
Abstract
Study design
Randomized experimental study.
Objective
Compared to able-bodied people, patients with paraplegia due to thoracic spinal cord injury (SCI) are at an increased risk of heat illnesses during exercise due to impaired thermoregulatory responses. To overcome this limitation, we investigated the performance of three phase change material (PCM) cooling vests of different melting temperatures (Eijsvogels, #49) and coverage area of the trunk.
Methods
Sixteen participants were divided into three groups according to their injury level. All were tested for V20 full vest (20°C Tm, 75% coverage). Mid-thoracic and high-thoracic groups were tested for V14 vest (14°C Tm, 75% coverage). The mid-thoracic group was tested for V20 half vest (20°C Tm, 50% coverage). The participants performed a 30-min arm-crank exercise followed by a recovery period inside a controlled hot climatic chamber. The heart rate, segmental skin (Tskin), and core temperature (Tcore) values were recorded, and subjective questionnaires were taken.
Results
Compared to no vest (NV) test, all the vests showed an effective decrease in Tskin values of the trunk. However, the decrease in Tskin was not enough to induce a significant decrease in Tcore in all three groups. Mid-thoracic and low-thoracic groups showed a reduction in the increasing Tcore by the end of the exercise and recovery period. Finally, the level of thermal comfort was enhanced for the three groups.
Conclusion
The effectiveness of cooling vests for persons with paraplegia is dependent on injury level and thus the ratio of sensate to insensate skin. Future studies necessitate the investigation of the cooling effects of PCM vests at a lower Tm with a larger sample size.
Introduction
Spinal cord injury (SCI) is an insult to the spinal cord that alters its function and can even lead to death, depending on the site of injury. According to the National Spinal Cord Injury Statistical Center (NSCISC), there are 17 810 new cases of SCI yearly, with a total approaching 300 000 cases in the United States (National Spinal Cord Injury Statistical Center, 2020). The causes of SCI are many, but motor vehicle accidents have been in the lead for the past 40 years, followed by falls, crimes and violence, sports injuries, and medical and surgical complications, among others 1 (National Spinal Cord Injury Statistical Center, 2020).
Regardless of the spinal cord injury level, SCI can be classified as either complete or incomplete. According to the American Spinal Injury Association (ASIA), a complete injury refers to the total loss of the sensory and motor functions below the injury level, whereas an incomplete injury refers to the maintenance of certain sensory and/or motor functions below the injury level. SCI may lead to physiological disturbances, the most important of which are the disorders caused by the autonomic nervous system. The loss of the sympathetic nervous system and the compensatory attempt by the parasympathetic one can potentially results in bradycardia, hypotension, thermoregulatory dysfunction, and disruption in the skin blood flow. 2
One of the fundamental homeostatic mechanisms in the body is the regulation of the core body (Tcore) temperature. Under normal conditions, Tcore is 37oC ± 0.5oC, despite any fluctuations in the ambient temperature. A slight deviation from this range may alter the function of the vital organs and disrupt homeostasis. 3 Patients with thoracic SCI, commonly referred to as paraplegia (PA), experience thermoregulatory dysfunction that induces thermal strain due to unsafe elevation in their core body temperature (Tcore). The impaired spinal cord affects the synchronization of the human sympathetic activity resulting in the disruption of the vasomotor (blood vessel vasodilatation/vasoconstriction) and sudomotor (shivering/sweating) responses. Hence, patients with PA are unable to maintain a balanced body temperature below the threshold of thermal strain (37.5°C) due to the loss of the sweating and vasodilatation responses and the vasoconstriction and shivering responses which normally occur when the body temperature is above or below its thermoneutral state, respectively. 4 By this, for the health and well-being of patients with PA, it is of important interest to investigate the performance of phase change material (PCM) cooling vests of different melting temperatures and coverage area of the trunk during exercise in hot conditions to alleviate thermal strain for this population.
Since this group of people cannot maintain their body temperature under thermal stress, physical activity and exercises are considered challenging. The trunk contains the largest share of thermoreceptors for coldness sensitivity and sweat glands, in comparison to other body segments.5,6 Therefore, paraplegic patients cannot balance the heat gain due to the high metabolic rate with the peripheral heat loss since a significant portion of the trunk skin area is insensate.
To prevent the uncontrolled and risky elevations in Tcore, previous studies tested various cooling methods on this vulnerable population. Limited studies investigated the use of phase change materials (PCMs) cooling vests on paraplegic patients. Cooling the sensate skin of the trunk and lowering Tskin values help in increasing the conduction heat transfer from the core to the periphery, thus lowering Tcore values. In the mentioned studies, there were no suitable control groups and the participants performed different types of exercise which may change their effort and thermal response. Most importantly, these studies have not taken into consideration the variations among the participants in terms of injury level while designing the vests. And the injury level is determinant of the altered physiology state and the thermoregulatory dysfunction level.
In the current study, the authors investigated the effect of three PCM vests on patients with paraplegia with SCI during exercise according to their different injury level.
Experimental Methods
Human Subjects
The ethical approval to perform the experiments on human subjects was obtained from the Institutional Review Board (IRB) at the American University of Beirut (AUB) (IRB ID: BIO2018-0401). All participants signed a consent form to participate in the project and publish their data. The spinal cord injury level was obtained from the patient’s medical record, and the severity of the injury whether complete/incomplete was determined by a physical exam performed by a neurosurgeon according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) exam.
In the current project, the participants, with SCI, were divided into three groups according to their thoracic injury level (Figure 1). Group I: participants with T1-T3 SCI (n = 3), group II: participants with T4-T8 SCI (n = 8), and group III: participants with T9-T12 SCI (n = 5). Figure 1 shows the percentage of insensate skin and the impaired region in each group. Schematic representation of the impaired regions of the torso according to the spinal cord injury level.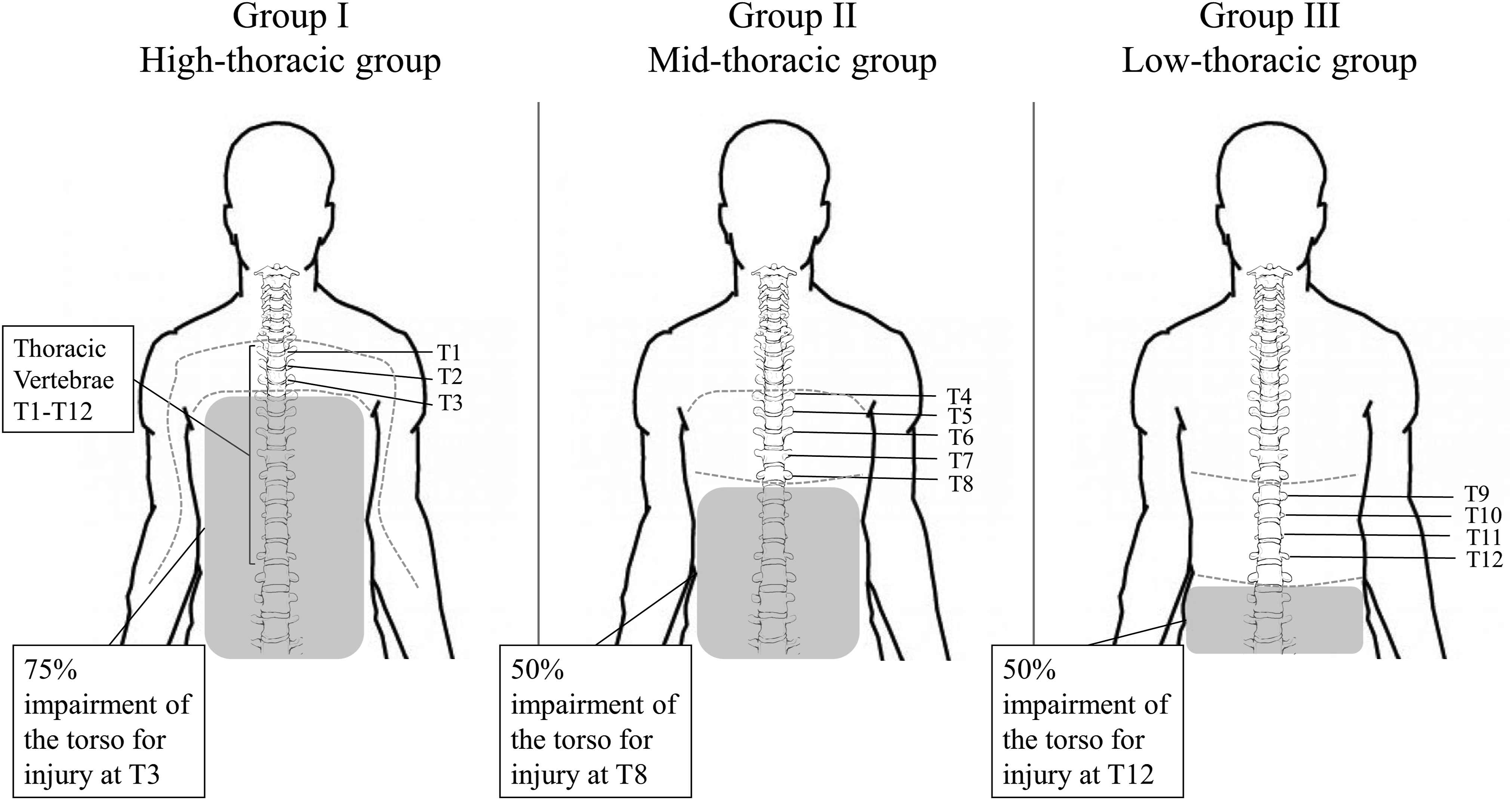
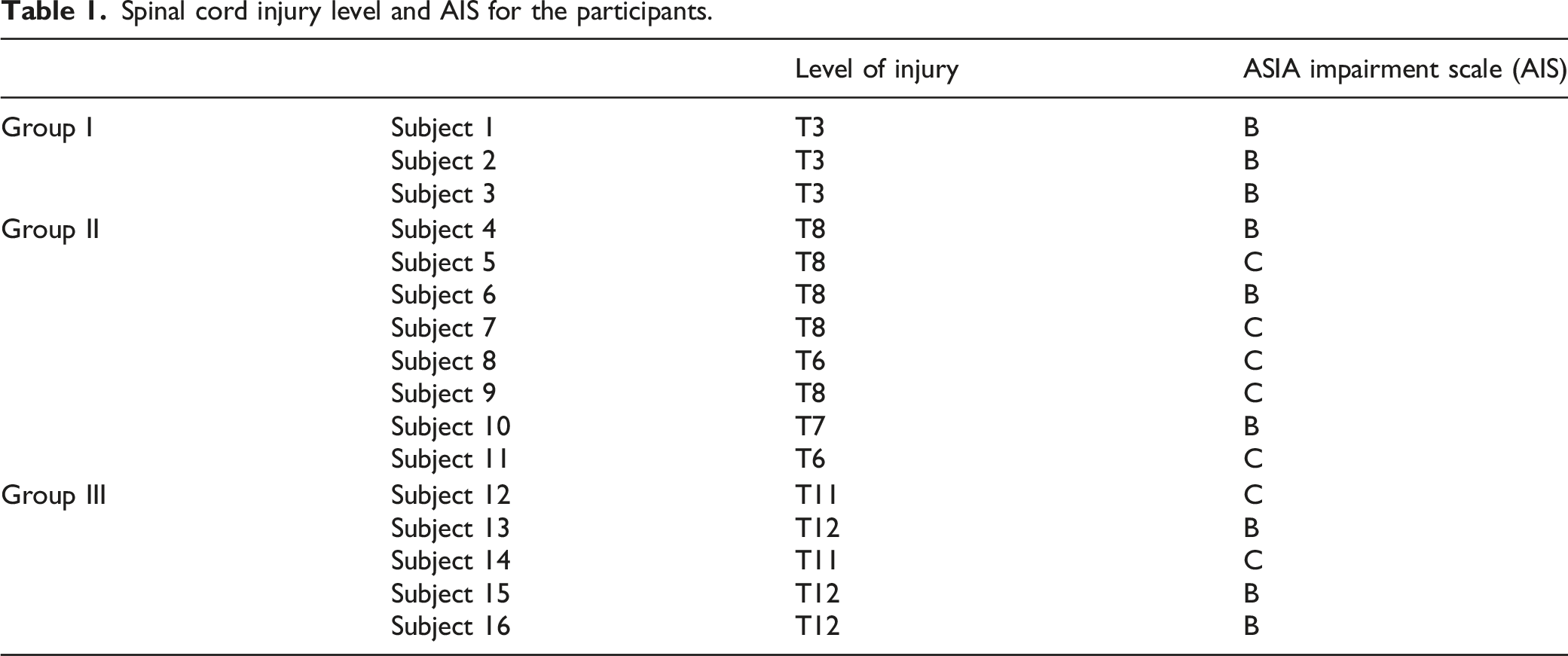
Spinal cord injury level and AIS for the participants.
Physical properties of the participants represented as mean ± SD.

The recruited participants were middle-aged (31 ± 6 years) males and females with thoracic SCI with an average weight and height of 67 ± 11 kg and 171 ± 7 cm, respectively (Tables 1 and 2).
Finally, all participants signed the consent form, committed to a physiotherapy program provided by the recreation center and exercised at least two times per week.
Cooling Vest Characteristics
The polyester cooling vests were commercially designed to hold up to 22 equally sized PCM packets, which were made of a salt mixture of sodium sulfate and water known as Glauber’s salt 7 with a melting point of either 20°C or 14°C.
Two types of PCM vests were used. The first vest of a 20°C melting temperature consisted of two subtypes: V20 full, composed of PCM packets covering the full trunk (chest, upper back, middle back, and abdomen), and V20 half covering half of the trunk (chest and upper back) to target the sensate skin area only (Figure 2), which resulted in lower vest weight. The weight of V20 half and its PCM coverage area of the trunk were both 36% less than in V20 full Schematic representation of the total phase change material coverage at the front and back of the torso for V20 full and V20 half vests.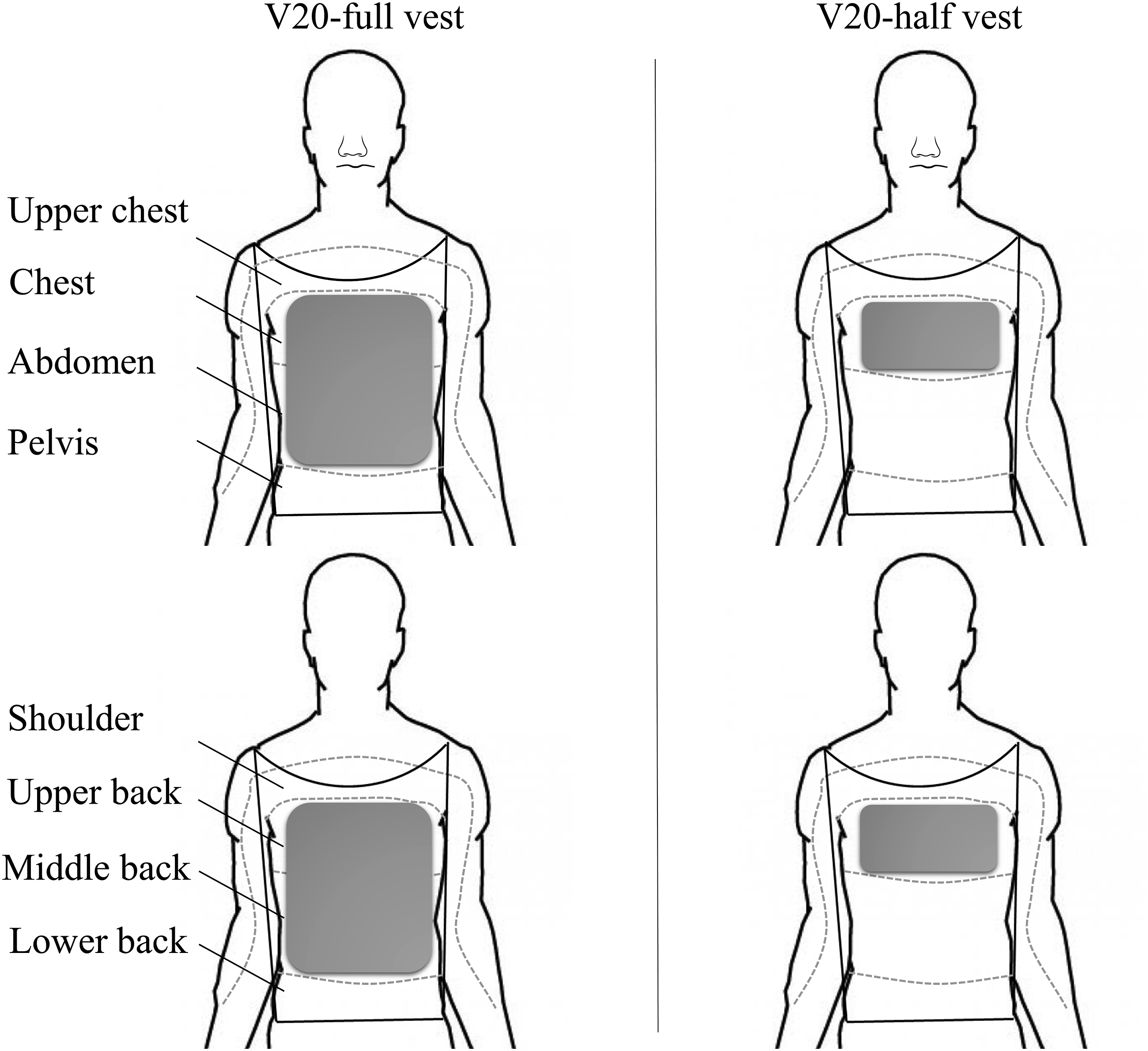
The second vest of a 14°C melting temperature covering the full trunk (V14) included the use of 4 packets of non-toxic carbon-based liquid (Alkane Blend).
Group I: tested with V20 full and V14 full.
Group II: tested with V20 full, V20 half, and V14 full.
Group III: tested with V20 full.
The comparison between V20 full and V20 half is indicative whether cooling the sensate skin only can be as effective as cooling the full trunk. V20 half was tested in the mid-thoracic group only since it is the only group that has variations in the sensate/insensate areas.
Physiological and Physical Measurements
Dry bulb temperature and relative humidity sensor (OM-EL_WIN_USB, OMEGA, UK, .5°C and .5% resolution) measured every 1 min the ambient conditions of the climatic chamber. The accuracy of this sensor is reported to be ±.5°C at typical temperature range (35–80°C) and 3% at typical relative humidity range (20–80%). Temperature iButton sensors (iButton DS19221, Maxim Integrated, CA, USA, .0625°C resolution) were taped on seven body segments at 10 positions (chest, upper back, lower back, pelvis, forehead, forearm, palm, thigh, calf, and foot) and recorded a measurement every 1 min throughout 60-min period of preconditioning, exercise, and post-exercise. The average accuracy of the iButton temperature sensors is .1°C when used at the environmental conditions of (30°C and 50%) with a maximum deviation of .4°C. To ensure proper contact with the skin, a surgical tape was used to place the sensors on the different segments.
Heart rate was recorded every 5 mins using a pulse oximeter (Model 2500A PalmSAT, NONIN, USA, ± 3 bpm accuracy). The values of Tcore were measured in two ways: using an activated ingestible pill and an infrared tympanic thermometer, IRTT. The ingestible pill was configured using e-Celsius Performance Manager software and its monitor (eViewer Perf CE monitor, BodyCap, France) to read every 30 s the gastrointestinal temperature, as an indicator of Tcore. The accuracy of the pill is ±
Subjective questionnaires were explained to the participants and taken every 5 mins during the 30-min exercise period. The whole body and torso thermal sensation, the thermal comfort, the wetness sensation on skin and clothing, and the rating of perceived exertion were evaluated.8-13 The reference scales of the subjective ratings by the participants are summarized in the supplemental table.
The three experimental vests differ in either their melting temperature or their coverage proportion of the trunk. Subjective questionnaires and objective data, including the heart rate and segmental Tskin and Tcore values were taken every 5 mins of the experiment.
The heart rate increased safely during the exercise period (from 15 mins to 45 mins) and then decreased in the recovery period (from 45 mins to 60 mins) and remained relatively stable in each period; besides, none of the patients experienced extreme discomfort.
Experimental Design
All experiments were conducted at the same time in the afternoon inside a climatic chamber. The latter was equipped by a centralized air-conditioning ducted system and contained the arm-crank ergometer (Angio rehab with automatic stand, Lode, the Netherlands). All participants performed arm-crank exercise at constant load of 30 W to limit the variability in metabolic rate generation between subjects of the same group. However, performing the same load of exercise, patients with PA are expected to generate different metabolic rates based on the injury level because the latter affects maximal oxygen uptake as lung capacity is lower in high-thoracic levels.14-16
The climatic chamber conditions were set at hot humid conditions of 30°C room temperature and 50% relative humidity. These conditions were monitored and measured using a temperature and a relative humidity sensor. The reported measurements for all experiments showed a small deviation from set conditions (30.6 ± .1°C and 50 ± 5% humidity). Figure 3 summarizes the detailed steps of the protocol on the day of the experiment. During the 60-min experiment, core and skin temperatures were recorded every 5 mins using the ingestible pill and skin sensors, respectively. Precautions were implemented for stopping the experiment if any of the two conditions occurred to avoid any risk for the participants: (i) the core temperature reaches 38.5°C and/or (Tanabe, #199) if the participant wishes to stop any time during the experiment. Schematic illustration of the experimental design.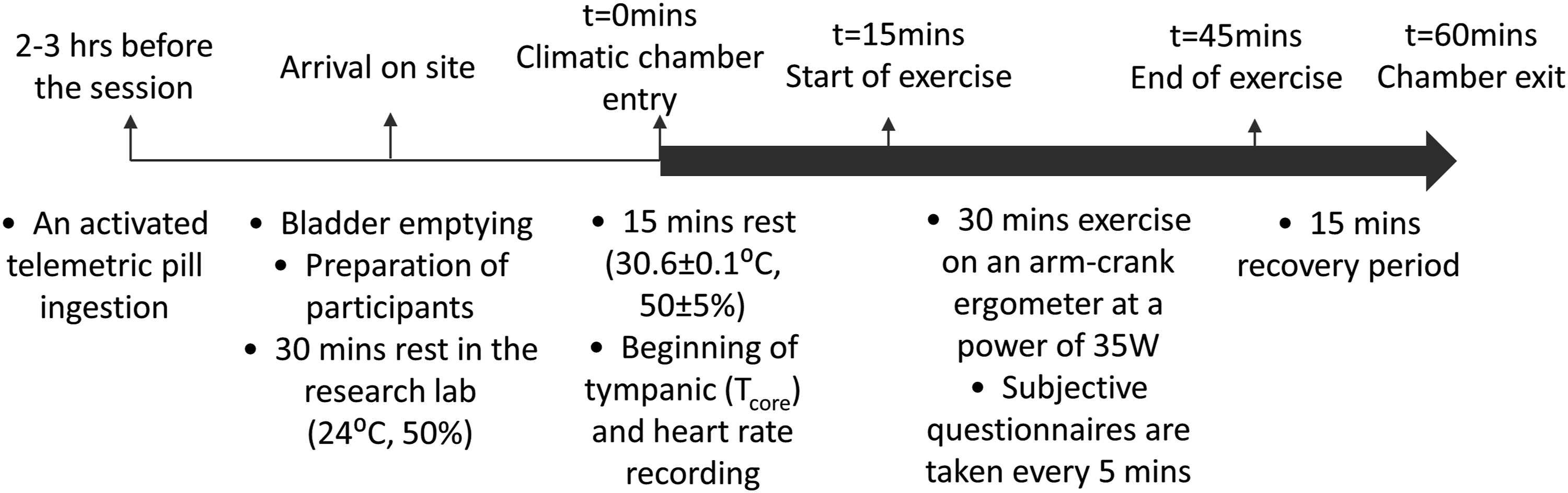
Statistical Analysis
Comparison of the effectiveness of the cooling vest was considered within each group separately due to the variability of metabolic rate among thoracic SCI levels at the same load of arm-crank exercise (30W). Data are presented as ± standard error of the mean (SEM). Statistical analysis was performed by ANOVA and paired-sample t test with significance was set at P-value .05.
Results
The vests described in this article have not been previously tested in patients with paraplegia. To determine the effectiveness of these vests, the participants performed a 30-min arm-crank exercise followed by a 15-min recovery period. Every 5 mins, the skin temperature (Tskin) for the trunk segments (chest, pelvis, upper, and lower back) and the core temperature (Tcore) were measured.
Group I
Figure 4 shows that group I, patients with high-thoracic (T1-T3) SCI, wearing V20 full trunk had a decrease, but did not reach significance, in the segmental Tskin and Tcore. The Tskin at the chest area increased non-significantly in patients wearing V20 full in comparison to the control (NV); however, the Tskin at the pelvis, upper, and lower back for V20 full is lower than that of the control. Nevertheless, even if the segmental Tskin decreased Tcore, it did not reach significance. Graphs showing the variation of the heart rates, segmental Tskin (chest, pelvis, upper, and lower back), and Tcore values as a function of time (mins) for the high-thoracic group (T1-T3) wearing V20 and V14 full trunk. Data are means ± SEM, asterisk indicates P < .05 with respect to the control no vest (NV), *P < .05, **P < .01, ***P < .001.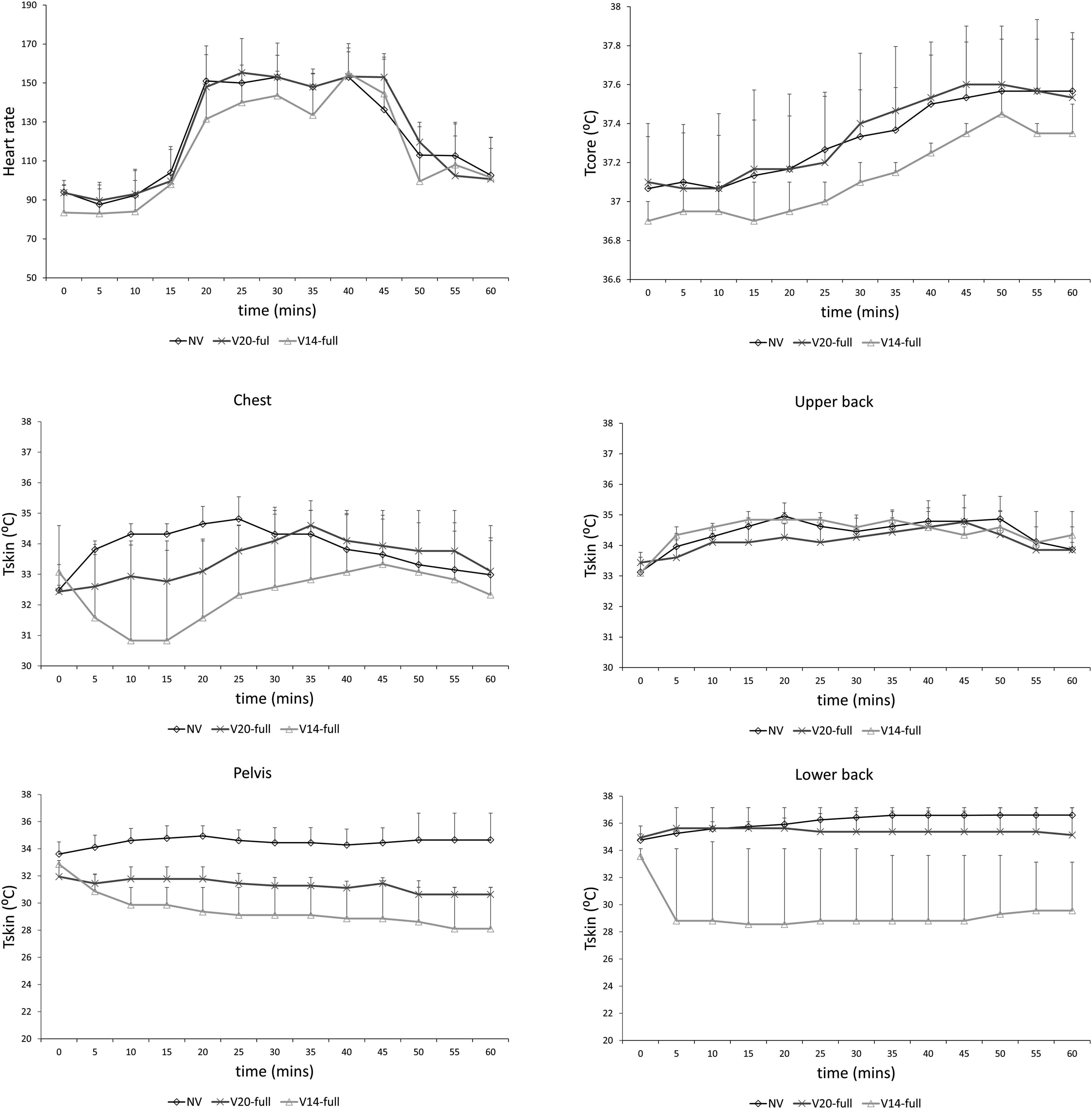
Another PCM cooling vest was developed with lower melting temperature
These objective findings were in concordance with the subjective ones (Supplementary Figure 1). The participants reported improvement in the thermal comfort level from “uncomfortable” with no vest to “slightly uncomfortable” with V20 full and “comfortable” with V14. Similarly, for the whole body and torso thermal sensations, where the impressions changed from “hot” with no vest to “slightly warm” and “neutral” with V20 full and V14, respectively. The vests had a non-significant effect on the perceived exertion and skin wetness.
Group II
Spinal cord injuries at the level of the high- or low-thoracic spine have similar ratios of sensate and insensate skin in the same group, unlike those at the mid-thoracic (T4-T8) level. Therefore, patients in group II were also tested for V20 half trunk, covering the sensate skin only, in comparison to the control NV and V20 full trunk. Surprisingly, V20 half increased Tskin non-significantly in the upper and lower back and pelvic regions, while decreased the temperature non-significantly in the chest region, in comparison to the NV group. At the same time, V20 half group registered the lowest Tcore values in comparison to the NV and V20 full groups. V20 full caused a non-significant decrease in the Tskin at the chest, upper back, and pelvic regions and significant decrease in the insensate skin of the lower back from time 20 mins to 60 mins. This decrease in the temperature in the sensate skin area was not enough to induce a significant decrease in the Tcore (Figure 5), yet Tcore was below the threshold of thermal strain (37.5°C). Graphs showing the variation of the heart rates, segmental Tskin (chest, pelvis, upper, and lower back), and Tcore values as a function of time (mins) for the mid-thoracic group (T4-T8) wearing V20 full trunk and V20 half trunk. Data are means ± SEM, asterisk indicates P < .05 with respect to the control no vest (NV), bar and asterisk indicates P < .05 of V20 half with respect to V20 full, *P < .05, **P < .01, ***P < .001.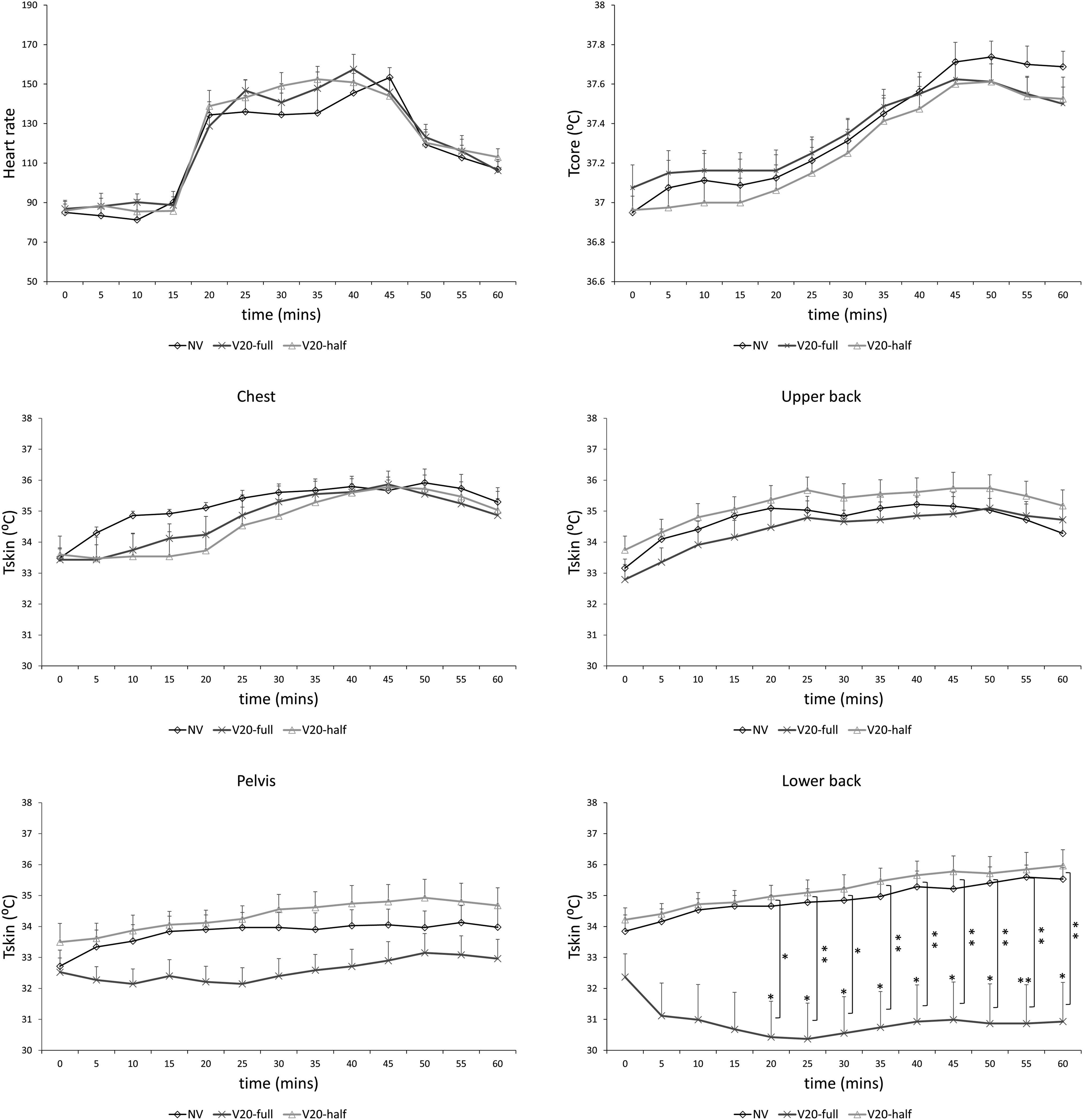
Similar findings were shown with V14 vest. Non-significant decrease in the segmental Tskin and Tcore was registered, yet the change in the Tcore was below the threshold of thermal strain (37.5°C). In addition, V14 caused a more pronounced decrease in the Tcore, in comparison to V20 full trunk in the recovery period (Figure 6). Graphs showing the variation of the heart rates, segmental Tskin (chest, pelvis, upper, and lower back), and Tcore values as a function of time (mins) for the mid-thoracic group (T4-T8) wearing V20 and V14 full trunk. Data are means ± SEM, asterisk indicates P < .05 with respect to the control no vest (NV), *P < .05, **P < .01, ***P < .001.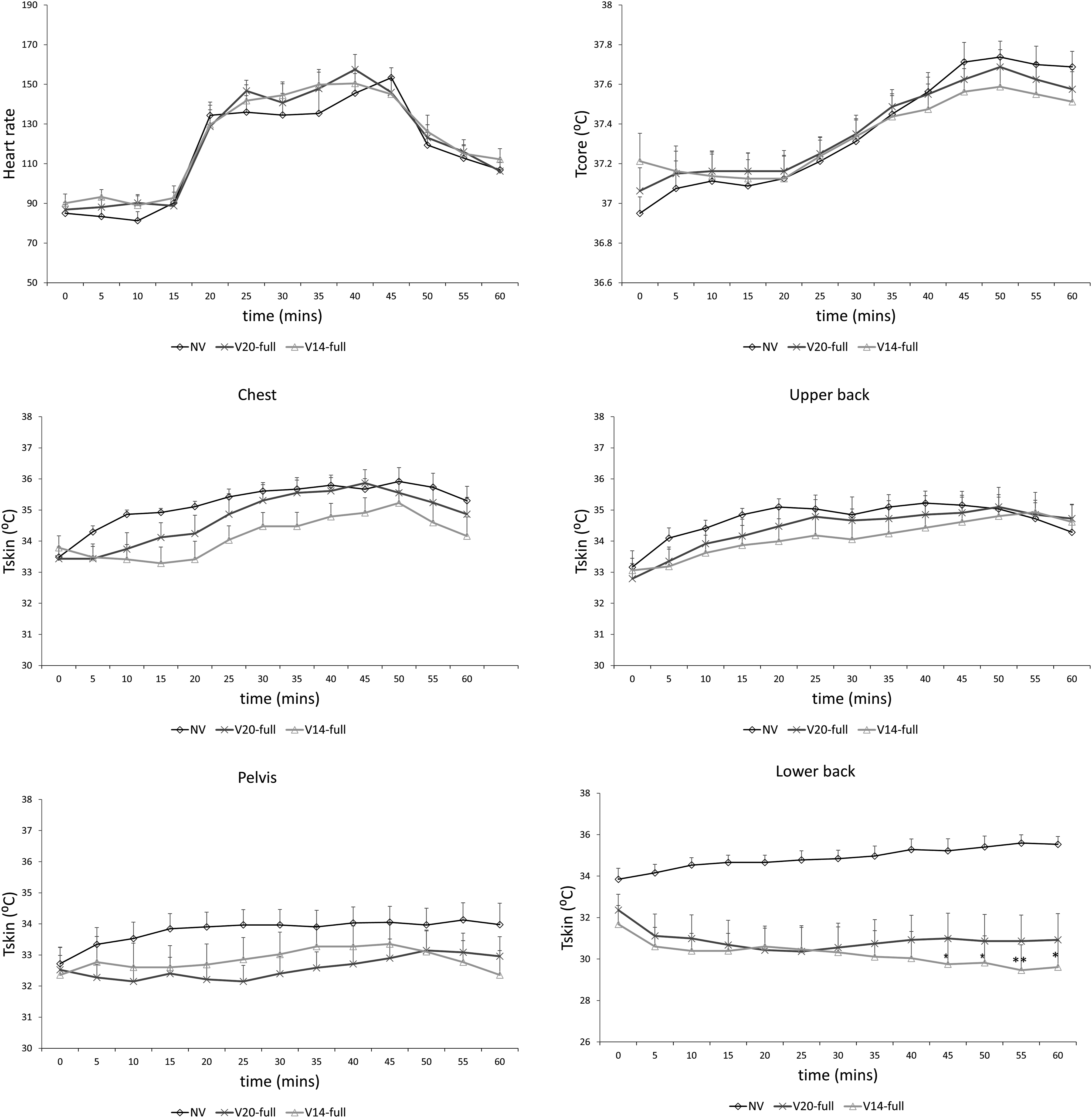
However, the subjective data showed that the participants experienced better thermal sensation and comfort levels upon wearing the vests, especially the V14 vest. Besides, the perceived exertion changed from “hard” with no vest to “fairly light” with V14 (Supplementary Figure 2).
Group III
Like the first two groups, patients with low-thoracic (T9-T12) SCI wearing V20 full trunk showed a non-significant decrease in the Tskin in the sensate areas (chest and upper back) and a significant decrease in the Tskin in the lower back area. These changes were not pronounced to induce a significant decrease in Tcore; however, it is worth mentioning that Δ change in the Tcore in this group is the highest among all groups (Figure 7). Graphs showing the variation of the heart rates, segmental Tskin (chest, pelvis, upper, and lower back), and Tcore values as a function of time (mins) for the low-thoracic group (T9-T12) wearing V20 full trunk. Data are means ± SEM, asterisk indicates P < .05 with respect to the control no vest (NV), *P < .05, **P < .01, ***P < .001.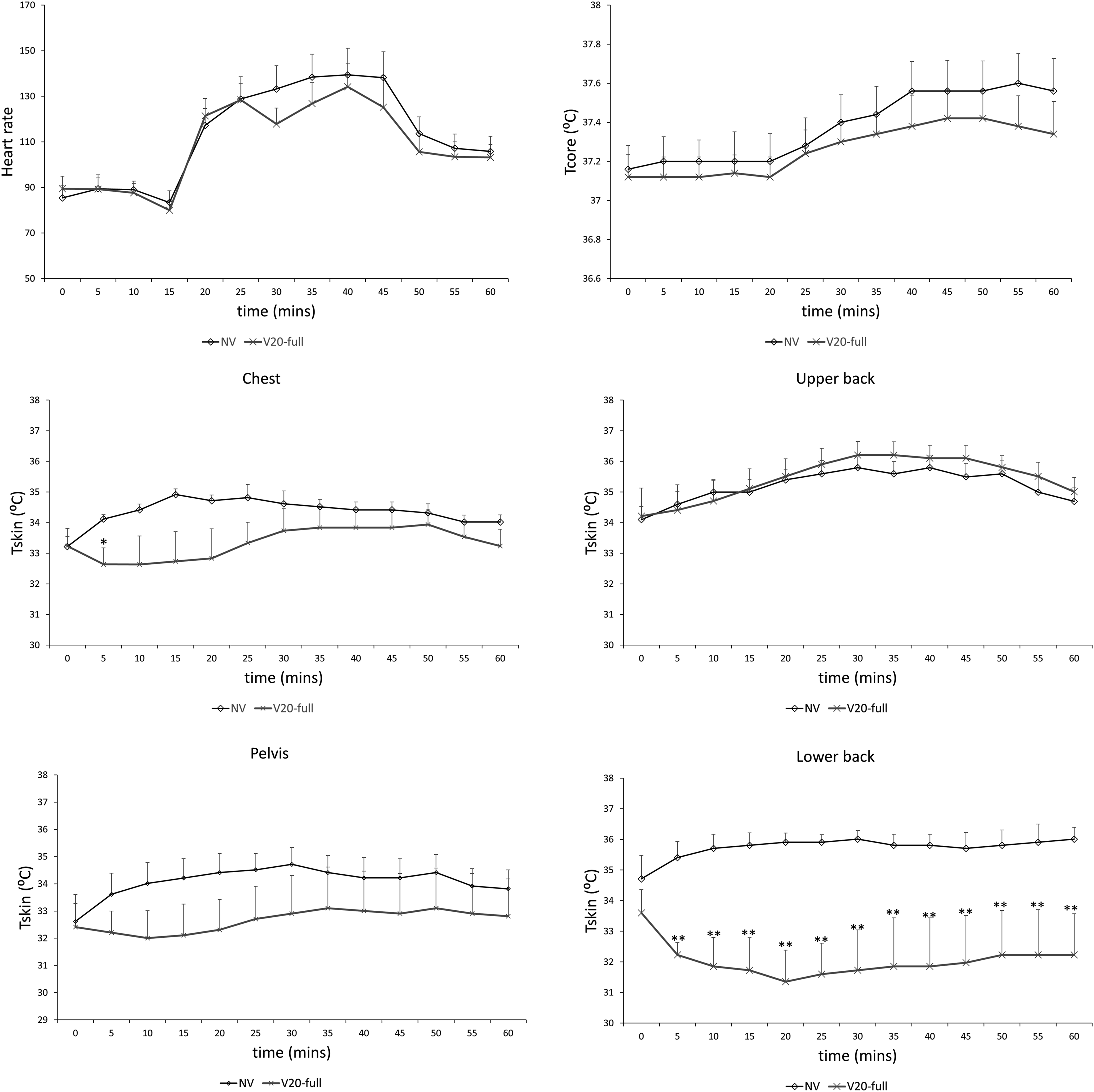
In addition, the torso thermal sensation improved from “uncomfortable” to “neutral” with the vest. The thermal comfort level, perceived exertion, and skin wetness significantly improved in the low-thoracic group upon wearing V20 full, in comparison to the control NV (Supplementary Figure 3)
Discussion
The literature body about the effectiveness of PCM cooling vests for patients with PA is still scarce. This is the first human study that documents the effect of these three PCM cooling vests on the segmental Tskin and Tcore in patients with thoracic spinal cord injury at these melting temperatures (14°C and 20°C) and with such exercise protocol. The overall aim of the study was to investigate the effectiveness of the cooling vests in PA patients during exercise and whether their lowering temperature potential is dependent on the spinal cord injury level.
People with SCI lack the thermoregulatory response mechanism of the body where Tcore changes according to the ambient temperature. This is due to an impaired sweating and vasomotor responses at the insensate skin. 17 The impairment of the homeostatic process is dependent on the injury level and the ratio of insensate skin area to total skin area. The higher the level of the SCI, the more severe the symptoms are. Therefore, significant changes in the temperature in the insensate areas have no effect on the Tcore due to the lack of vasodilation and vasoconstriction and thus the lack of the heat transfer mechanisms. 18 This supports our findings where a significant decrease in the Tskin at the lower back area in the mid- and low-thoracic groups caused a decrease in the Tcore to below the threshold of thermal strain (37.5°C). Moreover, the greatest change in Tcore was shown in the low-thoracic group which has the lowest injury level and the highest ratio of sensate skin among the groups and thus the most preserved thermoregulatory mechanism.
In addition, the subjective and objective findings for V14 were better than that of V20 full trunk in the mid-thoracic group. V14 caused a more pronounced decrease in the segmental Tskin and Tcore values in the resting period, in comparison to V20. Our findings are in accordance with previous studies. Goa et al. found that the cooling rate of the PCM vests depends on the temperature gradient between the subject and the PCM packets. 19 A comparative study on the cooling effect of two PCM vests of different melting temperatures (24°C and 28°C) showed that the vest with the lower melting temperature had a more noticeable effect on the torso and mean Tskin. 20
Limitations
Several factors and limitations may affect the results. The eligible participants who were accepted for participation were all with incomplete injuries (ASIA B or C) as reported by the neurosurgeon who was in charge in examining them. No participant with complete injury participated in this study despite extensive recruitment efforts. This limitation was considered when evaluating the change in core temperature in NV test. The findings for each group showed gradual increase in core temperature as an indication of impaired autonomic system in persons with PA. Findings of change in Tcr values in NV test were like previous studies in literature which recruited participants with complete thoracic injury to perform exercise in hot environmental temperature (>30.0°C).21-24
Besides, the cooling rate of the vests depends on the temperature gradient, melting temperature of the packets, and the covering area of the vest. 19 Besides, the exercise protocols are highly variable in literature in terms of duration, experimental groups, exercise type, and the covered body region which limits the comparative nature among the studies. Future studies necessitate the investigation of the cooling effects of PCM vests at a lower melting temperature with a larger sample size.
Conclusion
The results of this experimental study indicated that all the vests showed better cooling effects in the low-thoracic and mid-thoracic groups, rather than in the high-thoracic one. This indicates that the cooling effect of these vests was dependent on the injury level, where the least effect was shown in group I (high-thoracic) since this group had the highest ratio of insensate skin. However, the decrease in the segmental Tskin values was not enough to induce significant decrease in Tcore values in all the groups. Yet, the subjective findings showed an enhanced comfort level, in comparison to the control no vest group.
Supplemental Material
sj-pdf-1-gsj-10.1177_21925682211049167 – Supplemental Material for Effect of Phase Change Material Cooling Vests on Body Thermoregulation and Thermal Comfort of Patients With Paraplegia: A Human Subject Experimental Study
Supplemental Material, sj-pdf-1-gsj-10.1177_21925682211049167 for Effect of Phase Change Material Cooling Vests on Body Thermoregulation and Thermal Comfort of Patients With Paraplegia: A Human Subject Experimental Study by Charbel K. Moussalem, Farah Mneimneh, Rana Sarieddine, Shadi Bsat, Mohamad N. El Houshiemy, Georges B. Minassian, Nesreen Ghaddar, Kamel Ghali and Ibrahim Omeis in Global Spine Journal
Supplemental Material
sj-tif-1-gsj-10.1177_21925682211049167 – Supplemental Material for Effect of Phase Change Material Cooling Vests on Body Thermoregulation and Thermal Comfort of Patients With Paraplegia: A Human Subject Experimental Study
Supplemental Material, sj-tif-1-gsj-10.1177_21925682211049167 for Effect of Phase Change Material Cooling Vests on Body Thermoregulation and Thermal Comfort of Patients With Paraplegia: A Human Subject Experimental Study by Charbel K. Moussalem, Farah Mneimneh, Rana Sarieddine, Shadi Bsat, Mohamad N. El Houshiemy, Georges B. Minassian, Nesreen Ghaddar, Kamel Ghali and Ibrahim Omeis in Global Spine Journal
Supplemental Material
sj-tif-2-gsj-10.1177_21925682211049167 – Supplemental Material for Effect of Phase Change Material Cooling Vests on Body Thermoregulation and Thermal Comfort of Patients With Paraplegia: A Human Subject Experimental Study
Supplemental Material, sj-tif-2-gsj-10.1177_21925682211049167 for Effect of Phase Change Material Cooling Vests on Body Thermoregulation and Thermal Comfort of Patients With Paraplegia: A Human Subject Experimental Study by Charbel K. Moussalem, Farah Mneimneh, Rana Sarieddine, Shadi Bsat, Mohamad N. El Houshiemy, Georges B. Minassian, Nesreen Ghaddar, Kamel Ghali and Ibrahim Omeis in Global Spine Journal
Supplemental Material
sj-tif-3-gsj-10.1177_21925682211049167 – Supplemental Material for Effect of Phase Change Material Cooling Vests on Body Thermoregulation and Thermal Comfort of Patients With Paraplegia: A Human Subject Experimental Study
Supplemental Material, sj-tif-3-gsj-10.1177_21925682211049167 for Effect of Phase Change Material Cooling Vests on Body Thermoregulation and Thermal Comfort of Patients With Paraplegia: A Human Subject Experimental Study by Charbel K. Moussalem, Farah Mneimneh, Rana Sarieddine, Shadi Bsat, Mohamad N. El Houshiemy, Georges B. Minassian, Nesreen Ghaddar, Kamel Ghali and Ibrahim Omeis in Global Spine Journal
Footnotes
Acknowledgments
This publication was made possible by the Collaborative Research Stimulus grant award 24477-103557 of the American University of Beirut. The findings achieved herein are solely the responsibility of the authors. The authors thank the subjects for their motivation to participate, as well as their complete dedication to the experimental work. Theauthors also thank “Dr Mohammad Khaled Social Foundation”, physiotherapist Dr Iman Baydoun; research assistant Georges Manissian; andNurse Suzzane Seifeddin for their technical assistance during subjectrecruitment and experimental protocol.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.