
Abstract
Background:
Traumatic amputation of fingers results in a serious impairment of hand function and affects the psychological status of the patients. The implant-retained finger prostheses are an alternative treatment. The aim of this case report is to represent the use of osseointegrated implants for retention of finger prostheses in a patient with amputated thumb and index finger.
Case Description and Methods:
Dental implants were placed in the residual bone of the fingers using two-stage surgery. Custom-made attachments were used to provide retention between implants and silicone prostheses. Prosthetic fingernails were made of composite resin material.
Findings and Outcomes:
After 6 months, implants were clinically successful, and the patient was satisfied with the appearance and the function of the prostheses. The complications of broken prosthetic nail and mild discoloration were observed.
Conclusion:
Reconstruction of amputated fingers with implant-retained prosthesis is a worthwhile treatment providing esthetic, functional, and psychological benefits, although some complications might be experienced.
Clinical relevance
Implant-retained finger prostheses are an acceptable treatment modality for patients with amputated fingers. Evaluating implant prognosis, functional results and prosthetic results of the patients are necessary to address the benefits and complications of the treatment.
Background
A severe hand injury may impair the quality of life of the patients with physical, psychological, social, and economical consequences. 1 Several microsurgical techniques offer opportunities to reconstruct the lost digits. 2 Solitary digit transfer, bone lengthening, or ray transposition are the advent of surgical techniques for hand surgery that allow procedures for digit reconstruction to achieve their maximum potential in terms of function, predictability, and patient acceptance. 3 Most patients report satisfaction with the results of successful surgical reconstruction. 4 In some patients, however, surgical reconstruction is unsuccessful or contraindicated. In these patients, prosthesis can be mostly cosmetic with some functional benefit.3,5,6 Standard prosthetic digits that are made of silicone or acrylic resin are often unstable and lack sensibility. 7 Furthermore, the stump of the amputated finger should be minimally 1.5 cm in length to fit the standard digital prosthesis. 8
Osseointegration technique was originally described by Brånemark et al. 9 for oral rehabilitation of edentulous patients in the 1960s. Osseointegration principle has also been extended to extraoral rehabilitation in the late 1970s and used in the management of orbital, auricular, and nasal defects. 10 Lundborg et al. 5 then reported fixation of digital prostheses by osseointegrated implants. With this technique, the problem of instability of the prostheses for patients with short stumps on which a standard digital prosthesis is unable to fit properly has been avoided. Furthermore, the osseointegrated digital prosthesis can provide some level of tactile sensation to the patients. Osseointegrated implant makes perception of pressure and vibration possible, and sometimes also makes the patient able to identify textures and surfaces of various materials as running the prosthetic finger over them.7,11 Other reports revealed that the patients were able to perform daily manual activities such as writing with a pen, typing on computer, playing piano, and grasping objects.12,13 However, experience with the technique is limited in the literature. Clinical reports with follow-up times ranging from 6 months to 3 years revealed that osseointegrated implants anchoring finger prostheses successfully survived during these follow-up periods.5,6,9 Lundborg et al. 11 also reported a 13-year successful function of an implant in a patient with traumatic thumb amputation. Implant failures supporting finger prostheses have also been reported in the literature.7,14 Other concerns with osseointegrated finger prostheses are soft tissue health, prostheses longevity, and complications. Additional results on biological, prosthetic, functional, and esthetic outcomes of the treatment are needed. This case report gives an account of the use of osseointegrated implants for retention of finger prostheses in a patient with traumatic amputation of thumb and index finger and reports on biological and prosthetic results of the prostheses.
Case Description and Methods
A 15 year-old female patient who lost her right thumb and index finger presented for treatment. The patient had traumatic amputation of the fingers when she was 3 years old. The amputations occurred at the proximal phalanx of the thumb and the index finger. Preoperatively, the affected hand was evaluated radiographically for implantation. The required width and length of the implant were determined by measuring the width of the inner cortex and the length of the bone to the subchondral area in the radiograph, respectively. In the first stage of surgery, implants with 10 mm in length and 3.5 mm in diameter (IDcam M; IDI system, Paris, France) were placed in the proximal phalanx of the thumb and the index finger (Figure 1(a)). At the second stage of surgery, approximately 3 months later, the skin flaps were again raised and healing caps (Ref. 0213, IDI system) were attached to the implants. After a 2-week healing period, impression cylinders (Ref. 2004, IDI system) were secured on the implants and impressions were made of each abutment and stump using silicone impression material (Zetaplus; Zhermack SpA, Badia Polesine, Italy). Retentive attachments were designed to provide retention by frictional forces and rigid support for silicone prostheses as described in a previous report (Figure 1(b)). 12 Anti-rotationally secured burnout cylinders (Ref. 022601, IDI system) were used as wax patterns in the casting procedure of the attachments.
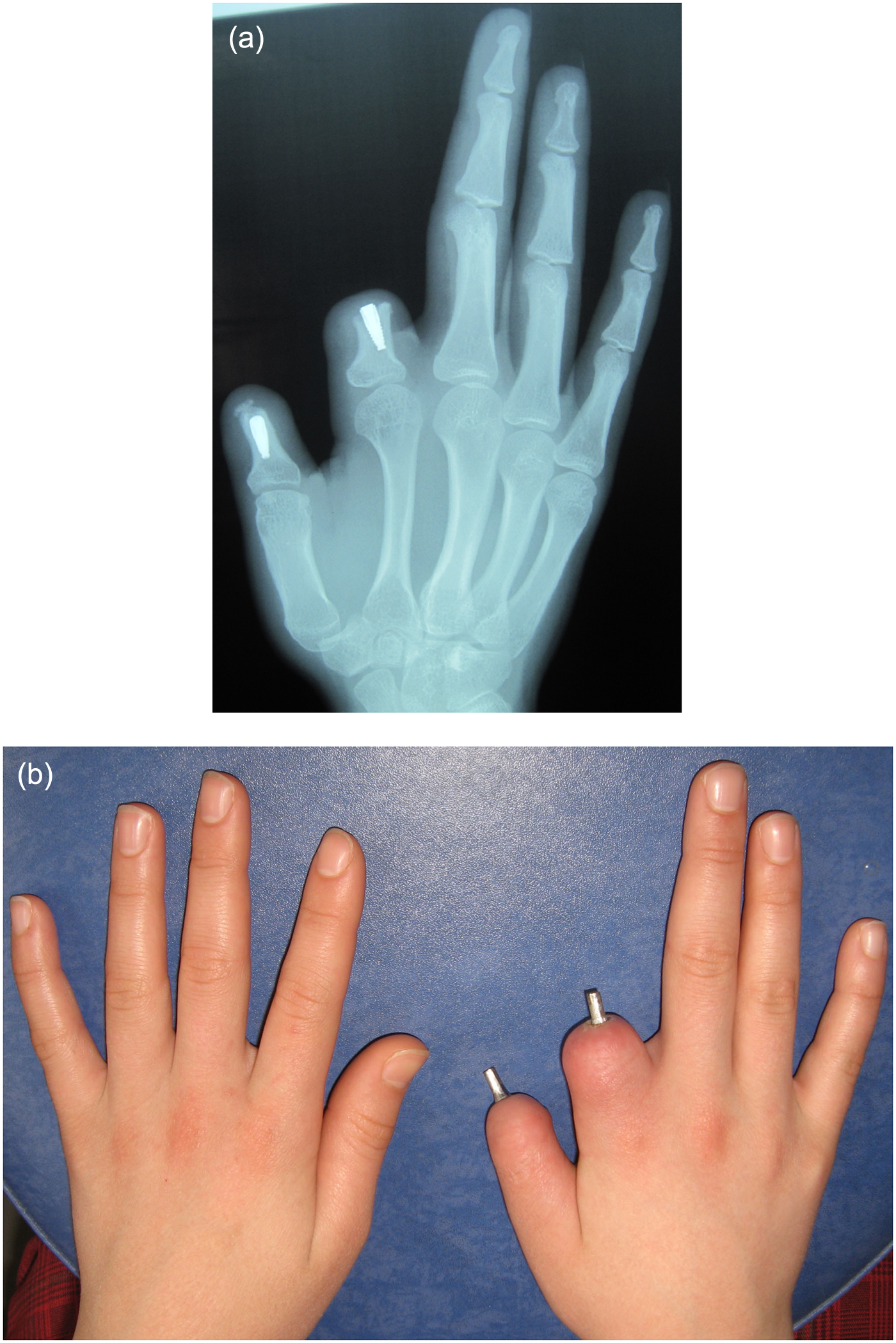
(a) Radiographic appearance of osseointegrated implants 3 months after surgery and (b) retentive attachments in place.
Wax patterns of the finger prostheses were generated by making impressions of contralateral digits of the patient with an irreversible hydrocolloid impression material (Hydrogum Soft; Zhermack SpA), and wax was poured into the negative molds to duplicate the lost fingers. The wax patterns were adapted on the casts including attachments. The size, shape, and contours of the wax patterns were evaluated on the patient (Figure 2(a)). The wax patterns were returned on the casts. The thickness of the portion of the stump casts that corresponds to prostheses margin was reduced by 0.5 mm to compensate stretching of the thin silicone edge and to provide continuous skin contact round the silicone margin. The wax was adapted and feathered on the reduced cast margin.
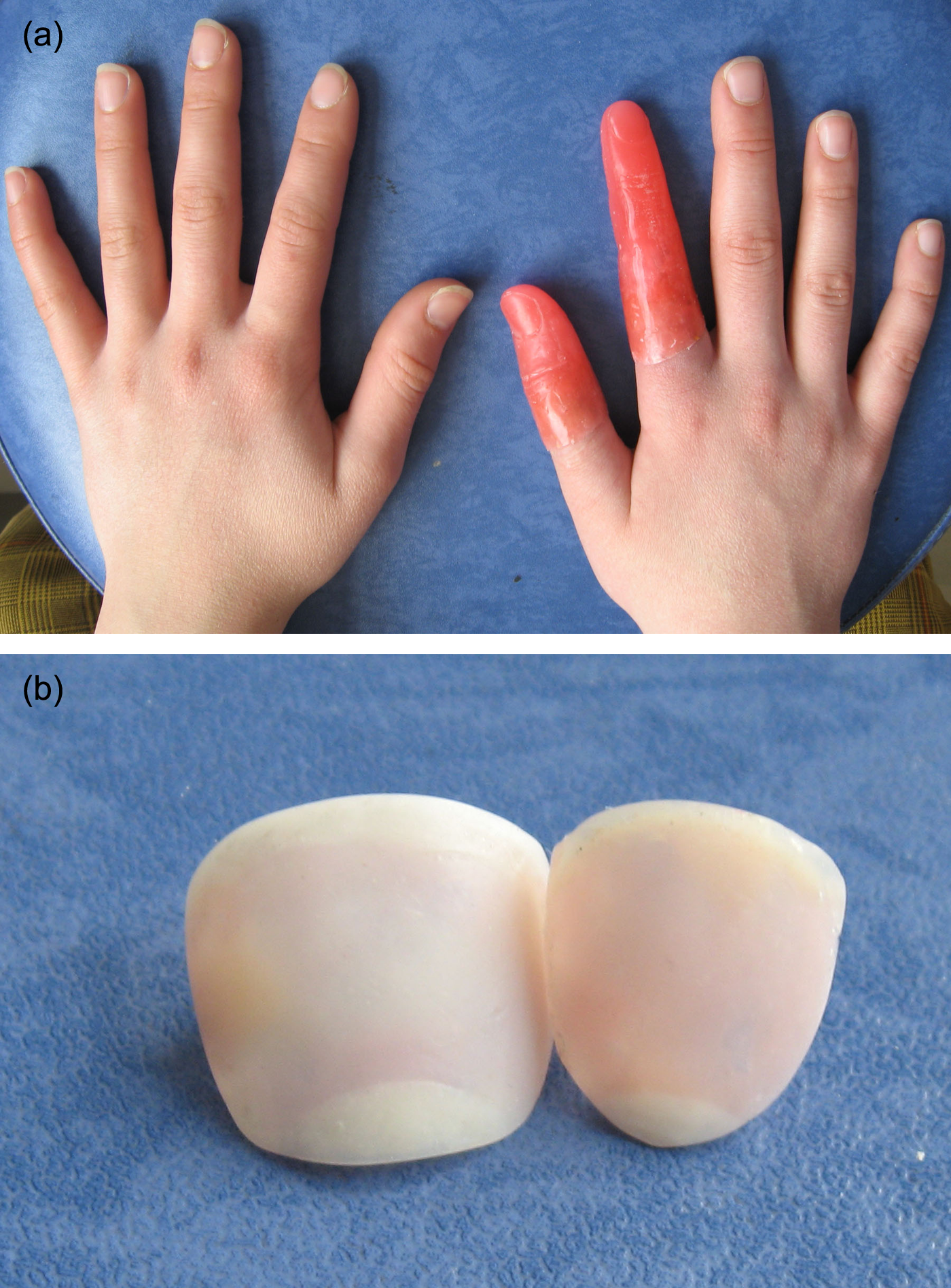
(a) Wax patterns in place and (b) custom-made composite resin fingernails.
The thickness of the wax nail beds was reduced to approximately 1–2 mm to create space for prosthetic nails. Undercut was created beneath the cuticle margins to retain the prosthetic nails within the final prostheses. Skin folds, wrinkles, and print patterns were made on wax patterns of the finger prostheses considering the contralateral digits of the patient. Individual stone molds were fabricated using the lost wax technique. 8 Finger prostheses were fabricated from high-strength heat curing silicone material (high-strength silicone rubber; Principality Medical Ltd, South Wales, UK), which was intrinsically pigmented. The substructures were cleaned with acetone, and silicone primer (Platinum primer; Principality Medical Ltd) was applied to the substructure in order to secure the acrylic resin substructure to the silicone prosthesis. The silicone was processed at 100°C for 1 h.
The impressions of the prepared nail bed of each silicone prostheses were made with irreversible hydrocolloid impression material and stone casts were obtained. The fingernails were made of composite resin material (Flow line SYR assortment; Heraeus Kulzer GmbH, Hanau, Germany), which was intrinsically colored to match the shades of the nails of the patient. The semitransparent composite resin material used for the fingernails of the patient was intrinsically pigmented using the intrinsic coloring agents of the composite material (Effect color RSY assortment; Heraeus Kulzer GmbH). Colored composites were inserted in appropriate places in the isolated stone casts of nail beds and cured using a light source. The composite resin nails (1–2 mm in thickness) were removed from the cast and polished with composite disks (Sof-Lex pop-on; 3M ESPE Dental Products, Seefeld, Germany) (Figure 2(b)).
The nail beds and prosthetic nails were cleaned with acetone. A low viscosity, room temperature curing silicone (Extrinsic sealant; Principality Medical Ltd) was applied to the nail beds of the prostheses. The nails were slid into the undercuts of the cuticles, and a light pressure was applied to remove excess material. The fit and shade of the finger prostheses were evaluated on the patient. Some minor extrinsic coloration was applied to some areas of the prostheses to enhance the color match between the prostheses and the tissues of the patient (Figure 3(a)). Instructions for home hygiene care were given to the patient when prosthesis was completed. These instructions included demonstration of mechanical debridement of crusting around the abutments with a soft bristle toothbrush and irrigation with warm water and soap. Recall examinations were performed 1 week and 3 and 6 months after the prostheses insertion, and arranged follow-up visits at every 6 months, unless some complications occurred sooner. Clinical and radiological assessments were performed. The patient was monitored in terms of implant success, health of peri-implant skin, frequency of use, function, appearance, and complications by a prosthodontist who did not participate in the fabrication of the prostheses. The patient provided written informed consent that the data can be used for scientific purposes.
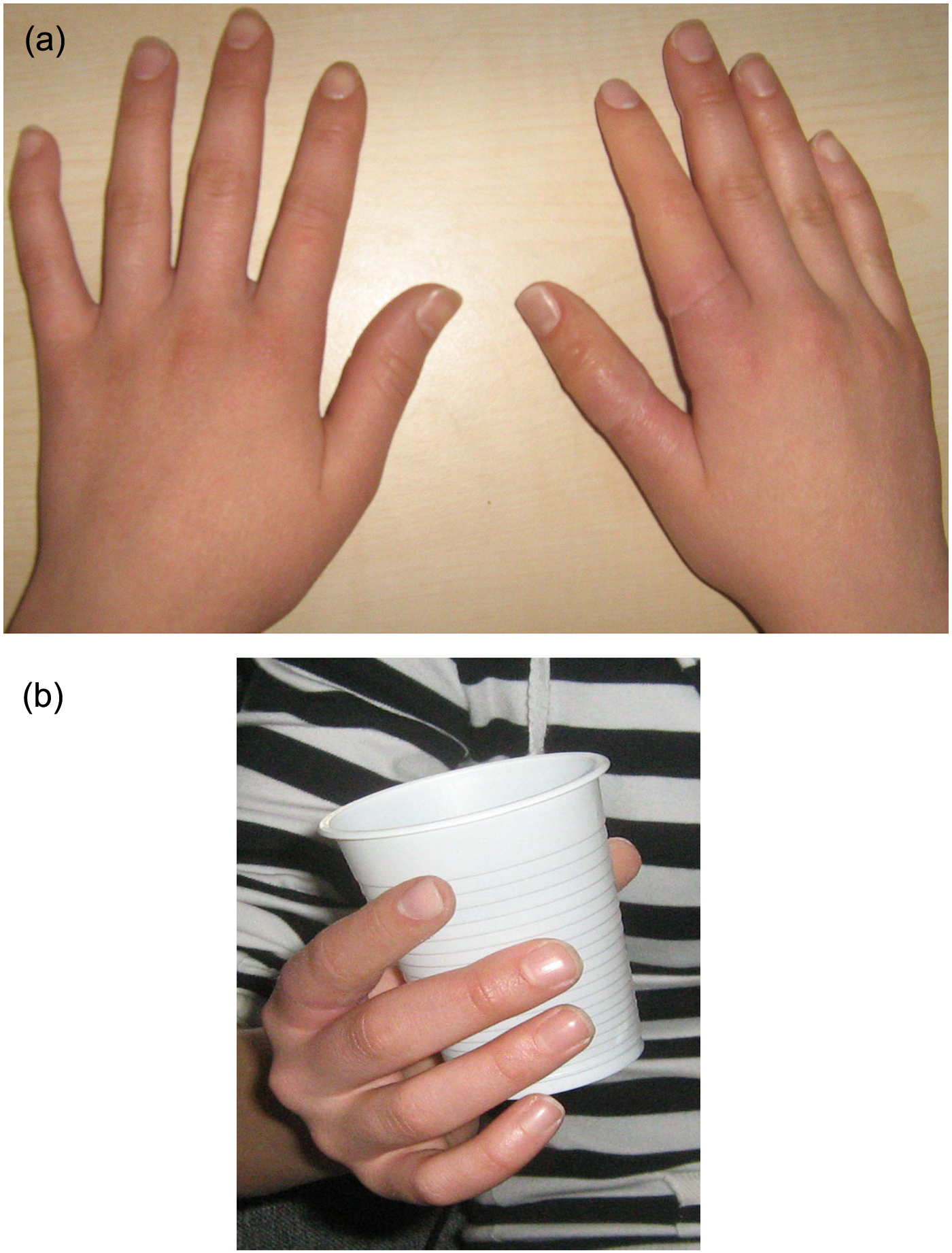
(a) Silicone prostheses in place and (b) osseointegrated silicone finger prostheses in function.
Findings and Outcomes
The duration of the follow-up period was 6 months. The implants were clinically and radiographically integrated in the bone as revealed by an absence of clinically detectable mobility and normal-looking bone trabeculae surrounding the implant during the follow-up period. Peri-implant skin showed no signs of infection.
The patient was very happy with the appearance and comfort of her prostheses and wore them most of the time. She reported that she wore the prostheses throughout the day except sleeping and having shower, which means that she wore them 14–16 h a day.
The patient was trained to use her hand as she had lost two fingers in her right hand when she was very young. Immediately after insertion of the osseointegrated finger prostheses, the patient began to use her right hand for picking up small objects (Figure 3(b)). At the 6-month examination, she demonstrated that she was able to perform various activities such as writing, picking up objects, brushing her hair, and applying make-up with her prosthetic fingers. The patient accepted the prostheses as a part of her body.
The complications experienced with the prostheses included broken prosthetic nail 5 months after the prostheses insertion and a mild level of discoloration observed at the 6-month control. Composite nail was refabricated and reapplied to the silicone prosthesis.
Discussion
Traumatic amputation of the digits results in dramatic impairment of hand function and esthetic.1,2 Traumatic amputation of a thumb particularly is a serious injury, as it removes the pole that can be opposed to the fingers. 11 Furthermore, thumb and index finger mediate collateral and precision grip, which are the two most important prehensile functions of the hand. Reconstruction of thumb and index finger, therefore, is highly important. Currently, many traumatically amputated digits can be saved by surgical replantation.4,5 As the surgical reconstruction techniques are generally the first choice for treating amputated digits, prosthetic treatment can be considered as an alternative reconstruction technique in unsalvageable cases or in cases of replantation failure.3,13–15 However, a more cautious approach is warranted for applying a prosthetic thumb for children, because thumb sensation is important at early ages for a proper development of brain, bimanual dexterity, and environment exploration. To ensure a successful rehabilitation process, rehabilitation team should take into consideration all influencing factors, such as functional, emotional, social, and professional profile and age of the patient. 2 The drawbacks of prosthetic reconstruction might be mitigated by using osseointegrated implants. A common experience is that placing an osseointegrated titanium implant within the intramedullary canal of the residual bone of the amputated stump provides a secure attachment for the prosthesis. Furthermore, the prosthesis can deliver some tactile sensation via osseointegrated implant.5–7,14 Lundborg et al. 11 made a sturdy to identify the mechanism of osseoperception, and they reported that the tactile stimuli applied to the prosthesis activated the primary somatosensory cortex of the brain.
This case report showed, in agreement with the previous reports, that osseointegrated finger prostheses provided a high degree of esthetic and functional improvement for a patient with amputated fingers.5,6,12–14 The follow-up of the patient, however, revealed that some technical complications related to prosthetic materials might arise and this possibility should be taken into account in choice of the treatment and maintenance.
Successful osseointegration and good prognosis have been reported for titanium implants used in the finger reconstruction5,6,13; however, failures are also reported in the literature.7,14 Doppen et al. 7 observed implant failure due to infection and Sierakowski et al. 14 reported a loosening of implant due to trauma. Heitmann and Levin, 3 however, argued that the major role played by thumb in the hand, especially in pinching and grasping, may cause an overload on the implant in the residual bone structure of the thumb. The lessons learned from the previous experiences might be useful in treatment planning and providing maintenance instructions to the patients. In the present case, the implants were immobile and radiographically no peri-implant bone loss was observed during 6 months after loading.
Peri-implant skin infection has been addressed with the skin-penetrating osseointegrated implants. 15 Manurangsee et al. 6 and Lundborg et al. 5 advocated trimming the skin surrounding the abutment to the same thickness as the split-thickness skin graft at the second-stage surgery; thereby, the skin is attached to the underlying cortical bone to minimize mobility. This is a similar technique applied to skin-penetrating implants in the maxillofacial region. 15 An alternative solution to this problem has been suggested by Doppen et al. 7 They suggested creating an epithelialized track into the screw cavity of the implant. They reported that they secured good peri-implant health using this technique. In the present case, peri-implant skin was trimmed as proposed by Lundborg et al. 5 and any soft tissue complication was not observed. Appropriate home care and rigorous hygiene applied by the patient are thought to be a contributing factor for the good soft tissue health.
Providing tactile sensation to an amputated stump is one of the major benefits of the osseointegrated finger prostheses. Functional improvements in patients soon after treatment with osseointegrated finger prostheses without any signs and symptoms of discomfort have been reported in the literature5–7 and the results of the present case report confirm these findings. Sierakowski et al. 14 also observed some degree of pain at bone-implant interface and cold intolerance in patients. However, these symptoms did not negatively affect implant survival and functional improvements. Further extensive studies are needed to objectively assess the improvements in hand function after treatment with osseointegrated finger prostheses.
For the success of an implant therapy in any part of the body, preventing prosthetic and technical complications are as important as osseointegration and biological responses. The broken prosthetic nail was a technical failure observed with the prosthesis. Composite resin material shows adequate strength in dental applications 16 ; therefore, the composite resin nail prostheses used in the therapy (1–2 mm in thickness) were not expected to fracture. The patient’s repeated application and removal of the nail polishes are thought to be responsible for this failure. Also, the discoloration of the silicone around the nails may be attributed to acetone containing nail polish removers. Composite nail was refabricated and reapplied to the silicone prosthesis and the patient was instructed for a careful use of nail polishes and removers.
Discoloration, which is attributed to the color change in elastomers and pigments over time, is a common problem limiting the life span of silicone extraoral maxillofacial prostheses. Other problems experienced in silicone prostheses are a decrease in quality of fit of prostheses at edges and a deterioration of the prostheses. 17 In the present case, physically improved silicone material fabricated for extremity prostheses was used. Any deterioration of the prostheses in the present case cannot be attributed to the properties of this material. However, a mild discoloration of the prostheses was observed after 6 months. Renewal prostheses would be fabricated after a significant discoloration. The estimated survival time for the silicone extraoral prostheses has been reported to be 1–1.5 years. 17 Discoloration of the silicone material is a multifactorial phenomenon and may be attributed to various factors such as material and pigment characteristics, personal habits, and environmental staining. Despite some improvements in biocompatibility and mechanical properties of medical grade silicones, the color degradation problem has not been resolved yet and the research is going on in this field.
Conclusion
Reconstruction of amputated fingers with implant-retained silicone prosthesis is a worthwhile treatment modality providing esthetic, functional, and psychological benefits to the patients, although some complications might be experienced.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.