
Abstract
Background:
Walking in high heels presents biomechanical challenges, yet they remain part of many women’s attire. However, women with a lower limb amputation are limited in available footwear options.
Case description and methods:
This case study is in response to one patient’s assertion that she walked better and more symmetrically in heels than flat shoes with her below-knee prosthesis. She underwent gait analysis in athletic shoes and 10-cm stiletto high heels worn with a pediatric running foot to determine if these claims could be substantiated through biomechanical measures. Global gait asymmetry indices were calculated.
Findings and outcomes:
Asymmetry indices were nearly identical between athletic shoes and heels but joint-level findings differed substantially. Ankle mechanics were more symmetrical in heels but hip mechanics were less.
Conclusion:
The maintenance of symmetry in stiletto high heels does not imply maintenance of gait quality, as high heels are known to adversely affect some components walking mechanics.
Clinical relevance
Returning to high-heel wear is achievable for prosthesis users. Accommodations can be made using creativity in prosthetic foot selection to enable successful ambulation; however, attention to gait mechanics may be important for patient safety.
Background
Walking in high heels can be challenging. High heels introduce several negative effects on gait mechanics,1–6 and a biomechanical analysis suggests that heels should be avoided altogether. 7 However, this recommendation may be unrealistic given that heels remain part of many women’s attire. It is important to have the choice and autonomy to be able to wear shoes that are appropriate and/or adequate for a given event, but this choice can be particularly difficult for prosthesis users. For example, some prosthesis users may find professional employment difficult because only athletic shoes can accommodate their prosthetic foot. 8 Others report the desire for adjustable feet to wear heels of different heights with different clothing options. 9 Aesthetics are also an important consideration, and dissatisfaction with prosthetic fit and appearance is more common in female prosthesis users than males.10,11
Women generally have a far wider variety of footwear options than men, including high-heeled footwear. A typical biological ankle can plantar flex to adjust to different heights, but few prosthetic feet can accommodate more than a modest rise in heel height. Some prosthetic companies recently introduced energy-storing-and-returning feet that can be used with heels (e.g. Runway®, Freedom Innovations, LLC; Elation®, Össur; and Accent®, College Park, Inc.). However, none exceed a 5-cm rise. This limitation restricts the available options for most women using lower limb prostheses. A survey by the American Podiatric Medical Association 12 in 2003 reported that 62% of able-bodied women wear heels over 5 cm. For prosthesis users to achieve these higher heel heights, SACH feet are available for a pre-determined heel rise. However, these designs are not adjustable for different heel heights.
The subject in this study had a goal of returning to walking in heel heights of 10 cm and higher. Unfortunately, None of her prostheses at the time could accommodate her desired choice of high-heeled footwear. After a custom prosthesis was made to fulfill her goal, she reported that she perceived walking more symmetrically in high heels than in flat shoes. Anecdotally, other female prosthesis users have made similar statements. The authors determined that a direct comparison of high heels and flat shoes was warranted to determine whether these statements could be supported via biomechanical measures. Specifically, the aim of this case study was to determine how gait mechanics and gait symmetry changed in a female below-knee prosthesis user when wearing high heels compared to flat shoes.
Case description and methods
The subject was a 29-year-old female (height: 1.55 m, mass: 46.8 kg), K4 level ambulator, with a traumatic trans-tibial amputation on the left side. The specific occasion to which she wished to wear high-heeled footwear was a military banquet that required formal attire, and dresses owned by the subject were at lengths most appropriate to be worn with high heels. The subject has agreed to publication of these details in this case report. Platform stiletto high heels with a 10.16-cm heel rise were selected by the subject for this occasion (Figure 1). A variety of different prosthetic feet were considered to accommodate the desired heel height and options included a SACH foot, a swimming foot, and several pediatric feet. Ultimately, the subject and her prosthetist determined that a pediatric running foot would best suit her needs by accommodating the heel rise she desired. Crepe was used to build up the heel and toe regions to fit within the shoe. For comparison purposes, athletic shoes with no heel rise (Adidas Samba) in combination with an energy-storing-and-returning prosthetic foot (Talux, Össur) were analyzed.

A pediatric running foot (Flex Run, Össur) modified to be used with 10-cm stiletto high heels.
A 26-camera motion capture system (120 Hz, Motion Analysis Corp., Santa Rosa, CA, USA) tracked three-dimensional (3D) motions of 57 reflective markers secured to anatomical landmarks and body segments. 13 Five centrally located force platforms (1200 Hz, AMTI, Inc., Watertown, MA, USA) in tandem along the walkway recorded 3D ground reaction forces. A digitization pointer was used to identify 20 anatomical landmarks in relation to marker clusters (C-Motion, Inc., Germantown, MD, USA).
The subject walked in both footwear conditions at a self-selected speed and at standardized speed of 1.1 m/s. Successful trials were identified as those in which the foot made complete contact with one of the force platforms and, in the standardized speed trials, speed fell within a ±5% range of the target speed. Five successful trials on each leg in each footwear condition were analyzed.
Using Visual3D software (C-Motion, Inc., Germantown, MD, USA), marker data were interpolated using a cubic spline and filtered with a Butterworth low-pass filter at 6 Hz; ground reaction force data were low-pass filtered at 50 Hz. A 13-segment full-body model was created. The 3D ankle, knee and hip joint angles, and pelvis and trunk segment angles were calculated. Ankle joint powers were calculated and scaled to body mass. All biomechanical data were normalized to 101 data points across the stride.
Temporal–spatial variables including step length and step, stance, and swing times were computed and symmetry was assessed using an Asymmetry Index (ASI) with the equation
where XRight is a metric from the right side and XLeft is the same metric from the left side at the controlled speed.
Sagittal plane ankle, knee, hip, pelvis, and trunk angles were incorporated into a Global Gait Asymmetry (GGA) score 14 at the controlled speed. The GGA accounts for asymmetries across every point in the gait cycle and weights asymmetries across the joints and segments equally. Greater GGA and ASI scores indicate greater left-right asymmetry. Peak kinematic values were identified, averaged, and compared between footwear conditions.
Findings and outcomes
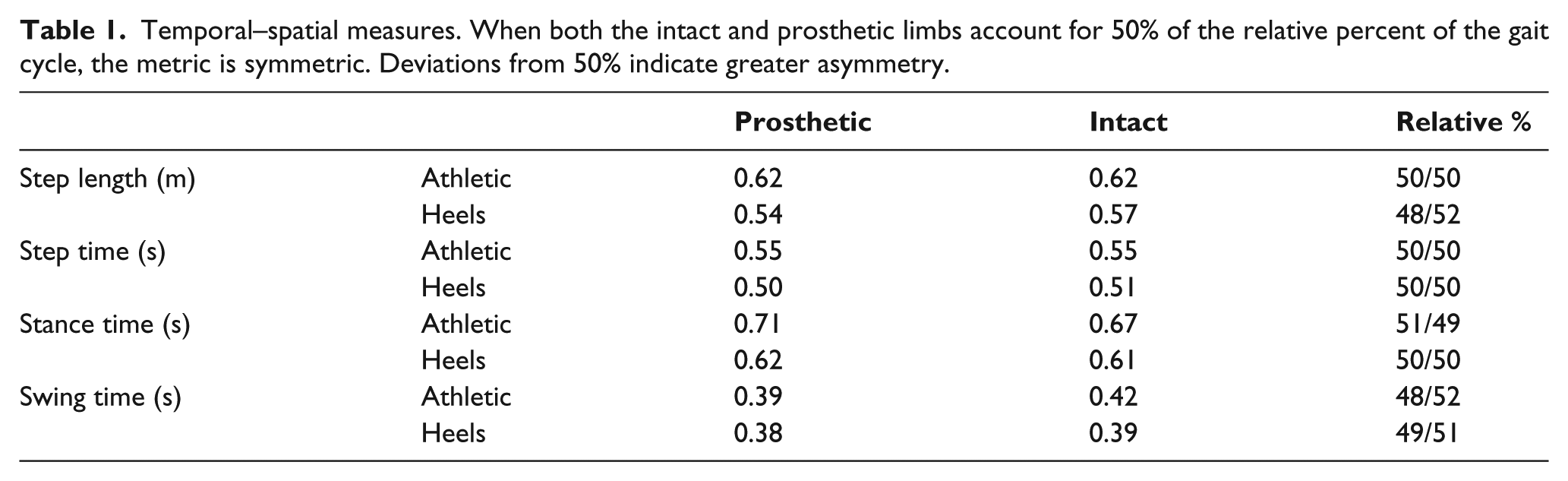
The self-selected walking speed was 27% slower in 10 cm heels (0.84 m/s) compared to athletic shoes (1.15 m/s). Step lengths were more asymmetric in heels (longer on prosthetic side), but stance and swing times were more symmetric than athletic shoes (Table 1). Overall gait symmetry, assessed via cumulative GGA scores, was only 2% different between athletic shoes and high heels (Figure 2).
Temporal–spatial measures. When both the intact and prosthetic limbs account for 50% of the relative percent of the gait cycle, the metric is symmetric. Deviations from 50% indicate greater asymmetry.
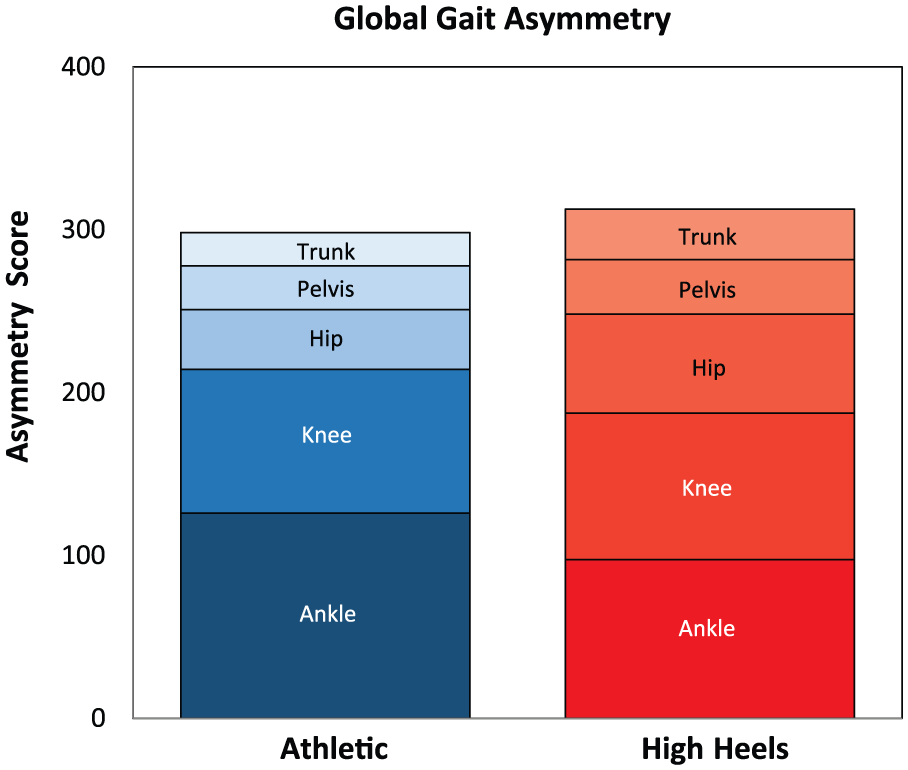
Gait asymmetry across the lower limbs when using different shoes. Greater values indicate greater left–right asymmetry.
Ankle
GGA scores in both footwear conditions were greatest at the ankle and progressively decreased at each analysis of a more proximal joint or segment. In the athletic shoes, the asymmetries at the ankle accounted for 42% of the overall asymmetry, whereas the ankle accounted for only 31% of the overall asymmetries in high heels. High heels positioned the foot in a plantar flexed position and reduced ankle range of motion 37% on the prosthetic side and 27% on the intact side relative to athletic shoes (Figure 3).
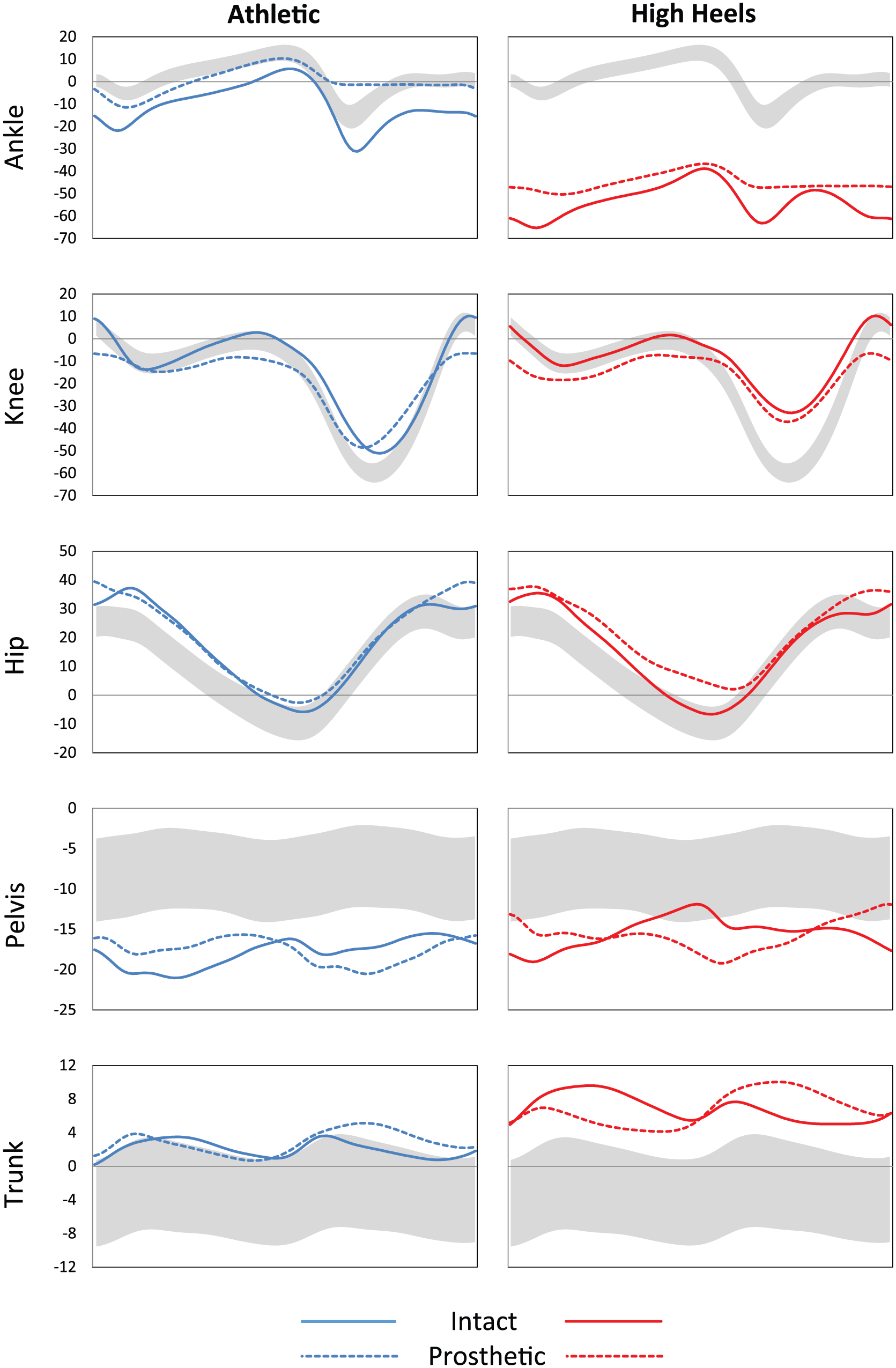
Joint and segment kinematics across the gait cycle when walking at a standardized speed of 1.1 m/s. Solid lines represent the intact limb, dashed lines represent the prosthetic limb, and gray shaded areas represent a normative reference range from 54 able-bodied subjects.
Knee
GGA scores at the knee were consistent between conditions and accounted for 30% of the asymmetry in the athletic shoes and 29% of the asymmetry in the high heels. Peak knee flexion was only 8% less on the prosthetic limb than the intact limb in athletic shoes but was 53% greater in heels. Peak knee flexion during early-mid stance in heels relative to athletic shoes was 24% greater on the prosthetic limb but 12% less on the intact limb.
Hip
Asymmetries in hip angles contributed to 12% of the total GGA score in athletic shoes and to 19% in heels. Together the hip, pelvis, and trunk asymmetries accounted for 28% of the overall asymmetry in athletic shoes and 40% in high heels. Peak hip flexion was 7% greater on the prosthetic limb than the intact limb in both footwear. Hip extension was similar between limbs in the athletic shoes but was 11% less on the prosthetic limb in high heels. Hip extension fell within the normative reference range on the intact side in both footwear conditions but was less on the prosthetic side in high heels.
Pelvis
Asymmetries in pelvic segment motion between left and right steps accounted for 9% of the GGA score in athletic shoes and 11% in high heels. Overall, anterior pelvic tilt was more pronounced in the patient than in the normative reference range. The asymmetry was greater in the high-heeled footwear condition as peak posterior tilt occurred during mid stance in the high heels and peak anterior tilt occurred at this same time in athletic shoes.
Trunk
Asymmetries in trunk segment motion between left and right steps accounted for 7% of the GGA score in athletic shoes and 10% in high heels. Overall, posterior trunk tilt was more pronounced in the patient than in the normative reference range, particularly in the high heels, which exhibited visually more asymmetric motion.
Power
High heels substantially reduced the average peak ankle power generation at push-off. Wearing high heels reduced the peak on the prosthetic limb by 70% and on the intact limb by 47%. When comparing between limbs, the average peak ankle power generation at push-off was 28% lower on the prosthetic limb in athletic shoes and 60% lower in heels.
Discussion
This study was undertaken to determine whether the results of a gait analysis could support anecdotal claims of improved gait in female prosthesis users walking in high heels. Overall, the use of high-heeled footwear with a pediatric running foot introduced no negative effects on gait symmetry in a female transtibial prosthesis user on level, straight terrain at a standardized speed. GGA scores were remarkably similar between athletic shoes and high heels. The greatest asymmetries occurred predominately at the ankle and knee in athletic shoes and were spread across the ankle, knee, and hip in high heels. Specifically, high heels substantially improved the symmetry of ankle joint motion, but this came at the expense of more asymmetrical hip motion.
Improvements in symmetry are not always synonymous with improvements in gait, as high heels are known to adversely affect several components walking mechanics (e.g. Simonsen et al. 5 ). For example, high heels substantially reduced ankle power generation at push-off. When walking in heels, the patient preferred a slower walking speed and shorter step length. Ankle motion was constrained by the shoes, resulting in a plantar flexed position and limited range of motion. Hip extension on the prosthetic side was substantially reduced and posterior trunk lean increased. These resulting kinematic changes created a more pronounced deviation from the normal lumbar lordosis, which may lead to the development of low-back pain. 5
The pediatric running foot enabled the subject to walk in 10-cm stiletto high heels. The use of a pediatric running foot provided the subject with greater versatility than a SACH foot or an adjustable heel height foot, which is limited to a 5-cm heel rise. With only minor adjustments in alignment, this foot can be worn with a variety of different shoes and with a variety of different heel heights (within ~2 cm). For example, the subject wears this design with approximately 20 other high-heeled shoes she owns. It fits securely within the high heels tested in this study with little movement between the shoe and the prosthetic, which can be a concern with some footwear that provide limited structural support. The pediatric running foot was also one of the lightest options considered. The reduced mass may have important implications for energy cost as mass, particularly when added distally on the limb, 15 negatively affects the metabolic cost of walking.
Conclusion
The goal of returning to pre-amputation footwear, to include 10-cm stiletto heels, should not be discounted for prosthesis users. Accommodations can be made using creativity in prosthetic foot selection to enable individuals with amputations to ambulate successfully. Stiletto high heels may not negatively affect gait symmetry in a prosthesis user, but this does not imply an overall improvement in gait mechanics. Thus, the assessment and training of gait mechanics with a variety of footwear may be warranted to ensure patient safety and promote autonomy.
Footnotes
Author contributions
E.R.E., D.H.L., and C.A.R. contributed to the study concept and design and critical revision of manuscript for important intellectual content. D.H.L. contributed to the prosthetic modifications. C.A.R. contributed to the data collection. E.R.E. contributed to the analysis and interpretation of data. E.R.E. contributed to the drafting of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.