
Abstract
Background and aim:
Digital technology is becoming more accessible for common use in medical applications; however, their expansion in prosthetic and orthotic laboratories is not large because of the persistent image of difficult applicability to real patients. This article aims to offer real example in the area of human facial prostheses.
Technique:
This article describes the utilization of optical digitization, computational modelling, rapid prototyping, mould fabrication and manufacturing of a nasal silicone prosthesis. This technical note defines the key points of the methodology and aspires to contribute to the introduction of a certified manufacturing procedure.
Discussion:
The results show that the used technologies reduce the manufacturing time, reflect patient’s requirements and allow the manufacture of high-quality prostheses for missing facial asymmetric parts. The methodology provides a good position for further development issues and is usable for clinical practice.
Clinical relevance
Utilization of digital technologies in facial prosthesis manufacturing process can be a good contribution for higher patient comfort and higher production efficiency but with higher initial investment and demands for experience with software tools.
Background and aim
Rapid prototyping (RP), optical digitization and virtual prototyping software have become instruments of general use in the area of medical applications, 1 especially in the area of prosthetic applications. During the last decade, the development of technologies minimized the previous main problems 2 associated with the use of technology in the specific areas of orthotic and prosthetic aids. In the field of facial prosthesis, Ciocca et al. 3 describe the process for the production of ear prostheses step by step using a three-dimensional (3D) laser scanning of a patient’s face, using 3D models of ear from digital library and RP of moulds for silicone processing. Another article focused on the facial replacements 4 describes the use of computed tomography (CT) and special 3D scanner designed to scan the skull. For creation of the missing organ, authors used a mirrored geometry of the left ear. The moulds created on the 3D printing machine were used for production of the final casting of the prosthesis. Also Qiu et al. 5 deal with the use of stereolithography for the production of a four-piece mould for the nasal prosthesis. The geometry of the patient’s face was obtained by CT and reconstructed using Mimics software. The modifications were implemented by the Geomagic program. As the nose is not a paired organ, the nose geometry was obtained from the database (Ninth People’s Hospital, Shanghai, China). Previous studies 6 clearly indicate the direction of the current development trends in facial prostheses and considerable emphasis on the use of technologies, which increase the efficiency of the whole process from design to production and bring better patient comfort and convenience. The aim of the following text is to describe the manufacturing process of the nasal prosthesis, with use of commonly available digital technologies, which can be more comfortable for the patient and can bring a high-quality result in shorter time.
Technique
The whole methodology (Figure 1) covers the following six main steps:
Data acquisition of the whole face and nose geometry.
Virtual reconstruction, the nose adjustment and positioning.
Manufacturing of the nose prototype via RP technology.
Mould fabrication.
Manufacturing of the silicone prosthesis.
Final fitting on the patient’s face.
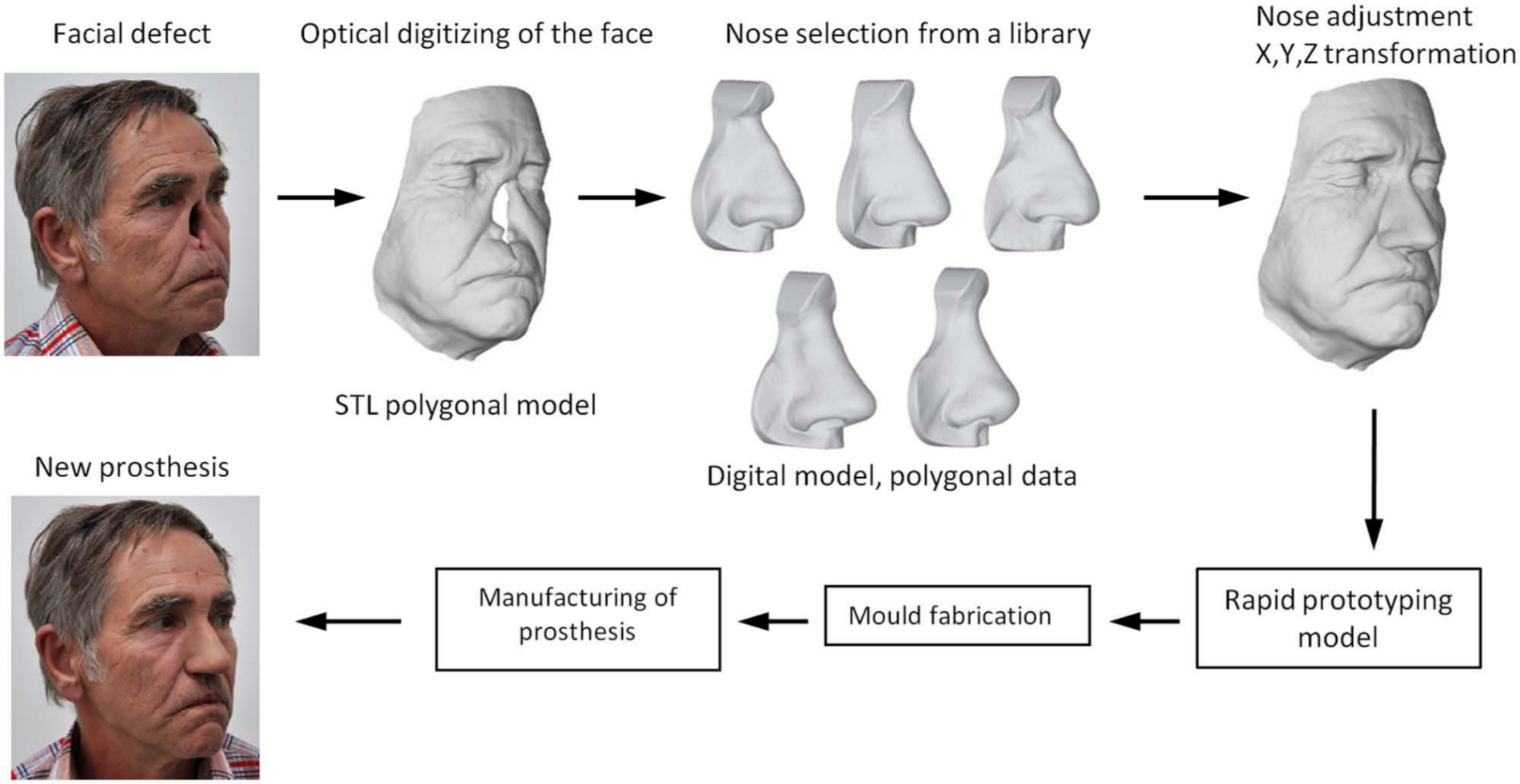
Design process and the methodology of the facial prosthesis manufacturing.
Data acquisition
Face digitization
The first step in the process was the digitization of a patient’s face. With respect to the speed and accuracy of scanning, the ATOS scanner with a camera resolution of 0.8 million pixels, which with the use of a measuring volume of 250 × 250 × 250 mm3 captures surface with resolution of 2 points/mm, was used in this work. The scanner works on the principle of structured fringe projection. The system consists of one projector lens and two cameras with charge-coupled device (CCD) chips. The projection unit projects the fringe patterns onto the object, and the deformed shape of the fringes is captured by two cameras.
The face was scanned from two sides (Figure 2), and the total time needed to scan was 25 s. The scanning was done without reference points, and both scans were spatially aligned using the ‘best fit’ software function that, on the basis of geometric deviations, aligns the polygonal meshes with the smallest deviation. The resulting data were stored in the standard STL data format (polygonal data format).
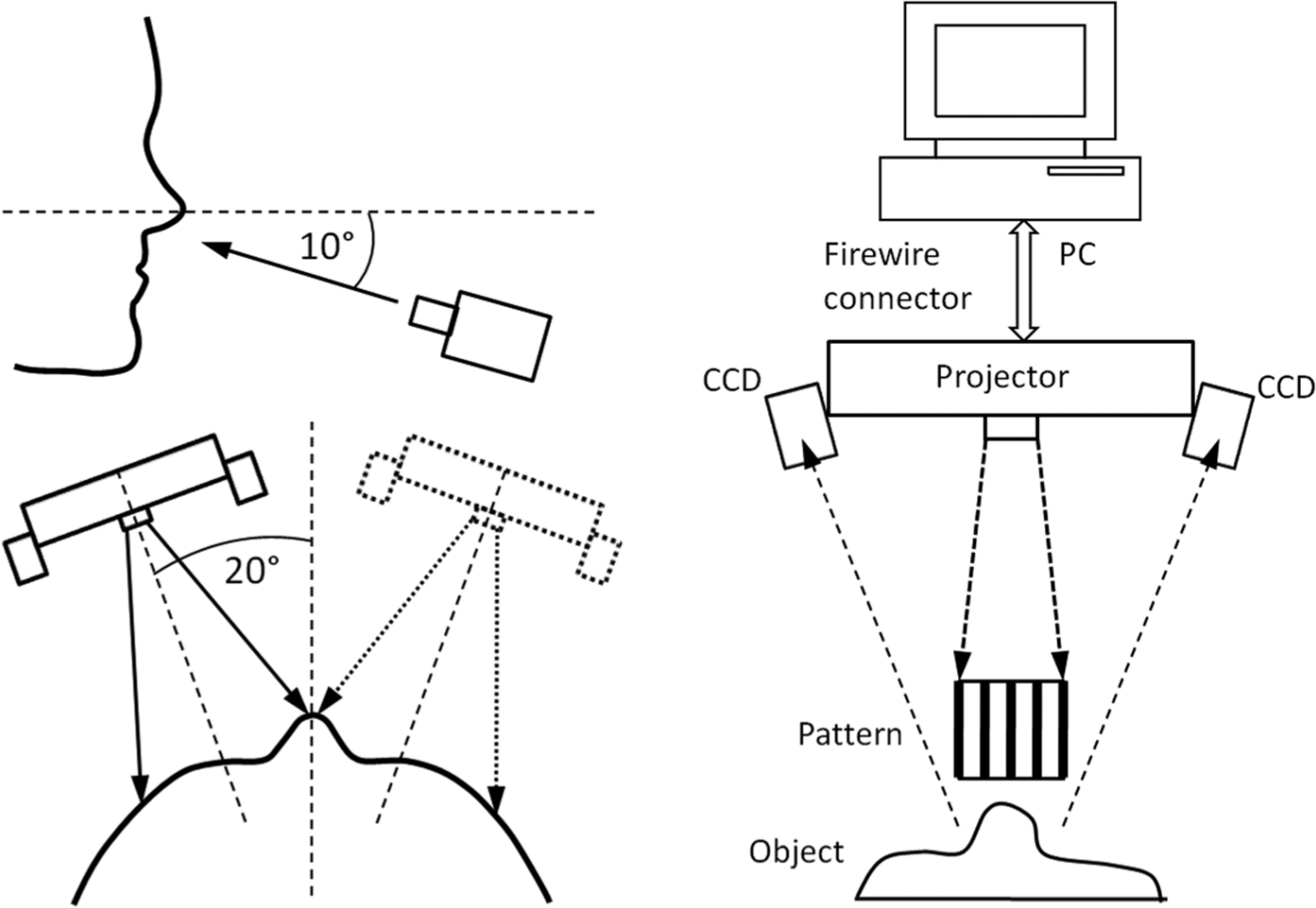
3D optical digitization. The procedure – two positions of the scanner during scanning of patient’s face (left part); measurement setup – fringe pattern projected on the object is captured by two CCD cameras and analysed in PC, which is connected by FireWire to 3D scanner (right part).
Selection of the nose
If possible, it is preferable to capture a digital copy of the nose surface 7 before surgery and get a natural shape. However, 3D digitization is often performed after surgery, and only then the shape of the remaining tissue after removal of the nose is obtained. The nose must be replaced by suitable donor geometry. Physical classification of noses was described in literature. 8 Based on this typology, we have worked out a database of computational models (Figure 1) of different types of noses (the Roman, the Greek or Straight, the Nubian or Wide-nostrilled, the Hawk, the Snub and the Turn-up or Celestial nose). The 3D digital models were obtained by 3D scanning (ATOS scanner) of plaster models of noses taken from donors. Plaster casts can be accurately scanned in high resolution, and accuracy can be obtained in comparison with the direct scanning of the patient. A deviation from the real shape is in the order of hundredths of millimetres, which is more than sufficient for this application. The nose was selected, with regard to gender, from the digital library with the use of older photographs of the patient.
Virtual alignment
The initial alignment (Figure 3(a)) of a digital model of the nose and the scanned data of the patient’s face was performed in the Rhinoceros software. Individual models of the noses were placed in layers, whose visibility can be turned on or off.
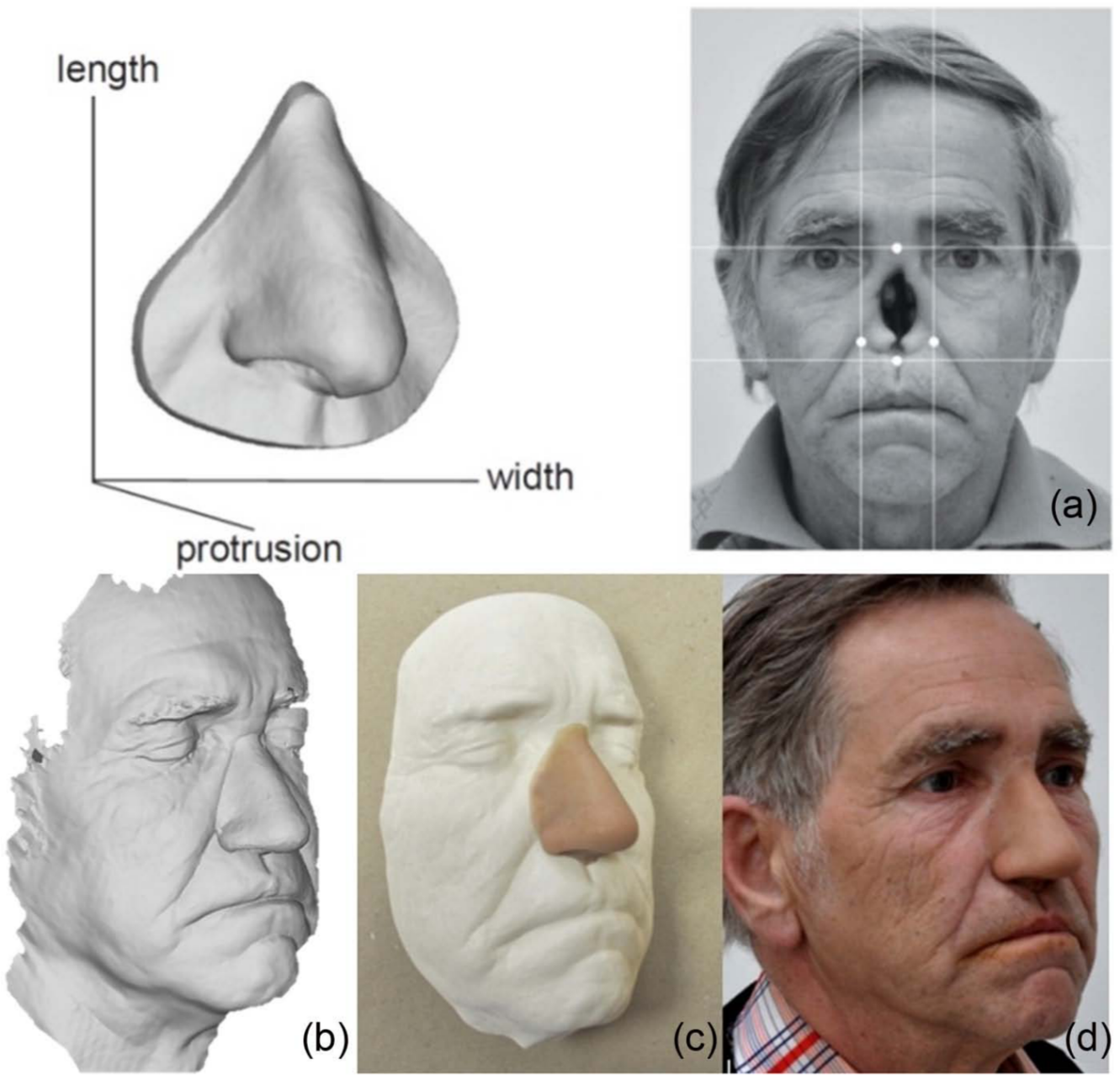
(a) The initial state – scanned plaster cast of the nose and patient facial defect, (b) alignment of the digitized data of the nose and patient face in Rhinoceros software, (c) final prosthesis fitted on plaster cast and (d) final prosthesis fitted on patient’s face.
Such an organized database enables fast access to the scanned data and its quick comparison and the consequent adjustment. After importing the face, the data are manually oriented in the basic coordinate system and merged with the geometry of the nose. The size of the nose is then adjusted (in x-, y- and z-axes independently) according to the proportions of the face (Figure 3(b)). The model is then exported to STL format.
RP
The modified model of the patient’s nose was fabricated by the RP method called ‘3D printing’ (ZPrinter 310 Plus; Z Corporation, Burlington, MA, USA). The RP model was printed in 325 layers (the thickness of 1 layer is 0.1 mm), and it lasted for 65 min. The 3D printer uses a powder/binder/infiltrant system for the model building. The technology has a 300 × 450 dpi resolution and layer thickness of 0.089–0.2 mm. The print head with 304 nozzles sprays a binder at defined positions into layers of powder. The wax pattern is manufactured by means of creating a silicone mould (S20; Torten, Nachod, Czech Republic) over the RP model and then by pouring the melted wax (Modelling wax epithetics; Bredent, Senden, Germany) into the silicone mould.
Mould fabrication
The final silicone nasal prosthesis was manufactured in a mould. A two-piece mould (Figure 4) was designed from a high-quality stone plaster (Die-Kean; Heraeus Kulzer, Hanau, Germany). The base of this mould was built according to the precise impression of the patient’s face. A wax pattern of the nose was manually blended on the base of the mould to ensure smooth edges and surface overlapping of the nasal prosthesis. The second part of the mould was made by pouring the stone plaster over the wax pattern fitted on the base of the mould.

The final two-piece plaster mould for silicon prosthesis manufacturing.
Manufacturing of a silicone prosthesis
The custom-made silicone nasal prosthesis was fabricated from LSR A-221-05 and A-223-40 silicones (Factor II, Lakeside, AZ, USA). The silicone blend was cured inside a mould in an oven (90°C, 90 min). The colouring of the prosthesis was performed by intrinsic and extrinsic colouring processes (Human Coloration System; SiliClone Studio, Valley Forge, PA, USA). Extrinsic staining (anatomical surface details, surface matting) and trimming were the last stages of the manufacturing process of the prosthesis. The silicone nasal prosthesis was fitted onto an RP model before fitting onto the patient’s face.
Fitting on patient’s face
A patient after total rhinectomy has been fitted with a custom-made nasal prosthesis (Figure 3(d)) designed and fabricated by using the computer-aided design (CAD)/computer-aided manufacturing (CAM) methods. Two types of direct adhesive fixation (Pros Aide Adhesive; Alcone Company, Long Island City, NY, USA, and B-460 Silicone Adhesive; Factor II) were chosen for this patient, and it was a successful way of retention in daily use. There was an option to increase the retention by wearing spectacles that fitted well in upper part of nasal prosthesis; nevertheless, the patient was satisfied and had not used this option. The result was satisfactory for the patient, the plastic surgeon and the prosthetic team.
Discussion
The presented methodology reflects the current possibilities of using RP technology and optical digitization for manufacturing of facial prosthetics. The procedure uses optical 3D scanning technology of the plaster casts, which allows achieving greater accuracy and detail of the digital model in comparison with the laser scanning. It is practically possible to scan the skin texture. However, the used RP technology does not allow the exact replication of the modified model. In terms of time consumption (Table 1), it can be stated that digitization, data processing and 3D printing are the least time-consuming.
Time demands of the individual processes during the nose prosthesis manufacturing.
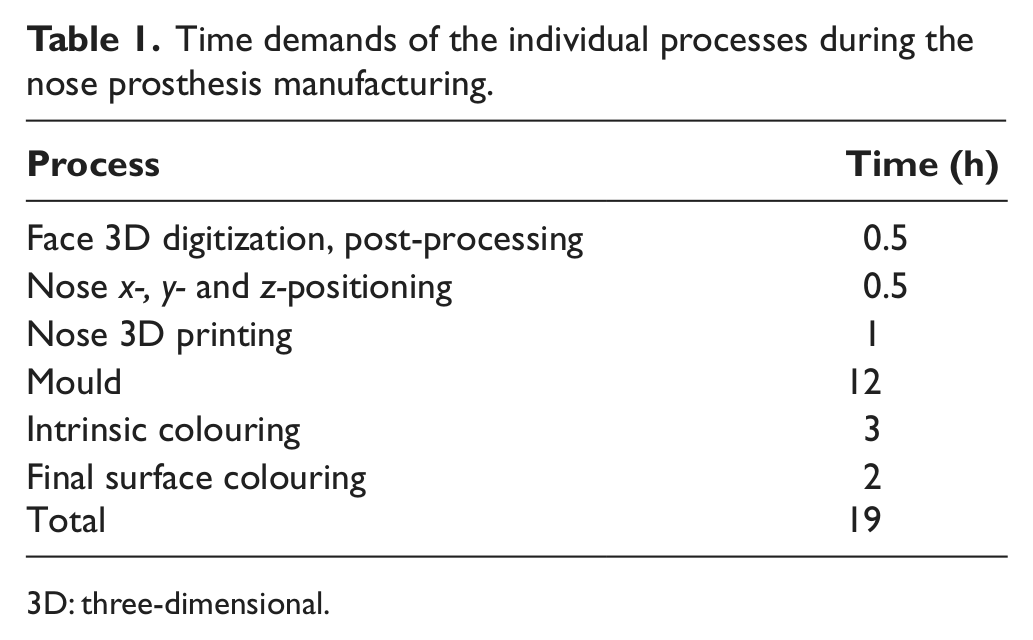
3D: three-dimensional.
The main benefit of methodology is the virtual fitting of a nasal prosthesis before manufacturing process. The team and a patient can evaluate shape, size and alignment of a nasal prosthesis on a face virtually in 3D visualization. That enables easy optimization of fitting process and leads to shortening the time of manufacturing and adjustments. From an economic point of view, the new manufacturing process is demanding, especially due to the purchase of digitization and manufacturing technologies. The process of obtaining digital data, its adjustment and preparation for production can be largely automated.
The described method represents an alternative to traditional ways of fabrication based on the manual sculpting of the model. The method is quite effective, although it requires equipment and computational skills of the CAD/CAM methods. This study verified the possibilities of advanced technologies and enabled the implementation of the process into clinical practice.
Footnotes
Acknowledgements
This work was completed in cooperation with the prosthetic workshop ING corporation, s.r.o. - Ortopedicka Protetika Frydek-Mistek, Frydek-Mistek.
Conflict of interests
None declared.
Funding
The work was supported by the research project ‘Application of Digital Technologies for Design, Manufacturing and Assessment of Custom-Made Orthotic and Prosthetic Devices’, no. FR-TI3/388; and by European Regional Development Fund in the framework of the research project NETME Centre under the Operational Programme Research and Development for Innovation. Registered no: CZ.1.05/2.1.00/01.0002, ID code: ED0002/01/01, project name: NETME Centre – New Technologies for Mechanical Engineering and Project of Specific Research FSI-S-11-30/1454.