
Abstract
Background:
Foot-drop is a common motor impairment of chronic stroke patients, which may be addressed with an ankle foot orthosis. Although there is reasonable evidence of effectiveness for ankle foot orthoses, user compliance is sometimes poor. This study investigated a new alternative to the ankle foot orthosis, the dorsiflex sock.
Case description and methods:
The dorsiflex sock was evaluated using an A-B single case experimental design. Two community-dwelling, chronic stroke patients with foot-drop participated in this study. Measures were selected to span the International Classification of Function, Disability and Health domains and user views on the dorsiflex sock were also collected.
Findings and outcomes:
The dorsiflex sock was not effective in improving participants’ walking symmetry, speed or energy expenditure. Participant 1 showed improvement in the distance he could walk in 6 min when using the dorsiflex sock, but this was in keeping with a general improvement trend over the course of this study. However, both participants viewed the dorsiflex sock positively and reported a positive effect on their walking.
Conclusion:
Despite positive user perceptions, the study found no clear evidence that dorsiflex sock is effective in improving foot-drop.
Clinical relevance
Although the dorsiflex sock offers an attractive alternative to an ankle foot orthosis, the case studies found no clear evidence of its efficacy. Clinicians should view this device with caution until further research becomes available.
Keywords
Background
Foot-drop is a common motor impairment seen among chronic stroke patients, characterised by a lack of active dorsiflexion. 1 Plastic, metal or composite-based ankle foot orthoses (AFOs) are commonly used to manage foot-drop, as recommended by the Royal College of Physicians. 2 Despite this recommendation, issues around comfort, usability and their restrictive nature during walking can limit their use. 3 Orthoses based on Lycra® or other similar materials (fabric orthoses) are being used clinically and may address these issues. However, despite positive results with similar products, primarily in a paediatric population,4–6 there are no reports on the efficacy of the application designed to correct foot-drop in an adult population with stroke. The principle behind the foot-drop application is to introduce a net dorsiflexion moment through elastic panels that are stiffer on the dorsal than the plantar aspect of a custom-fitted Lycra® sock. In addition, there is a suggested benefit from increased proprioception due to the tight-fitting nature of the garment. 7 We, therefore, aimed to investigate the effects of the dorsiflex sock (DS) in addressing foot-drop (DMOrthotics, Redruth, Cornwall, UK, http://www.dmorthotics.com/products/dynamic-lycra-orthotics.php) (Figure 1) by
Collecting initial data on the efficacy of the DS on step symmetry, energy expenditure, speed, exercise capacity and walking ability;
Investigating users’ perception of the DS.
Dorsiflex sock.
Case description and methods
Following ethical approval from University of Salford (REP 09/030), participants were recruited through the Manchester stroke club network. Participant information sheets were given to local stroke club network co-ordinators and distributed at meetings and electronically. Potential participants contacted the chief investigator and were screened against inclusion and exclusion criteria (Table 1).
Inclusion/exclusion criteria.
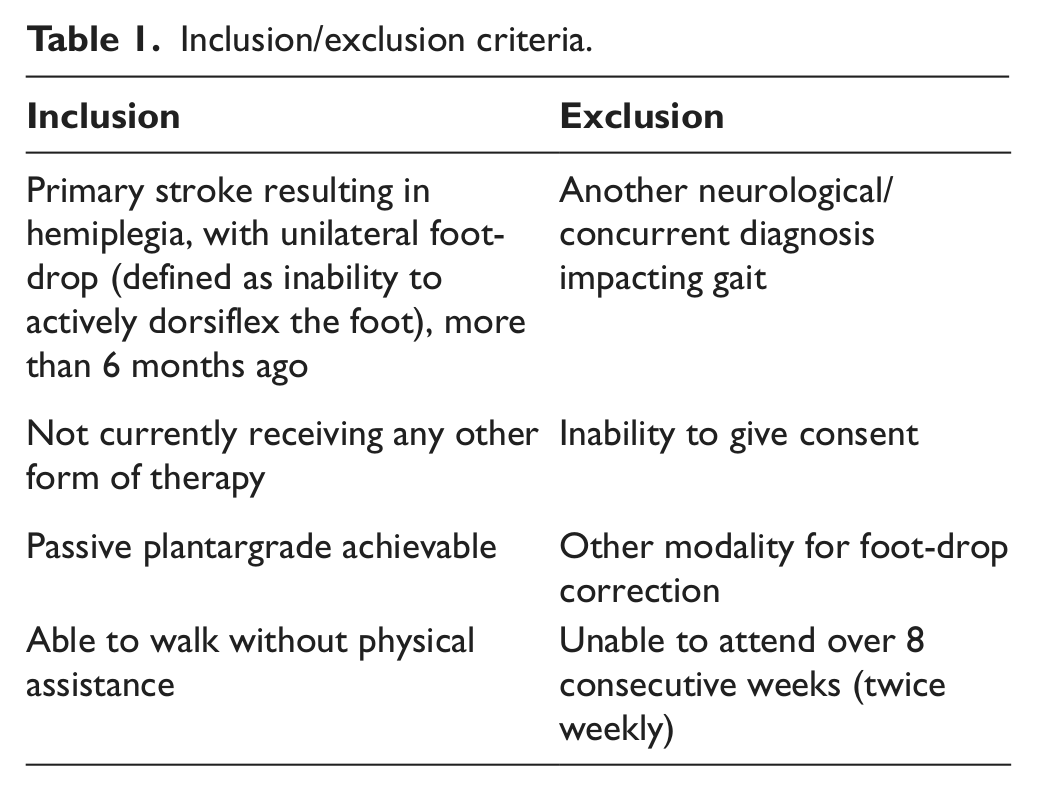
The majority of the screened volunteers were already using modalities for their foot-drop and hence were ineligible (see Table 1). A convenience sample of two who met the criteria, and were willing to complete the study protocol, were recruited to participate in this study.
Participants
Participant 1 was an unemployed 56-year-old gentleman with right hemiplegia. He could walk indoors with no walking aid, but used a four-point stick at night for safety. Outdoors he was independent with a stick over short distances, although he lacked the confidence to do this, depending on the conditions. He lived alone and was receiving no other therapy. His foot-drop was primarily due to weakness in his dorsiflexors. He had no cognitive deficit but did have expressive dysphasia.
Participant 2 was an unemployed 48-year-old gentleman with right hemiplegia. He was independently mobile both inside and out with a stick. He had been given a functional electrical stimulator but did not use it due to difficulties in donning. He lived with his partner and was receiving no other therapy. His foot-drop was primarily due to increased tone in his plantarflexors. He had no cognitive or communication deficits. Written informed consent for participation and publication was collected for both participants.
Design
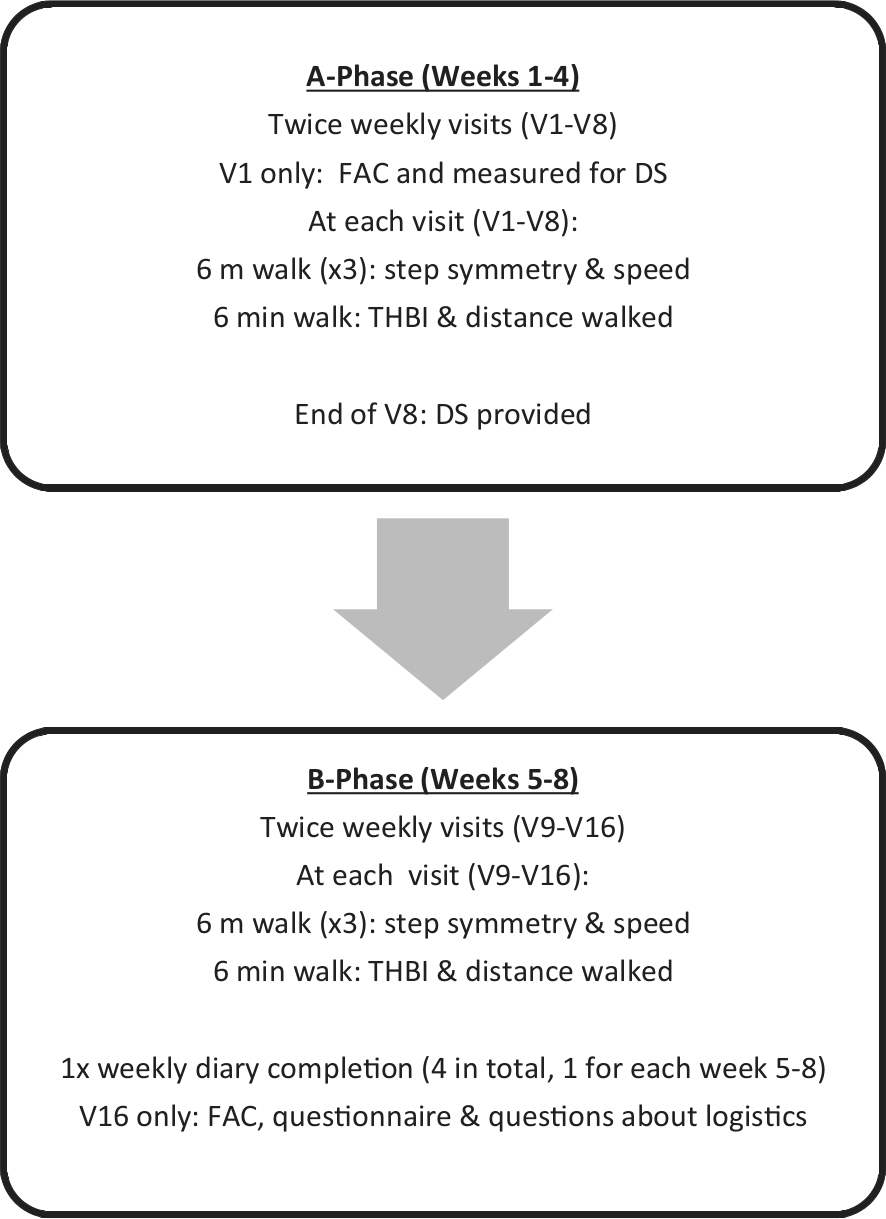
An A-B single case experimental design (SCED) 8 was used. Both phases (A and B) spanned 4 weeks, with participants visiting the University of Salford for testing twice weekly (V1–V16). This produced eight baseline (A) and eight intervention (B) data points, over a total of 8 weeks (Figure 2). Testing was on the same days each week and approximately the same time, no food or caffeine was allowed 1 h prior to testing, and participants rested for 2 min prior to testing to allow heart rate to settle. Participants wore the same shoes at every visit.
Protocol: all measures in A phase were taken without the DS; all measures in B phase were taken with the participant wearing the DS.
At V1, participants were measured for a custom DS, according to manufacturer guidelines, and the measurements were sent to the manufacturer. The DS was provided at the end of V8, then donning/doffing and care guidelines were explained, according to the manufacturer’s instructions. The participants were encouraged to take their DS home and use it between subsequent visits.
Outcome measures
According to the World Health Organization International Classification of Functioning, Disability and Health (ICF) model, measuring human function can be categorised as measures of ‘body functions and structures’ (BFS) and/or ‘activities and participation’. ‘Activities and participation’ can be further categorised into measurements within a standardised environment (capacity qualifiers (CQ)) and a person’s own environment (performance qualifiers (PQ)). 9 Outcome measurements that assess specific domains of these three ICF components (BFS, capacity qualifiers and PQ) were chosen from the relevant lower limb orthotic evaluation core set, developed by Brehm et al. 10
BFS
Gait pattern
At each visit (V1–V16), participants first performed three self-paced 6-m walks (with 1.5 m at either end 11 ). Mean values for step and stride regularity were calculated from vertical accelerations taken using a tri-axial lumbar-located accelerometer (Biometrics Ltd., Cwmfelinfach, Gwent, UK). 11 Step symmetry was then determined as a function of these. 11
Energy expenditure
Heart rate was monitored while the participants then walked for 6 min over a pre-defined course to calculate the total heart beat index (THBI). 12 This is a measure of energy expenditure which is reliable in non-steady-state conditions and is comparable to more established measures. 12
CQ
Gait speed
Mean values over the three 6-m walks 13 were calculated using a stopwatch.
6-min walk distance
The distance walked during 6 min (6-min walk distance, 6MWD) was recorded. This is a recognised measure of sub-maximal functional exercise capacity. 14
PQ
Walking ability
Functional ambulation categories (FAC) distinguish walking ability by the amount of physical assistance required ranging from ‘0’ (non-functional, ambulatory) to ‘5’ (independent, ambulatory). 15 These were recorded at V1 and V16.
User perception
Participants completed the validated user opinion orthotic questionnaire by Tyson and Thornton 16 at the end of V16. Diaries which recorded donning/doffing times, time worn and any effects/issues participants encountered were completed once a week in the intervention (B) phase on a day the participants were not at the university. 4 On V16, participants were asked specific questions on the logistical feasibility of the design and whether they would continue to use the DS. Although these measures are not within the core set of measures proposed by Brehm et al., 10 inclusion was justified in this first study of a new product. Figure 2 summarises when measures were collected.
Data analysis
Graphical interpretation and visual inspection was performed on all BFS and CQ data. 17 The autocorrelation coefficient, ‘the extent to which scores at one point in a series are predictive of scores at other points in the same series’ (p. 652), 18 was calculated for the baseline (A) data points using the method described by Bengali and Ottenbacher. 18 In the absence of significant autocorrelation (p ≤ 0.05), which would bias any calculations based on averages, the quasi-experimental 2-standard deviation (SD) method was applied. 19 This involves calculating a 2-SD ‘band’ based on baseline (A) data points which is then projected onto the intervention (B) phase. If two successive intervention (B) phase data points sit outside of the band, it is said to show a significant (p < 0.05) improvement. 19 PQ measures were recorded and summarised.
Findings and outcomes
BFS and CQ measures
Visual inspection of THBI, walking speed and 6MWD (Figures 3 and 4) showed an improvement trend for Participant 1 over the course of testing (V1–V16). Conversely, step symmetry demonstrated a declining trend for Participant 1. Neither of these trends appeared to be affected in any way by the introduction of the DS (Figures 3 and 4). Significant baseline autocorrelation, 18 even with first difference transformation, 19 was found in all measures apart from 6MWD. Participant 1’s improvement in this measure was classed as significant (p < 0.05) using the 2-SD method. 17 Participant 2 showed no change in any measure (Figures 3 and 4).
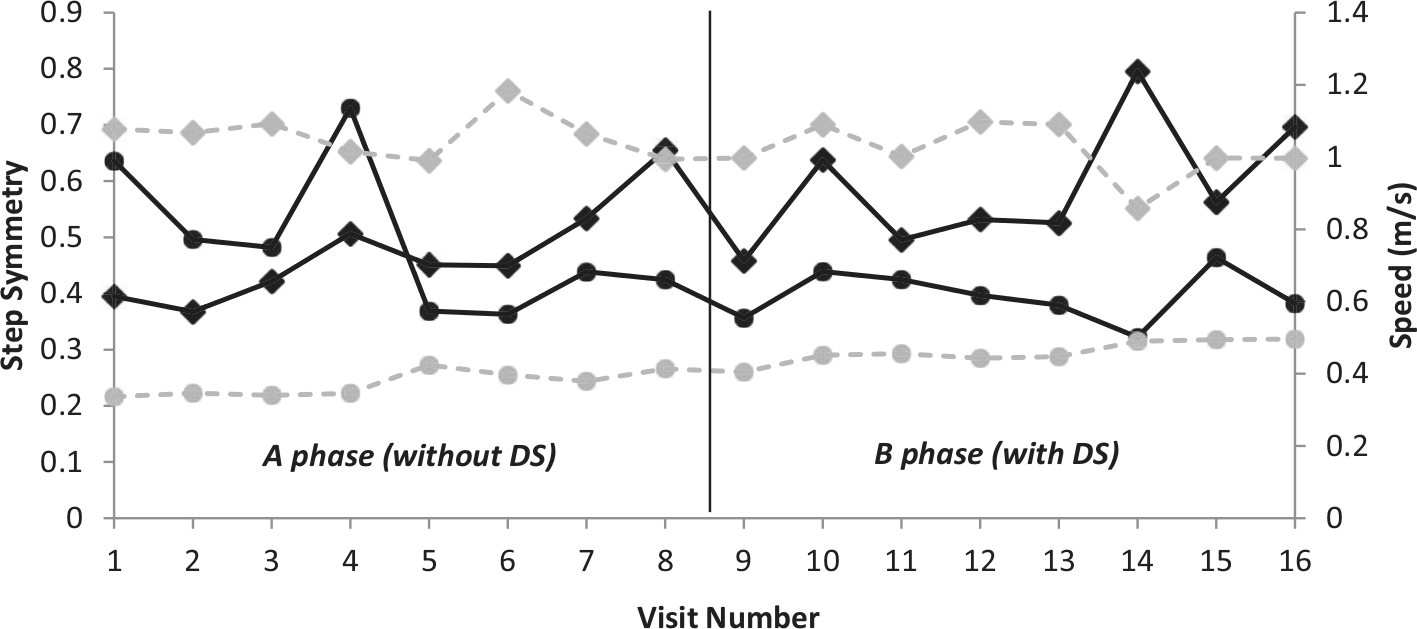
Average step symmetry and walking speed, both measured over three self-paced 6-m walk tests. Symmetry is depicted with a solid black line and speed with a dashed grey line. Participant 1 is represented by a circle and Participant 2 by a diamond. The 2-SD bands are not depicted to aid visual inspection and two data sets are shown to minimise the number of figures used.
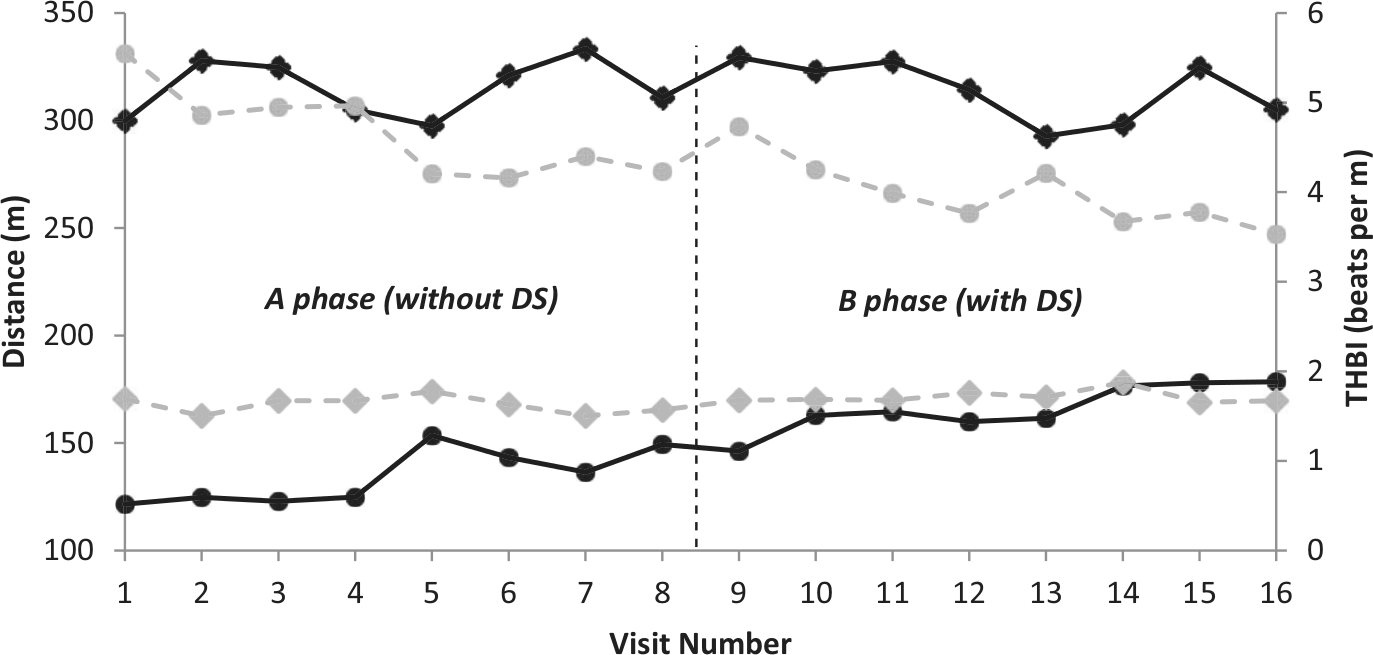
Both THBI and 6MWD were measured over a 6-min walk test. Distance is depicted with a black solid line and energy expenditure with a grey dashed line. Participant 1 is represented by a circle and Participant 2 by a diamond. The 2-SD bands are not depicted to aid visual inspection and two data sets are shown to minimise the number of figures used.
PQ measures
Walking ability
According to the descriptions by Mehrholz et al. 15 at V1, the FAC for Participant 1 was 4 (ambulatory, independent, level surface only), and for Participant 2 was 5 (ambulatory, independent). These scores were unchanged at V16.
User perception
With regard to the questionnaire, 16 Participant 1 reported the DS resulting in ‘little’ or ‘much’ improvement in all the areas of gait asked about. Overall, he reported his walking being ‘much better’. 16 The only impact Participant 2 reported was ‘a little improvement’ in the ability to lift his toes, but overall he felt his walking was ‘better’. 16 Both felt the DS was ‘easy’ to don/doff, ‘comfortable’ and were ‘not concerned’ by its appearance. 16
Diary entries showed that donning/doffing was consistently independent for both participants and times remained consistent throughout (Participant 1 reporting 2–3 min to don/doff; Participant 2 reporting 10–15 s to don and 5–10 s to doff). This was not consistent with what was observed, with both underestimating how long it took. Participants wore the DS all day after their first week, where the manufacturer recommended a gradual increase in use. Regarding the effects of the device, Participant 1 consistently wrote that his affected leg felt ‘very very limp’ without the DS on and he wrote he felt ‘better with it on’. Participant 2 had less to report, but noted that with the DS, ‘his toes were not catching when walking’.
Questioning around the logistics of the study design indicated that for Participant 1, two visits per week were all they could manage, but that he enjoyed his involvement as ‘it got him out of the house’, whereas Participant 2 could have come more frequently. Both stated they would carry on using the DS.
This study set out to preliminarily investigate the efficacy and users’ perceptions of the DS. The single quasi-statistical change in the 6MWD seen for Participant 1 cannot be confidently attributed to the effects of the DS. There was no change in any other BFS or CQ measures, and the change in the 6MWD is confounded by the continually improving trend observed for Participant 1 (Figures 3 and 4). 20 When taken together, this suggests it is more likely that the observed change was due to the repeated bouts of exercise during the walking tests at V1–V16, rather than the wearing of the DS. The DS had no impact on any measured aspect of Participant 2’s walking.
In terms of PQ measures, walking ability (FAC) was not affected by the DS. In contrast to the objective findings both participants’ perceptions of the impact of the DS on their gait were positive. This could be due to the inclusion/exclusion criteria (Table 1), which notably required repeated dedicated testing over 8 weeks during the day and the absence of other foot-drop modalities (Table 1). This restricted eligibility to those without daytime commitments and who were not having health-care input. The combination of these factors may well have resulted in a self-referred convenience sample whose views were positively influenced by the fact that their foot-drop was being addressed.
The A-B design is the basic SCED and has well-established limitations.8,17 As the DS could have a carryover effect, recruitment numbers were unknown (and were ultimately small), and compliance could not be predicted, alternatives such as A-B-A or multiple baseline design8,21 were not deemed appropriate. In addition, the participants were rather homogenous being male, right-sided hemiplegic and functioning at a relatively high level which limits the generalisability of the findings.
However, the design and measures chosen aimed to capture the breadth of impact of the DS and are indicative of measures used in studies that informed the Royal College of Physicians guidelines. 2 In contrast to our findings, thermoplastic AFOs have been reported to have a significant impact on a range of measures including speed, symmetry, exercise capacity and walking performance.2,3,22
Conclusion
Despite positive views of the DS from both participants, and the recognised limitations, this preliminary study found no clear evidence to demonstrate that the DS, with its current design, was effective in improving walking for two community-dwelling, chronic stroke patients with foot-drop. It should be viewed with caution as an alternative to AFOs, until further research becomes available. To strengthen the external validity of these findings further research should include a greater variety of participants in terms of side of hemiplegia, age, gender and FAC to represent the heterogeneous stroke population. Comparison to an AFO, or placebo, using either a SCED or a group design would strengthen internal validity. Measures should continue to refer to Brehm et al. 10 core set recommendations; however, BFS might be best served by using three-dimensional (3D) gait analysis, which would record the effect of the DS on kinematics, including toe clearance, a measure of trip risk, during swing. 23
Footnotes
Acknowledgements
We would like to thank the two participants, DMOrthotics for providing the DS free of charge and Helen Carrington for her help with data collection.
Declaration of conflicting interest
The authors declare that there is no conflict of interest with this work.
Funding
This work was supported by a bursary from the University of Salford.