
Abstract
Background:
It is always a challenge to rehabilitate geriatric amputees to perform self-care skills at home with limited ambulation. A new geriatric foot (with a lower effective foot length) has been specifically designed to reduce residual limb stress and to ease the step completion.
Objectives:
The aim of this study is to evaluate the benefit of a new geriatric foot versus a Solid Ankle Cushion Heel foot for low-activity persons with transtibial amputation.
Study design:
Crossover study.
Methods:
A total of 12 patients were included in this study. Outcome measures: 2-min walking test, Quebec User Evaluation of Satisfaction with Assistive Technology 2.0 questionnaire and pressure socket measurements.
Results:
The geriatric foot allows for greater patient satisfaction. The maximal pressure was significantly lower in the proximal anterior stump area. No statistical differences were obtained from the 2-min walking test.
Conclusion:
A geriatric foot designed with a low effective foot length improves the satisfaction and reduces proximal anterior socket pressures for poor-performing persons with transtibial amputation.
Clinical relevance
The development and evaluation of feet specifically designed for geriatric persons with transtibial amputation could improve their specific requirements and satisfaction.
Keywords
Introduction
In Northern Europe, over 90% of amputations are caused by vascular problems, and 80% of people with a lower limb amputation are aged over 60 years. 1 Although prevalence rates are decreasing, the number of amputations of vascular origin is increasing. 2
Lower walking ability reduces the capacity for everyday life activities and involvement in social activities.3,4 Ageing is a negative factor for the functional level but is not alone predictive.4,5 The achievement of rehabilitation goals is not much lower with geriatric patients (even aged over 80 years) than with younger patients. 6 People with a lower limb amputation aged over 90 years can be successfully fitted. 7
The reliable and inexpensive Solid Ankle Cushion Heel (SACH) foot is the most prescribed foot and is considered to be the most appropriate foot for the population of geriatric patients with limited locomotion.8,9 However, the SACH foot has many disadvantages. In terms of gait, the time between heel strike and foot flat has been observed to be twice as long as a normal gait. 10 The foot almost never remains flat during the stance phase, and the heel rises very early, as soon as the tibia has reached a vertical position. Tibia progression is limited during the unipodal stance phase because of the lack of ankle dorsiflexion. 11 All these disadvantages can partly explain the high energy consumption when walking with a SACH foot.
The literature shows that the Energy Storing and Return (ESAR) feet used by patients with a good mobility level can increase walking speed and reduce energy consumption. ESAR feet provide dorsiflexion of the prosthetic ankle and partly release the energy stored during the stance phase. Thus, it is accepted that active patients benefit from using ESAR feet, but no advantages have been demonstrated for walking for subjects with very low mobility, particularly for vascular amputees. 12
Hansen et al. 13 have introduced an approach for prosthetic foot evaluation based on the ‘Roll Over Shape’ concept. One of the parameters used by Hansen et al. 13 is the effective foot length ratio (EFLR). This ratio is approximately 0.8 for the human foot. For transtibial amputees, the decreased effective foot length leads to a decrease in the external moment of the ankle at the end of the stance phase and increased loading of the contralateral limb at the start of its stance phase. 14
The decreased external moment of the ankle is interesting: a lower ankle moment leads to a lower socket moment. Therefore, we might consider that this lower moment leads to a decrease in the pressures applied by the socket on the stump. However, the increased load on the contralateral limb is a negative parameter for persons with lower limb amputation because this increase may cause an early arthritis of the contralateral limb. Moreover, the risk of a unilateral amputee to have the contralateral leg amputated within 2 years ranges from 15% to 20%. 15 However, it is very important to consider that in slow walking conditions (speed < 0.8 m/s) we do not observe any difference in the load on the contralateral limb regardless of the effective foot length. 14 Moreover, a study performed in 2010 shows that the modification of the effective foot length does not lead to a statistically significant change in the energy consumption for non-vascular amputees. 16 Therefore, the new geriatric foot (NGF) (GERY®; PROTEOR, St Apollinaire, France) has been designed so that its effective length is short in order to reduce the sagittal moment in the ankle, and thus in the socket. This foot is recommended only for a population of low-activity-level amputees (walking speed < 0.8 m/s) to prevent a potential increase in the loading on the contralateral limb. Figure 1 shows a schematic description of the NGF compared to the SACH foot used in this study. The main differences are the shape of the core and the type of foam used.
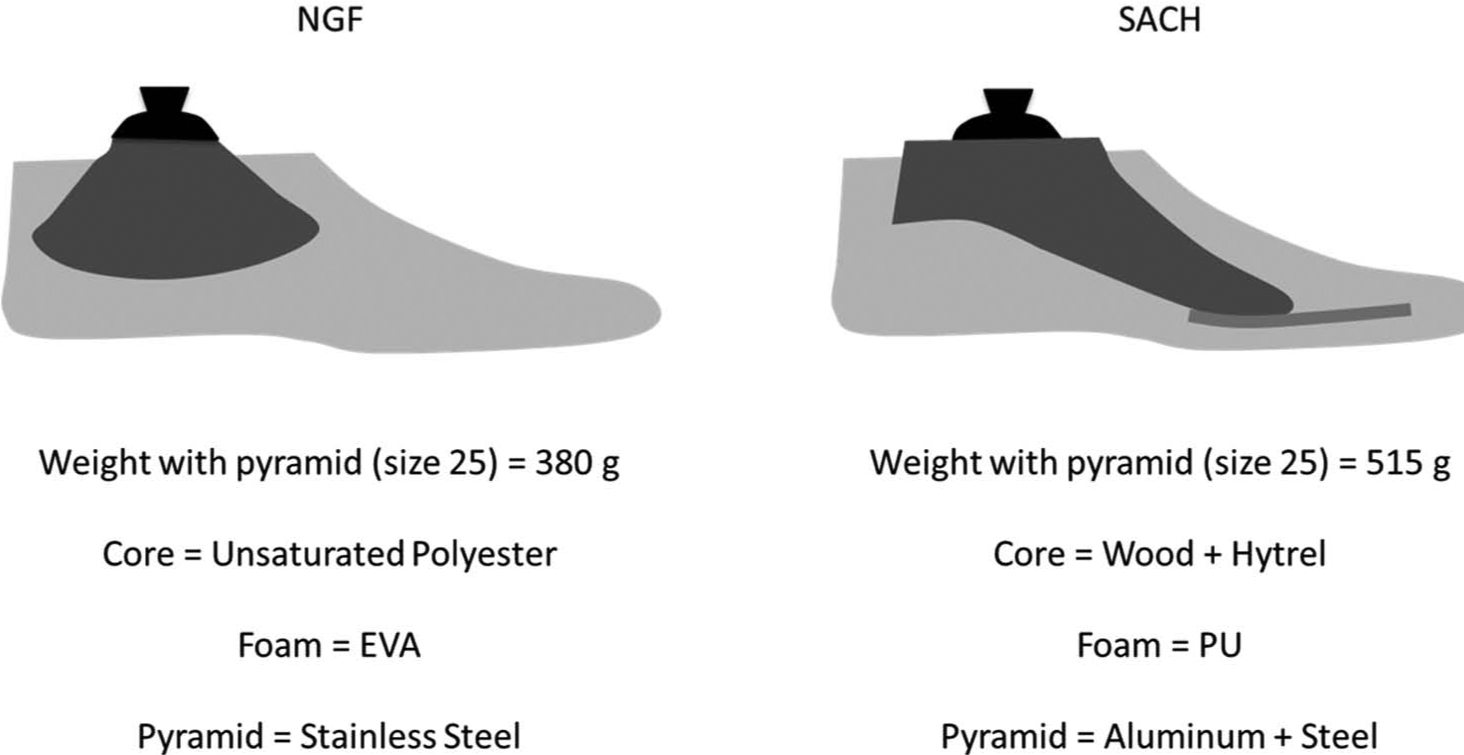
Schematic description of the NGF versus the SACH foot.
The aim of the study is to evaluate an NGF against the SACH foot in poor-performing geriatric people with a lower limb amputation. The main criterion is the satisfaction level of the individuals with a lower limb amputation. The secondary criteria considered the increase in the walking distance and the decreased pressure in the socket.
Methods
Study design and patient selection
The literature reports that patients tend to prefer the prosthetic foot they are used to wearing rather that those required by the study. 10 Therefore, we recruited six transtibial subjects who were initially fitted with a SACH foot (group A) and six transtibial subjects who were initially fitted with the NGF (group B). Both groups changed prosthetic feet at the end of the first test session. The patients subsequently used the foot for 2 weeks until the second test session. To minimize the variations caused by fatigue, each patient will have the second test session at the same time of the day as the first one. The statistical analyses of these differences were made using a Wilcoxon signed-rank test.
All the patients included in this study were recruited at the Centre de Re-education de la Tourmaline (Nantes, France) according to the following criteria:
Transtibial amputees aged over 65 years or subjects fitted with a SACH foot for less than 6 months, with low activity level and able to walk indoors (d4600 according to the International Classification of Functioning, Disability and Health).
The use of these data was made in accordance with both participating institutions and the Declaration of Helsinki which defines ethical principles for medical research involving human subjects.
Evaluation of satisfaction with the prosthesis
The satisfaction with the prosthesis was evaluated using the ESAT questionnaire which is the French version of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) 2.0 questionnaire. 17 This questionnaire is one of the few validated in French for the evaluation of persons with lower limb amputations 18 and includes 8 technical items that evaluate the satisfaction with assistive technology (the prosthetic foot in this study) and 4 items that evaluate the related services.
The ESAT questionnaire is specific for the evaluation of assistive technology and some of the items are not necessarily relevant in evaluating a prosthetic foot. In the second part of the questionnaire, the user is asked to rank the 3 items that he considers as being the most important. The priority items identified by the subjects included in this study were given particular attention.
Evaluation of walking ability
According to Loiret et al., 18 the two main validated tests used to quantify the ability of walking are the timed walking tests and the Timed Up & Go (TUG) test. The 2-Minute Walk Test (2MWT) is quick, reliable and sensitive to changes. Moreover, this measure is correlated to the evaluation of the physical ability of the 36-Item Short-Form Health Survey (SF-36) questionnaire. 19 The 2-min test appears to be the most appropriate version for geriatric patients with a lower limb amputation. 20 This test has been reported in literature with geriatric subjects to compare prosthetic knee components. 21
To our knowledge, the TUG test has not yet been used to compare two medical devices. Moreover, some authors report a ceiling effect for this test 22 and sensitivity to change may be lower than with the 2-min test. 23 Therefore, the 2MWT test was chosen to evaluate the subject walking abilities with the different feet.
Measurement of the pressure in the socket
Peaks of pressure applied to the stump can cause discomfort and even injuries that limit the walking distance and the quality of life. In the literature, pressure in the socket has been reportedly measured with different sensors. 24
The stump areas in which pressure induces pain have been described by Lee et al. 25 As design differences between the NGF and a SACH foot are mainly in the sagittal plane, the pressure was expected to differ in this plane. Thus, pressure sensors were placed at the distal and proximal ends of the anterior and posterior faces of the stump (Figure 2).
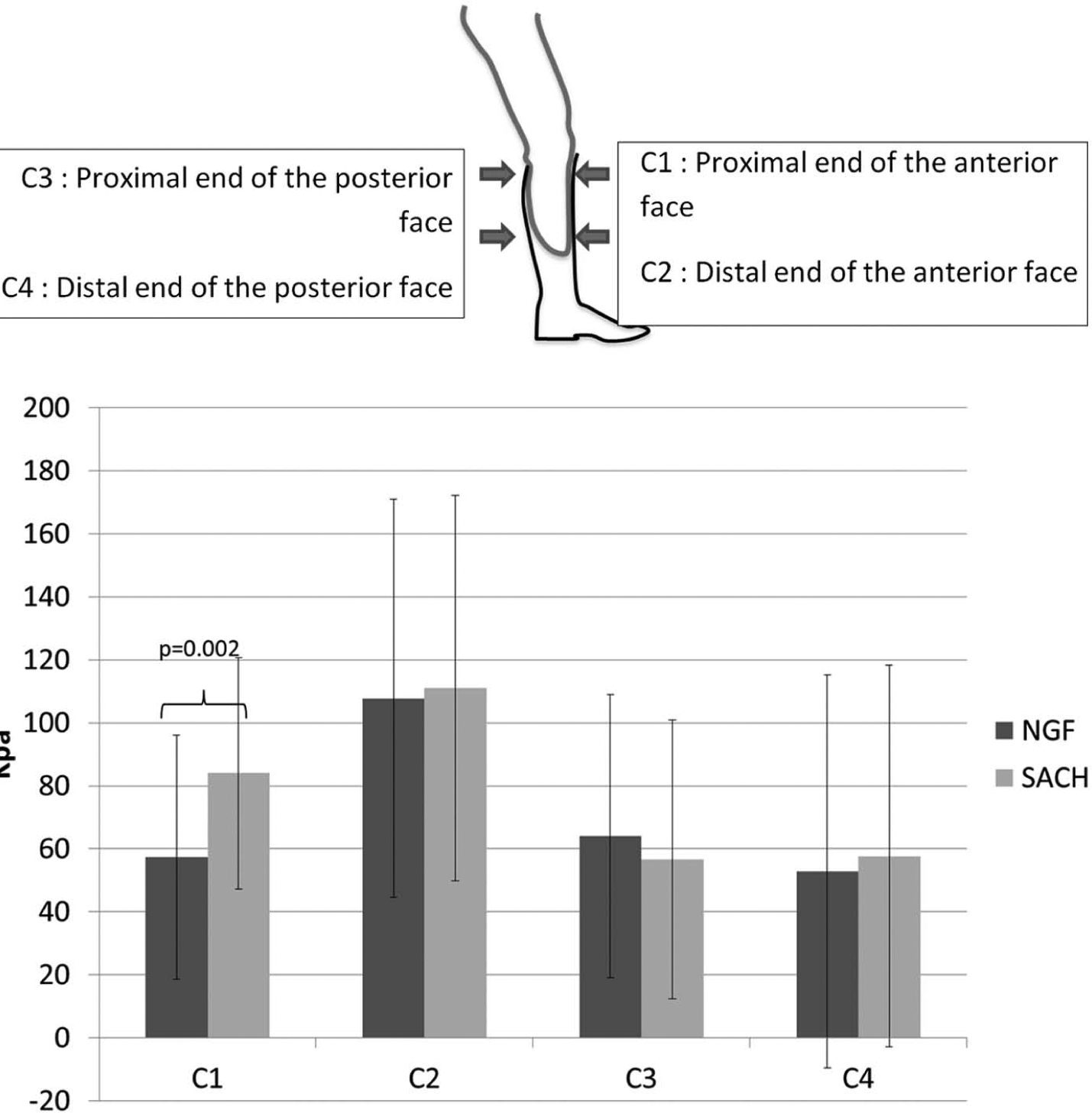
Mean pressure in the socket for transtibial amputees.
The pressure was measured using force-sensing resistor (FSR) sensors that have the advantage of being thin and flexible. However, installing the socket and the sensors may highly affect the measurement reproducibility, and therefore, pressure in the socket was measured at the same time (during the second session, for both the SACH foot and the NGF of groups A and B).
The main evaluation criterion for this study is the global score of the QUEST questionnaire. The scores for each item of the QUEST questionnaire, the distance walked during the 2-min test and the mean pressure measured in the socket are taken as secondary evaluation criteria.
Results
Table 1 shows the features of the 12 patients included in group A and group B. Both groups are similar in terms of age (mean age of group A: 77 years; mean age of group B: 77 years). All the patients use at least one technical aid.
Characteristics of the subjects.
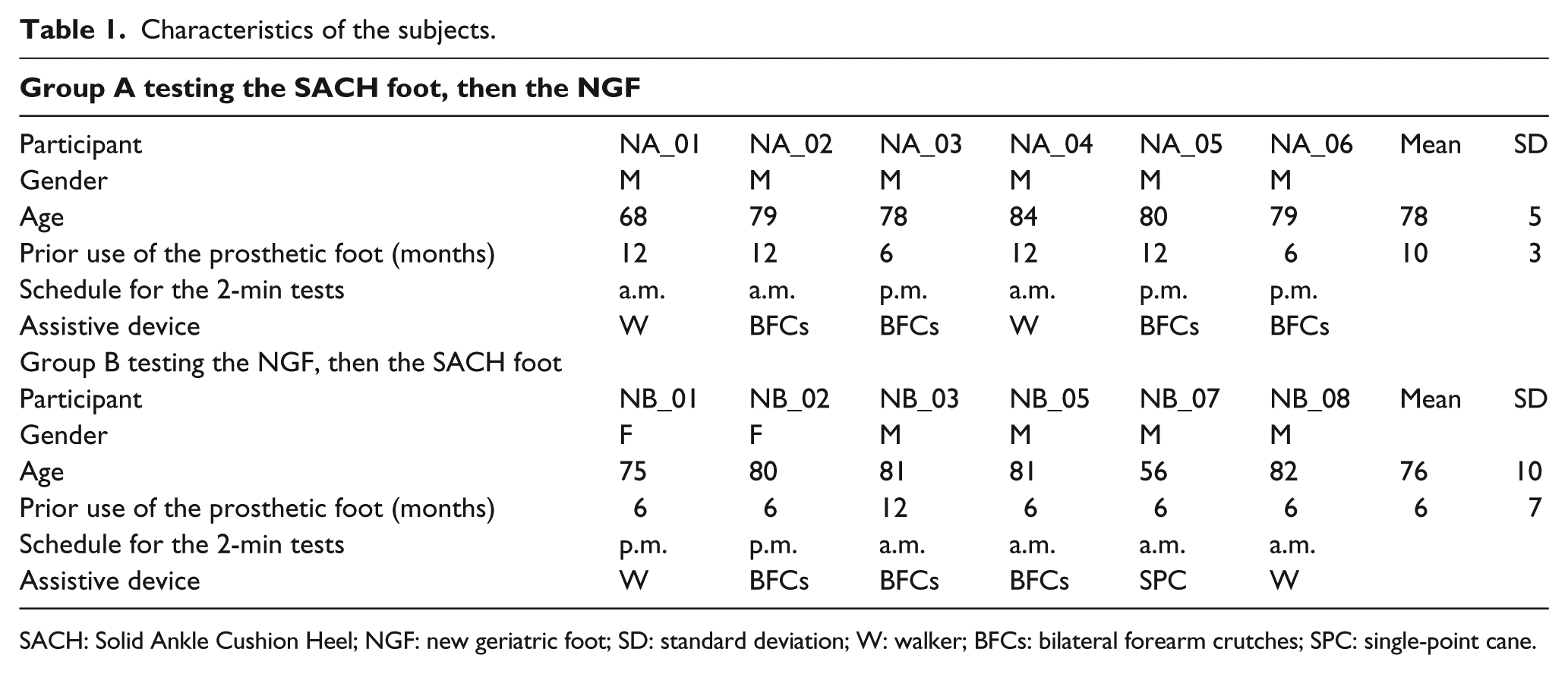
SACH: Solid Ankle Cushion Heel; NGF: new geriatric foot; SD: standard deviation; W: walker; BFCs: bilateral forearm crutches; SPC: single-point cane.
Table 2 shows the mean satisfaction level for the global score and for each item of the QUEST questionnaire.
Comparison of the satisfaction levels of the SACH foot and the NGF.
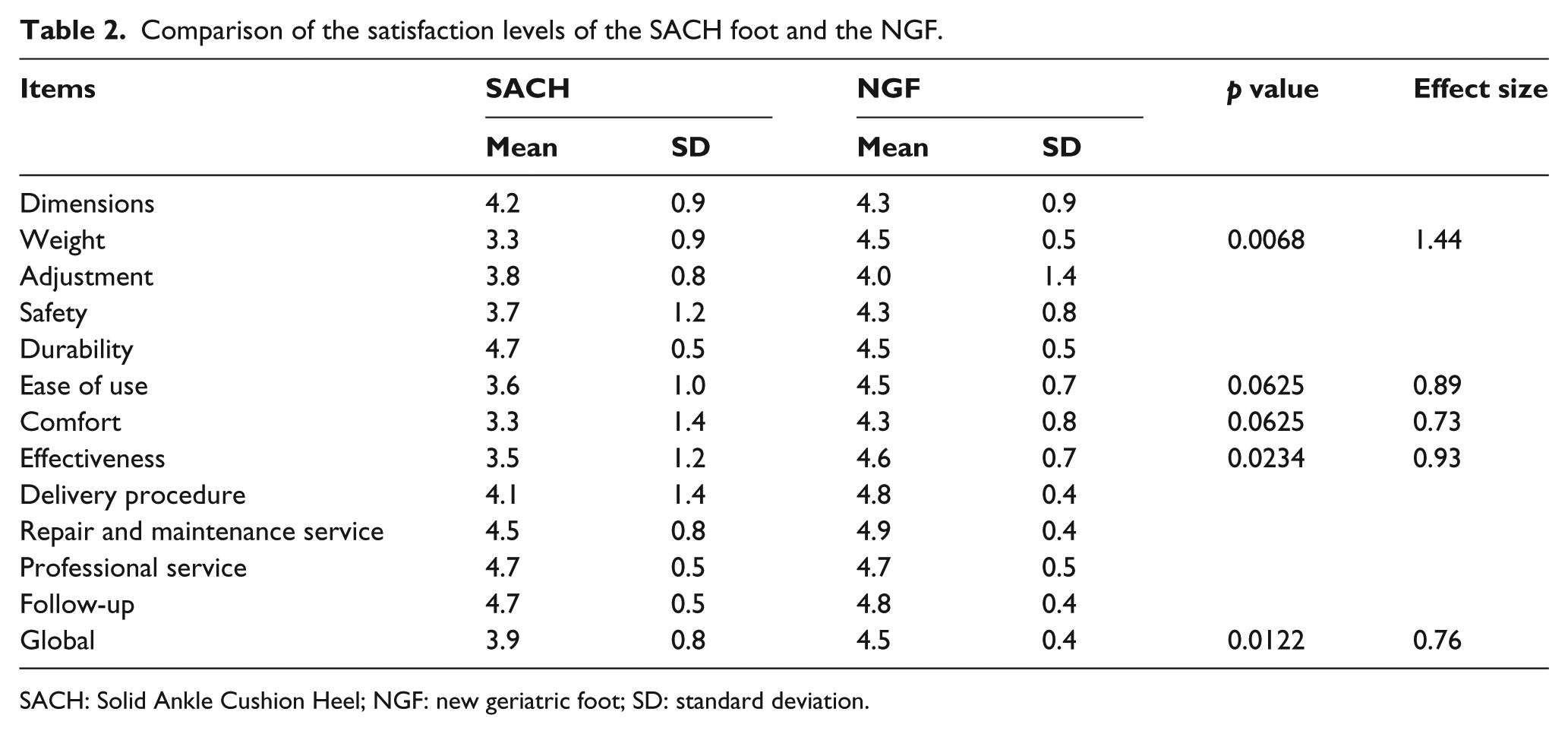
SACH: Solid Ankle Cushion Heel; NGF: new geriatric foot; SD: standard deviation.
The score of global satisfaction of the QUEST questionnaire is higher with the NGF than with the SACH foot (SACH: 3.9, NGF: 4.5; p < 0.002). On average, the satisfaction level is higher with the NGF for all items, except for ‘durability’. However, these differences are significant only for ‘weight’, ‘effectiveness’ and ‘global’ score. For items with a p value below 0.1, the effect size is indicated in Table 2. The following items were assessed as priority items by the subjects of the study:
Priority when using a SACH foot:
Weight Comfort and safety (equal)
Priority when using an NGF:
Comfort Safety Weight
Table 3 shows the distances walked by each group for their two walking tests P1 and P2.
Comparison of the distance walked during the 2-min test with the SACH foot and the NGF.

SACH: Solid Ankle Cushion Heel; NGF: new geriatric foot; SD: standard deviation.
The average distance walked with the NGF amounts to 62.9 versus 60 m with the SACH foot, but this difference is not statistically significant.
The pressure was measured continuously during stance phase. The pressure peaks appeared for C2 (distal area of the anterior face of the stump) and C3 (proximal area of the posterior face of the stump) during the first double support and for C1 (proximal area of the anterior face of the stump) and C4 (distal area of the posterior face of the stump) at the end of the unipodal stance phase. The pressure peaks were extracted and averaged for each subject. Pressure peaks measured in the socket are significantly reduced in C1 (in the proximal area of the anterior face of the stump). The differences in the other areas are minor and not significant.
Discussion
This comparative study includes 12 individuals with a transtibial amputation for vascular disease. The limited mobility of each patient has been confirmed by the walking distance during the 2-min test (lower than 60 m on average). All the patients had used at least one technical aid and they used a SACH foot or an NGF for 6–12 months. The use of technical aids is not homogeneous in the two groups, but we can consider that this selection bias is moderate because of the crossover design of the study.
Satisfaction questionnaire
Comfort, safety and weight are the 3 technical items considered by the patients as being the most important criteria to evaluate their prosthetic foot. The satisfaction level for these 3 items is higher with the NGF. The difference is statistically significant for weight. The use of the QUEST questionnaire is interesting because it shows the specificity of geriatric persons with lower limb amputation. The patients rate comfort, safety and weight as more important than effectiveness. These results could not be extrapolated to other persons with non-vascular lower limb amputation. 26
Walking test
The average distance walked with the NGF was 62.9 versus 60 m with the SACH foot. This difference is not statistically significant. Of the 12 patients included in the study, 11 increased the distance walked in their second walking test compared to the first test. However, this could be explained by the involvement of patients to perform the tests and their desire to do their best. The baseline is higher for group B than for group A, whereas the prior use of a prosthetic foot and the rehabilitation before entering the study were similar for both groups. The walking distances of this study are of the same order of magnitude as those in Devlin et al.’s 21 study (54 m in 2 min).
Pressure in the socket
The pressure levels measured in this study are comparable to those reported in the literature. 27 However, the average values tend to be lower. This observation can be explained by the selection of seniors with low walking speed using technical aids which allow them to unload their stump. These peaks of pressure can cause discomfort and injuries that limit the walking distance of persons with a lower limb amputation.
The NGF has allowed a statistically significant decrease (p < 0.05) in proximal anterior socket pressure. The distal anterior socket pressure shows minor and non-significant differences. This pressure peak occurs at heel strike. This result is normal as the SACH foot and the NGF demonstrate no functional difference in the heel area.
Differences were not revealed on the posterior face of the stump. A higher volume of soft tissues flattening pressure peaks can explain this result. According to the study of Neumann et al., 28 the pressure in C1 is highly correlated to the sagittal moment, and the pressures in C2, C3 and C4 are more correlated to the axial force in the pylon. The lower effective length leads to a lower ankle moment, 14 which reduces the pressure in the socket. The average walking speed of subjects is lower than 0.8 m/s (Table 3). At this walking speed, a shorter effective length does not cause an increase in the loading of the contralateral limb. 14
Conclusion
An NGF was designed with a reduced effective foot length. This NGF was evaluated against the SACH foot with geriatric person with transtibial amputations.
The cross comparison of the two groups demonstrates a higher satisfaction level when using the NGF. This increase is significant for the global score of the QUEST questionnaire (main criteria of this study) and the item ‘weight’ (p < 0.05). The 2MWT revealed no statistically significant difference. Moreover, the improved satisfaction level regarding comfort may be explained by the significant reduction (p < 0.05) of the pressure peak on the proximal area of the anterior face of the stump.
Footnotes
Conflict of interest
Xavier Bonnet works for the research department of PROTEOR. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.