to the orthosis to perform active flexion and extension of the hip and knee joints to achieve the desired constraint states.

New powered gait orthosis used in this study.
The electronics and motor included a Maxon Motor EC30 (Maxon, Switzerland) with a planetary gearbox with reduction of 156 for the hip joints and Maxon Motor EC45 (Maxon, Switzerland) with a planetary gearbox with a reduction of 110 for the knee joints. The system also included encoders, motor drivers, a power supply and a programmable controller. The motor sequencing was based on models optimized by software specifically designed and built for this purpose. The orthotic joint motion patterns could then be programmed into the microcontroller to the main system. Using this approach, the actuators were capable of generating appropriate movement patterns at specified intervals during the complete gait cycle Figure 2. One rechargeable 24 V (Lipo Battery, Thunder Power RC G6 Pro Lite 25C 5400mAh 6-Cell/6S) was used in this orthosis. The batteries and control board were placed within a backpack which was worn by subject during orthosis-using time. The operation of the new powered gait orthosis during walking was initiated by the orthotist via a joystick. The orthotist advised the patient to transfer weight to the left foot, and the right side knee actuator was then activated which flexed knee joint followed by the ipsilateral hip joint actuator which flexed the hip joint. The patient then moved the pelvis forward on the same side. The right side knee actuator was activated again to extend the knee joint, after which the hip joint actuator was activated and hip joint extended. This function allowed the patient to transfer her weight to the right leg. This cycle was then repeated for the left foot. During all these stages the left side knee joint was locked in extension by the left knee joint actuator.

Walking with the new orthosis.
The standard orthosis was manufactured for the volunteer subject by utilizing casts of the lower extremity, lumbar and pelvic areas. The total weight of IRGO was 5 kg, while total weight of powered gait orthosis with batteries, sensors, cabling and electronics was 10.1 kg. Kinematics and relevant gait parameter data were calculated when walking under the following four test conditions: walking with the standard IRGO, walking with the new gait orthosis using synchronized and powered orthotic knee and hip joints, walking with power added to the orthotic knee joints only with the hip joints driven by the usual reciprocating mechanism of the IRGO, and walking with power only added to the hip joints with the orthotic knee joints remaining locked in extension at all times.
Three versions of the powered orthosis were directly compared in this study. This was done in order to identify the effect of synchronization of power to both the hip and knee joints concurrently during ambulation when compared to the effects noted when walking with either the hip or knee joint activated in isolation. It was thought that activation of both the hip and knee joints concurrently would improve gait parameters when compared to either the hip or knee joints being activated in isolation, but this needed to be demonstrated. In addition, the effect of using these three test conditions to add power to the various joints, either in synchronization or separately, needed to be compared to the results when walking with the standard IRGO to provide proof of concept that application of power to joints would improve gait parameters compared to an un-adapted non-powered orthosis.
The following parameters were measured during the walking trials: hip and knee flexion and extension angles, walking speed, step length and cadence, COM excursion, and lateral and vertical compensatory motions. The hip and knee angles were calculated using the relative positions of the greater trochanter, the lateral condyle of the femur, the head and lateral malleolus of the fibula, the second metatarsal, and both ASIS. Lateral and vertical compensatory motions plus centre of mass (COM) displacement were calculated by analyzing the motions of the ASIS, seventh cervical vertebral and acromio-clavicular markers.
Findings and Outcomes
Joint angles
Hip angle
When walking with the new orthosis, the maximum hip flexion angle was 26.5±1.5° and the maximum extension angle was 9±1.5°. In walking with the standard IRGO the average flexion and extension angles were low compared to those of the new orthosis. The overall effect of wearing standard IRGO demonstrated a reduction in the average hip extension angle to approximately 7±1° and reduced the maximum hip flexion angle to 13.5±1.3°.
Knee angles
Walking with the powered gait orthosis showed maximum knee flexion angles of 37.5±2.6°, but this was much improved compared to the maximum knee flexion angle of 8±1° during swing phase of gait which was achieved when walking with the standard IRGO.
Step length, walking speed, cadence and compensatory motion
Temporal/ spatial data for each subject when walking with both orthoses are shown in Table 1. Improvements in step length, speed of walking and cadence was observed in walking with new powered gait orthosis as compared to the standard IRGO.
Comparing gait parameters between new powered orthosis and IRGO.
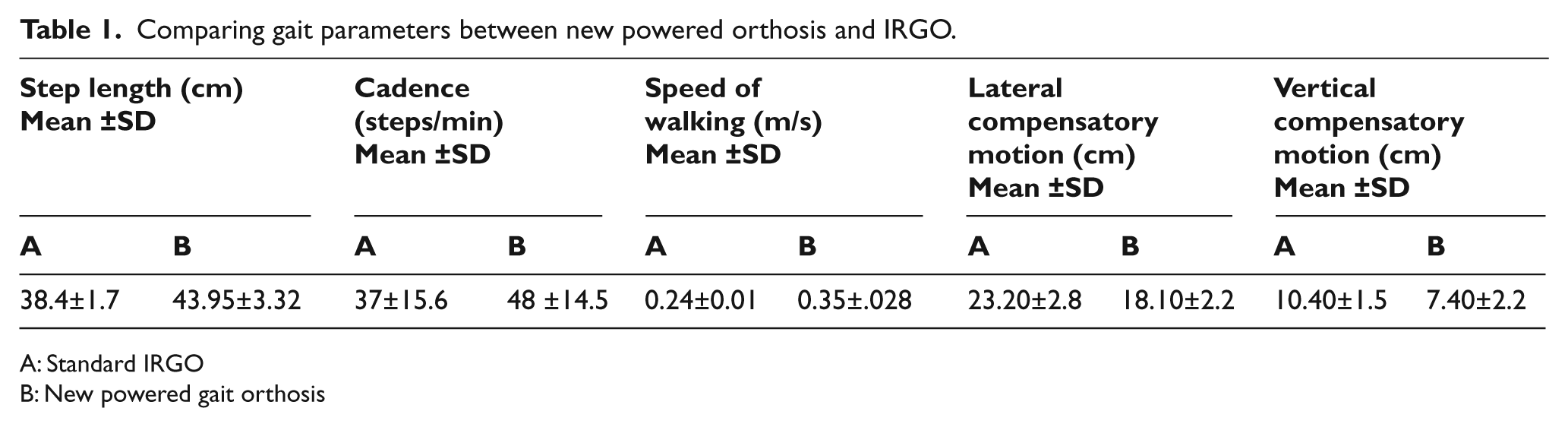
A: Standard IRGO
B: New powered gait orthosis
Table 1 demonstrates the mean and SD of the lateral and vertical compensatory motions in walking with the two types of orthoses. Compensatory motions are required for walking to move the trunk from side to side in SCI individuals. This pattern of gait causes loads to increase on the upper limbs in these patients. Compensatory motions were reduced when the patient walked with the powered gait orthosis as compared to standard IRGO. The amount of compensatory motions was maximally reduced when both actuators worked in synchronization compared to when only one actuator was powered (Table 2).
Mean ±SD of the gait parameters in actuators operations situations.

A: Operation of knee actuator
B: Operation of hip actuator
C: Synchronize operation of actuators
In comparing the resulting effects on step length, cadence and speed of walking when activating the hip or knee actuators in isolation, no substantial differences between these two testing conditions were noted. However, when both actuators were operated in synchronization, substantial differences were observed between the separately and synchronize-activated situations (Table 2). There were no side-specific differences demonstrated when comparing the results from the testing for any of the parameters measured.
Discussion
In this case study, the effects of using a powered and unpowered IRGO on walking were examined and compared in a single spinal cord injury patient. Walking with a powered gait orthosis was proposed to be more effective than a standard IRGO due to the inducement of reciprocal motions in the hips and movement in the knees activated by both actuators. Hip and knee joint angle patterns in this powered orthosis were similar to normal walking patterns when compared to walking with the standard IRGO. The maximum knee flexion and extension were reached at a position of 64% ±2.4 SD of the gait cycle which is comparable to normal walking 25 and maximum hip flexion and extension were reached at 25% ±2.2SD of the gait cycle respectively. In addition, differences were observed between the two orthoses in temporal/spatial parameters.
SCI patients need to produce a large effort and experience high energy consumption rates when walking with mechanical RGOs.12,15 To improve these problems, four electrically motorized actuators were used in the novel orthosis which applied synchronized movements in the hip and knee joints by modifying a standard IRGO. According to these results, the new powered gait orthosis improved walking and reduced vertical and horizontal compensatory motions. In this study, lateral compensatory motion and vertical compensatory motion were defined as the lateral and vertical trunk excursion in the frontal plane during walking; defined as a translatory motion in the global vertical and horizontal axes. Increased lateral trunk motion results in a greater laterally deviated trunk over the limb at midstance. 18 Activation of the actuators in the new orthoses caused active movement in the hip and knee joints, so negating the need for such large compensatory motions. The active movement afforded by the actuators in the hip and knee joints therefore decreased COM displacement.
Walking with new orthosis by the SCI patient showed the knee joint had an extended position during stance and was flexed by the actuators during the swing phase. The hip joints also had flexion and extension patterns similar to normal human walking. The subject did not feel unstable during the walking tests and anecdotaly reported less effort was required to walk, with seemingly reduced loads on upper limb joints. This needs to be investigated in a future study.
The activated joint mechanisms in the new orthosis caused improvement in kinematic parameters as compared to standard IRGO. These results were similar to results presented in previous studies. Ohta et al. demonstrated that activation of knee and hip joint actuators in an orthosis caused the gait speed and the step length to be increased; cosmesis of walking improved and compensatory motions decreased when SCI patients used a powered ARGO. 18 Kang et al. reported that walking with pneumatically- powered gait orthosis reduced gait speed and advantageously altered gait cycle parameters as compared to walking with an RGO. 19 Audu et al. following gait analysis when using a new hip constraint orthosis in healthy subjects announced that the new powered hip orthosis could be suitable for use by paraplegic patients. 26
In considering separating or synchronizing activation of actuators in hip or knee joints two points should be noted. There were no significant differences between separate activation of knee and hip actuators when actuated in isolation, but the speed of walking, step length, cadence compensatory motions and cosmesis of walking improved with synchronized IRGO walking compared to when the powered knee or hip joints were activated separately. The evidence in the literature suggests that activated knee flexion can decrease energy consumption.27,28 Energy consumption was not assessed in this study, but evaluation of the effect of this new orthosis, with bilaterally-powered and actuated hip and knee joints, on the energy cost of walking would be needed in a further study.
For safety reasons, a wheeled walker was used during all tests. This may have produced an influence on the measured values, because the subject needed to reach forwards for stability. However, it was decided to use this device for stability reasons and also in an attempt to potentially reduce the amount of increased mechanical load experienced on upper limb joints during the testing.
Two points are considered in this study. One is the effect of the knee joint actuator on the SCI patient. Studies in this field have reported that active knee flexion causes reduction in energy consumption.27,28 However, Baardman et al. demonstrated opposite results to this, 29 and Green and Grant demonstrated that knee flexion did not decrease compensatory mechanisms in their study. 30 The other point is the effect of the hip joint actuator on the orthotic gait. The results reported in this study were similar to those reported previously in this field.18-19
The patient reported that she felt that the use of both actuators tended to improve her walking performance. She also commented that the assistance afforded by the hip joint actuator had a tendency to reduce the load on upper limb joints. When the knee joint actuator was activated, compensatory motion of the upper part of the body decreased. Synchronized motion of the both actuators anecdotally produced the best effect in reducing walking effort.
A major disadvantage of the powered orthoses for use in paraplegic walking is energy density. Therefore, for a powered orthosis to be portable, the actuators and batteries should be lightweight and should offer many hours of use before needing recharging. In the past, motors utilized in lower limb orthoses have been extremely bulky and the batteries needed a massive backpack. We created a powered gait orthosis with a total weight of only 10.1 kg which we consider to be the lightest weight RGO capable of providing synchronized joint movement to date. The small, powerful and programmable motors used in this new orthosis should prove capable of facilitating the development of a commercially-viable device.
Increasing the patient’s functional abilities is the ultimate aim of a rehabilitation program in SCI patients when they are not using the orthoses. Plasticity of the nervous system occurs by specific re-training of stepping and walking after an incomplete SCI. 31 The useful effect of walking training in SCI patients is well reported. The use of powered gait orthoses as an assistive device could provide repeatable walking training for paraplegic patients to improve functional motor recovery by assisting a patient to train by walking in rehabilitation clinics. Because the new orthosis has synchronized hip and knee joint movements, it could be used for gait rehabilitation in SCI patients. However, before using such an orthosis, individuals with paralyzed muscles should use gait training in a clinical environment to increase muscle endurance.
Conclusion
SCI patients would benefit from needing a lower energy consumption rate and less effort to walk than that currently provided by reciprocal gait-type orthoses due to their lower limb paralysis and reduced endurance levels. To contribute to the satisfaction of these aims, a new powered gait orthosis with synchronized hip and knee joint motions was fabricated using powerful and small electric motors in an IRGO. Gait evaluation of this orthosis with co-activation of both actuators on walking in SCI patients showed improvements in gait speed, step length, cadence and compensatory motions when compared to walking with a standard IRGO. The results suggest that further development of the device is warranted in an extended study to verify the effect on the energy cost of walking and endurance by a group of volunteer SCI subjects with differing levels of injury when walking with the new novel orthosis.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.