
Abstract
Background:
This article describes the development and evaluation of a new medial linkage orthosis to potentially assist paraplegic patients to ambulate.
Case description and methods:
The orthosis was initially designed using the solid works program and was subsequently evaluated when used by a spinal cord injury subject to test the structure during standing and walking. Gait analysis was used to compare the medial linkage orthosis to a standard hip–knee–ankle–foot orthosis.
Findings and outcomes:
The results demonstrated improvements in gait velocity, step length, and decreased compensatory motions in the new orthosis compared to the hip–knee–ankle–foot orthosis.
Conclusions:
The results propose that this new Araz medial linkage orthosis could be used to assist paraplegic subjects who have adequate ranges of motion and also with weakness or reduced tone to stand and walk.
Clinical relevance
The Araz medial linkage orthosis can potentially provide standing and walking assistance for spinal cord injury patients.
Introduction
Walking and standing activities have been shown to have positive physiological and psychological effects such as decreased osteoporosis, fracture incidence, and spasticity and contractures and increased self-esteem and confidence in patients with spinal cord injury (SCI).1–3 Several types of mechanical orthoses have been developed to assist SCI patients in walking and standing. Hip–knee–ankle–foot orthoses (HKAFOs), hip guidance orthoses (HGOs), advanced reciprocating gait orthoses (ARGOs), and isocentric reciprocating gait orthoses (IRGOs) are all examples of orthoses that have been shown to assist walking in this patient group.4–9
The Walkabout and the Primewalk orthoses are both examples of medial linkage orthoses (MLOs), which also permit walking in this patient group.4–8 These types of orthoses have medially positioned hinged hip joints, which also incorporate a sliding mechanism to connect two KAFOs for paraplegic patient walking. The Walkabout orthosis has the advantage of being compatible with wheelchair use due to easy donning and doffing and its cosmetic appearance when compared to other mechanical orthoses. 4
The Walkabout system has a single-axis hinged joint that is positioned at a lower level than the anatomical hip joint. Saitoh et al.7,10 demonstrated that because it produced a slow cadence and short stride, walking speed with the Walkabout orthosis was low. Based on this limitation, Middleton et al. 9 developed the Moorong MLO, which has a sliding link centered on the anatomical hip joints.They reported that the new orthosis could improve walking in comparison with the Walkabout system in a paraplegic patient. Saitoh et al. 7 also developed another medial linkage device, the Primewalk which has a sliding-type medial hip joint sited adjacent to the normal anatomical hip joint, in an attempt to improve on the design of the Walkabout system.
One positive effect of the Walkabout orthosis is its reported reduction of energy consumption for paraplegic subjects compared to when walking with KAFOs.10,11 However, a comparison between the Walkabout orthosis and an IRGO has demonstrated decreased speed of walking and high energy consumption in Walkabout compared to the IRGO in walking in patients with SCI. 12 When comparing temporal spatial parameters, Saitoh et al. reported that the Primewalk was more effective than the Walkabout when used by paraplegic patients. The mean speed of walking, cadence, and step length when using the Primewalk was low compared to the IRGO.
A MLO does not provide a reciprocating effect when worn during ambulation. Therefore, in order to improve the efficacy of MLOs, a new medial linkage system–type orthosis for walking in patients with SCI was designed and fabricated for this study, which would also provide a reciprocating effect.
Case description and methods
Subject and experimental protocol
A female patient (age = 24 years, weight = 56 kg and height = 165 cm), with an incomplete lesion at T12 level grade B according to the American Spinal Injury Association (ASIA) score, participated in this study. She was an experienced HKAFO user with normal upper limb strength. Inclusion criteria for participation in this study were no history of cardiovascular or pulmonary diseases, contractures, severe spasticity, obesity, or asymmetric hip positions and were at least 6 months post injury. This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences. A standard HKAFO and a KAFO with Araz medial link system were analyzed when used for walking by the subject with SCI.
Orthosis considerations
Details of the Araz MLO
The Araz MLO was developed incorporating a medial linkage orthotic system designed to provide reciprocal motion and to improve the walking efficacy of KAFOs or HKAFOs in patients with SCI (Figure 1). An MLO with a single axis of rotation was previously proposed by Cliquet et al. 11 and Kirtley and McKay 4 (the Walkabout orthosis), which could control adduction and abduction of the lower limbs during walking. Specifically, the linkage prevented abduction of the swing-through leg while the body is tilted to create ground clearance for the swinging leg and, at the same time, prevented abduction of the stance leg under body weight. The Walkabout orthosis has a hinge and single-axis mechanism with 100–150 mm difference between linkage axis and the centers of the hip joints. 13 To solve the positional difference between the hip joints and the hinge axis of the Walkabout orthosis, the Moorong MLO and Primewalk orthoses were developed.
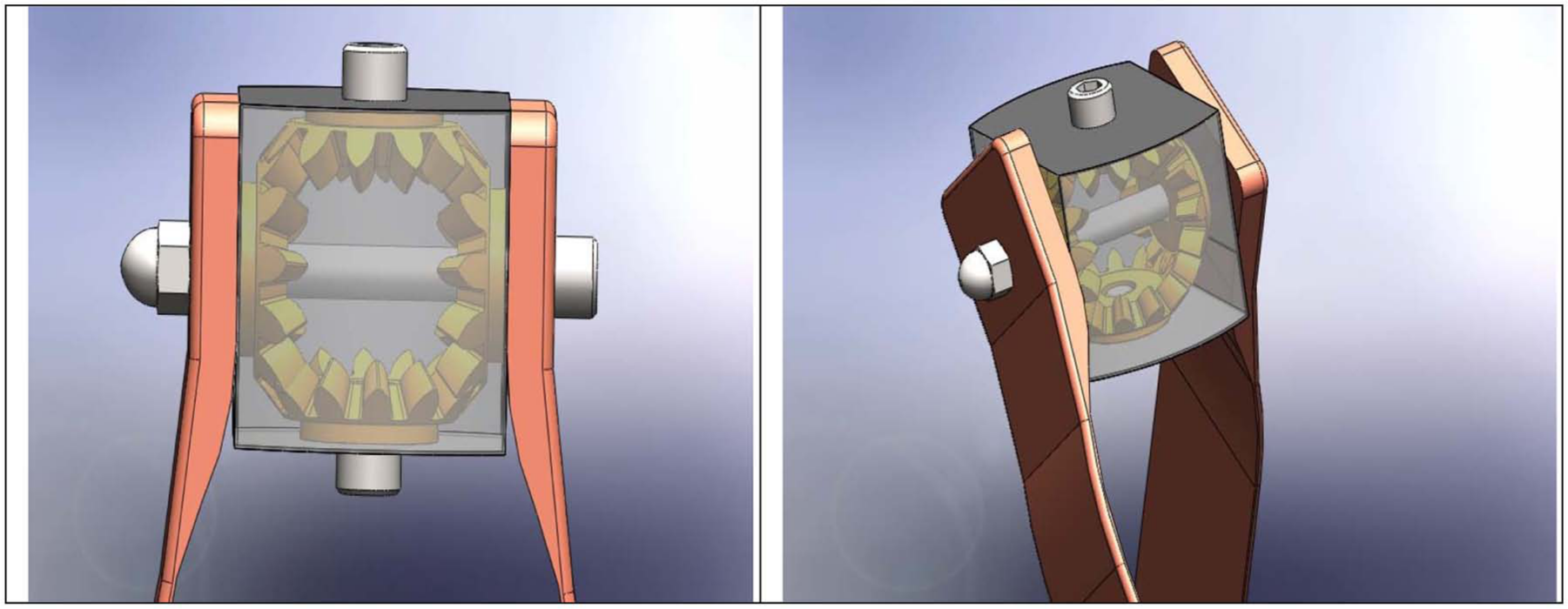
Araz medial linkage orthosis.
To this end, it was decided to extend the MLO system by providing a reciprocal motion between the two lower limbs and the hinge axis of the MLO. This was achieved by designing and fabricating the medial linkage with a reciprocating link.
The Araz MLO is therefore a proof of concept design incorporating a combination of a medial link system and reciprocating link concept prototype based on a single case study. The Araz MLO was made from duralumin and weighed 410 g (Figure 2). The reciprocal link mechanism was designed with the maximum angular range of motion (ROM) available by the mechanism being limited to 45°.

Anterior and superior view of the Araz MLO.
The weight of the patient was shifted over onto the stance leg by tilting the trunk, and this provided slight elevation of the contralateral leg, which allowed it to clear the floor as the swing phase was initiated. This was achieved by the patient extending the trunk to induce hip extension on the stance side, which caused flexion of other limb using the gearbox positioned between the two legs.
The Araz MLO mechanism was designed to link the two lower limbs and transmit part of the created torque about the hip of the extremity (leg) in stance phase of gait to the contralateral lower leg in a reciprocal approach to provide hip flexion. This function facilitates provision of swing phase of one leg with simultaneous push-off on the contralateral lower limb. Figure 3 shows the new mechanism mounted on bilateral cosmetic KAFOs, which were used in this study. Individuals with SCI have lost sensation in most of the lower limbs. A design of a device must take into account the safety of the users. For this aim, the device is attached to the thigh sections of the cosmetic KAFOs as in other designs that have been successfully used.

New mechanism on KAFOs, which was used in this study.
Gait analysis
The patient walked through a straight 6-m walkway at a gait analysis laboratory, which was equipped with a six-camera Vicon digital motion capture system (Oxford Metrics, UK) using a capture frequency of 100 Hz to gather data when the patient used each of the two types of orthoses. In total, 18 reflective markers were used on the lower extremity and the trunk. Markers were placed bilaterally over the position of the greater trochanter, anterior superior iliac spine (ASIS), the lateral condyle of the femur, the head and lateral malleolus of the fibula, the second metatarsal, the calcaneus, and over the jugular notch, the spinous process of the seventh cervical vertebrae, and the acromioclavicular joints.
The markers of lower limb joints were put on the uprights of the orthoses as close as possible to the positions where they would be located on the patient’s skin. The patient had practice walks in the gait laboratory to become familiar with the orthosis before data gathering. For all walking conditions with each orthoses, the SCI patient used a walking aid for stability and safety in walking with orthoses. For each test situation, the patient walked along the walkway five times. Cadence, step length, speed of walking, hip joint ROMs, and compensatory motions were analyzed from the motion analysis data. Data were averaged for both sides.
Findings and outcomes
Hip angle
The maximum hip flexion angle was 10.8° ± 2.2° and the maximum extension angle was 6.4° ± 1.6° when the SCI patient used the Araz MLO. However, the average flexion and extension angles of the hip joints were limited to 8° ± 1.8°and 5.2° ± 1.4°, respectively, when using the standard HKAFO. The overall effect of using the new orthosis demonstrated an increase of 4° in the average total hip ROM during ambulation.
Step length, walking speed, cadence, and compensatory motion
Table 1 shows temporal/spatial data when both orthoses were used. Improvements in step length, speed of walking, and cadence were noted when walking with the Araz MLO as compared to the standard HKAFO.
Mean ± SD of hip joint ROM and spatial–temporal gait parameters in walking with two types of ARGO.
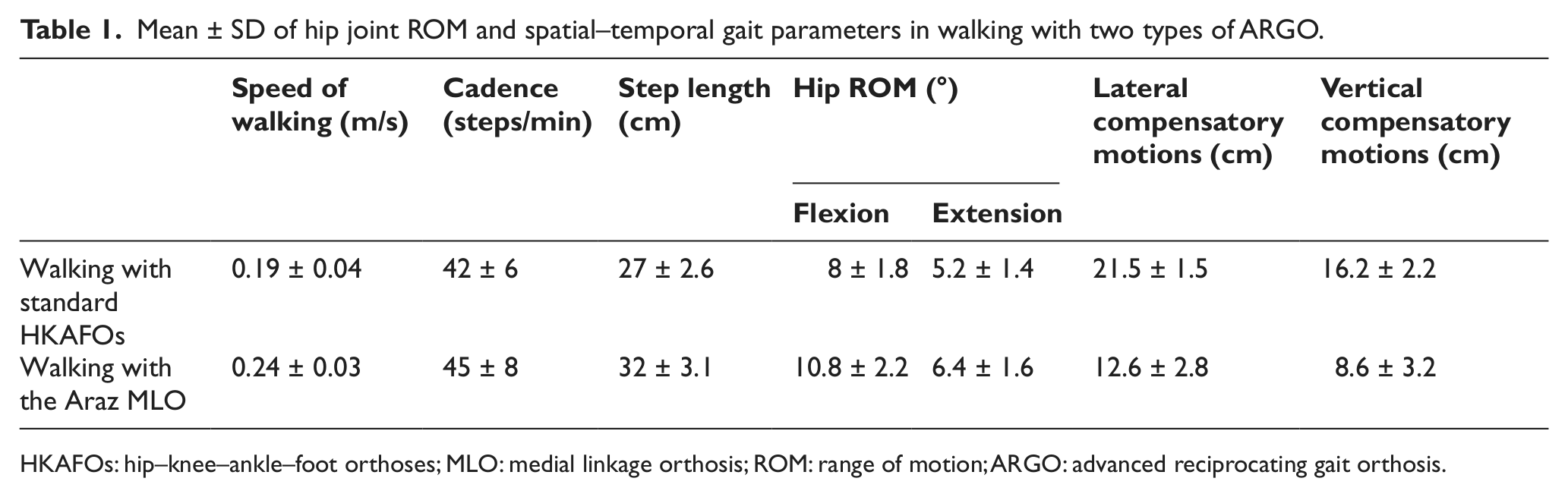
HKAFOs: hip–knee–ankle–foot orthoses; MLO: medial linkage orthosis; ROM: range of motion; ARGO: advanced reciprocating gait orthosis.
The mean and standard deviation (SD) of the lateral and vertical compensatory motions in walking with the two types of orthoses are shown in Table 1. Lateral and vertical compensatory motions are needed for ambulation of the trunk from side to side in SCI individuals in using orthotic devices. Walking with orthoses associated with compensatory motions causes high loads on the upper limbs in the paraplegic patients. Compensatory motions were decreased when the patient used an HKAFO with the Araz MLO as compared to standard KAFO (Table 1). The results therefore demonstrated that during ambulation, average total hip ROM was increased by 23%, mediolateral hip excursion was reduced by 42%, and vertical hip excursion was reduced by 47% in the volunteer SCI patient when walking with the Araz MLO compared to the standard KAFO.
Discussion
In this study, speed of walking was improved when walking with the new orthosis compared to standard HKAFOs. The sliding mechanism of the new system that provided an axis of rotation nearer to the anatomical hip joint associated with the reciprocal link produced a higher speed of walking and longer step length. Previous studies in this field by Saitoh et al. 10 and Middleton et al. 13 reported similar results in improvement of walking speed by using a sliding mechanism in an MLO,10,13 but they did not develop a reciprocating link associated with the medial linkage.
The reciprocating link is effective on walking and may reduce energy consumption in patients with SCI. The present new orthosis provides reciprocating movement of the lower limbs in conjunction with the medial linkage, which helps to stabilize the pelvis and lower leg in standing. Consequently, the Araz MLO caused an increase in walking speed and step length compared to a standard HKAFO. In this study, a comparison was performed between the new orthosis and a standard HKAFO as a first stage of evaluation on walking in paraplegic patients. Comparison between the Walkabout and Primewalk orthoses with this new orthosis with regard to temporal spatial parameters and energy consumption would be beneficial for a future study in this field.
In paraplegic patients who use an orthosis for ambulation, the fixed extended position of the knee joint in an orthosis means that foot clearance and swing of lower limb need to be provided by tilting of the trunk. This tilt occurs in both lateral and vertical directions. These compensatory motions can cause high loads on the upper limb joints and high levels of energy consumption in walking with the orthosis. Using this new orthosis reduced lateral and vertical compensatory motions compared to walking with a standard HKAFO. This parameter has been evaluated with mechanical and powered gait orthosis on SCI patients by Arazpour et al.14,15 and Ohta et al., 16 who reported improvement in these parameters when using a powered orthosis compared to mechanical IRGO and ARGO.
Using a sliding and hinged type of medial linkage in an orthosis has been associated with hip joint instability associated in walking. 17 The Araz MLO can only provide reciprocating motion, but for future design, we offer a device with sliding type that creates reciprocal movement and matches anatomic and orthotic joints. Pelvic instability may be improved with the new orthosis described in this study based on a reciprocal link.
Conclusion
Consequently, in this study, a new MLO with reciprocal link was compared to an HKAFO, and the encouraging preliminary results indicated that an improved and more efficient orthotic system for walking performance by SCI subjects may be proven in a larger and more extensive clinical trial. Further evaluation of the Araz MLO is therefore warranted during ambulation by a larger group of SCI subjects, which should also include an analysis of its effect on oxygen consumption.
Key points
Medial linkage orthoses (MLOs) (e.g. the Walkabout and Primewalk) could be used by paraplegic patients for ambulation.
The Araz MLO has been developed with a medial linkage orthotic system designed to provide reciprocating motion and to improve the walking efficacy of knee–ankle–foot orthoses (KAFOs) or hip–knee–ankle–foot orthoses (HKAFOs) in patients with SCI.
The Araz MLO has the potential to be used as an alternative approach to walking by SCI patients.
Footnotes
Conflict of interest
The authors did not have any conflicts of interest with regard to the study presented in this article.
Funding
We thank the University of Social Welfare and Rehabilitation Sciences (USWR) for financial support (grant number 91/801/1/13979) for this research.