
Abstract
Background:
Millions of people in low- and middle-income countries lack access to prosthetic care. A well-fitting, durable socket is important for prosthesis comfort and function, but conventional fabrication techniques require highly trained clinicians and specialized equipment.
Objectives:
To increase access to prosthetic care by developing a simple, low-cost socket fabrication method that does not require specialized equipment or electricity, and can be performed by persons with minimal prosthetic training.
Study Design:
Socket fabrication methods and socket function were evaluated in a pilot feasibility study.
Technique:
We describe a rapid method for fabricating a rigid foam socket directly over the residual limb, with a mass producible, strong, cosmetically appealing plastic outer shell. We fabricated sockets for four individuals with unilateral transradial amputations and evaluated socket function.
Results:
An individual with no formal prosthetic training was able to fabricate sockets and assemble a functional, comfortable prosthesis system within 90 min. All necessary supplies can be provided in a kit for under US$100.
Discussion:
Further work is required to determine durability, assess comfort, refine suspension methods, and to develop instructional materials.
Conclusions:
We developed a simplified, inexpensive method to fabricate sockets on the residual limb using expandable foam with an integrated cosmetic/structural covering (i.e. an exoskeletal system), for persons with transradial amputation. A transradial prosthesis socket can be fabricated in around 90 min. and all necessary materials, tools, and written instructions for fabrication and fitting can be provided in a kit. Specialized equipment and electricity are not required. Instructions for fabrication and fitting can be provided in multiple languages using online videos.
Keywords
Background
Millions of people with amputations in low- and middle-income countries (LMICs) lack access to prosthetic devices.1,2 The cost of prosthetic devices is high relative to income in these countries, and necessary equipment and trained clinicians are often unavailable. 3
The socket is an essential component of a prosthetic system, affecting stability, comfort, range of motion, and cosmesis. 4 Sockets are typically custom made by prosthetists with advanced training—and require time, expertise, and specialized equipment. However, in LMICs, an estimated 40,000 prosthetists/orthotists are needed, but only 400 are trained each year. 1 Required equipment 5 or reliable electricity are also often unavailable, 6 and travel to and from an established clinic may be prohibitive in terms of distance and cost. 3 Reducing the complexity of materials, procedures, and fitting time required for socket fabrication may increase access to care.
Several attempts have been made to simplify socket fabrication for people in LMICs. The OpenSocket (Bump, Champaign, IL) allows rapid fitting but lacks a cosmetically appealing cover. 7 Computer-aided design and computer-aided manufacturing (CAD/CAM) systems can digitally capture and model the shape of the residual limb, allowing three-dimensional (3D) printing of sockets, but computers, 3D printers, and electricity are required. 8 The Center for International Rehabilitation (CIR) technique 9 uses sand or small beads instead of plaster of Paris, reducing mold costs and fabrication times. However, like the International Committee of the Red Cross (ICRC) polypropylene socket,10,11 the CIR approach requires an oven, vacuum pump, electricity, and trained clinicians.
We developed a rapid socket fitting protocol (Table 1) using a mass-producible outer socket shell and expandable rigid foam. Four individuals with unilateral transradial amputations were fit by a staff engineer with no formal prosthetic training. This technical note describes our method and presents results from initial functional evaluation of these sockets.
Criteria for socket fabrication method.

Technique
Socket fabrication materials
The socket shell, which forms the outer structure of the socket (including the forearm) (Figure 1), was designed in SolidWorks (Dassault Systèmes SolidWorks Corporation, Waltham, MA, USA), using 25th to 95th percentile male arm circumference values for the wrist, forearm, and elbow and the length 12 to create a composite 3D arm envelope that can be cut to fit a wide range of people. Prototype shells were 3D-printed (Stratasys uPrint SE Plus, Eden Prairie, MN, USA) in acrylonitrile butadiene styrene (ABS; 0.254 mm), which allowed for iterative design and rapid fabrication.
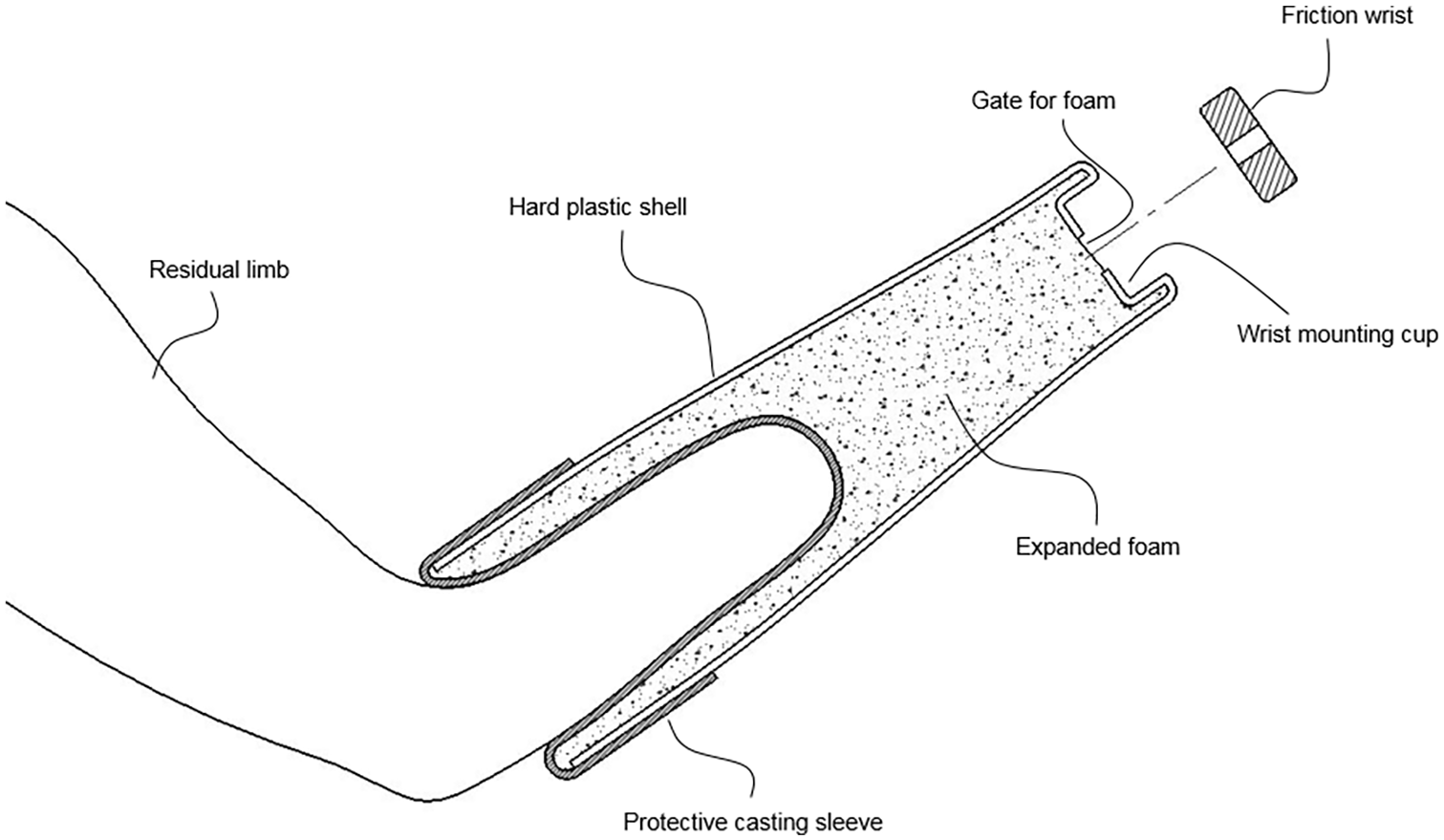
Diagram of low-cost socket fabrication method.
The socket was formed directly on the residual limb, using expandable polyurethane rigid foam (Foam IT 8, Smooth On Inc., Macungie, PA, USA), which was poured between the residual limb and the outer plastic shell. The foam is produced by mixing two pre-measured resins, which then expand to several times their original volume and cure to touch in 20 min. Once cured, the foam resembles a low-density solid plastic, which can be modified with simple hand tools (e.g. sanded to relieve pressure). Resins are packaged in dual chamber pouches (see Figure 2(b)) that allow for easy distribution, accurate mixing, and quick dispensing. 13
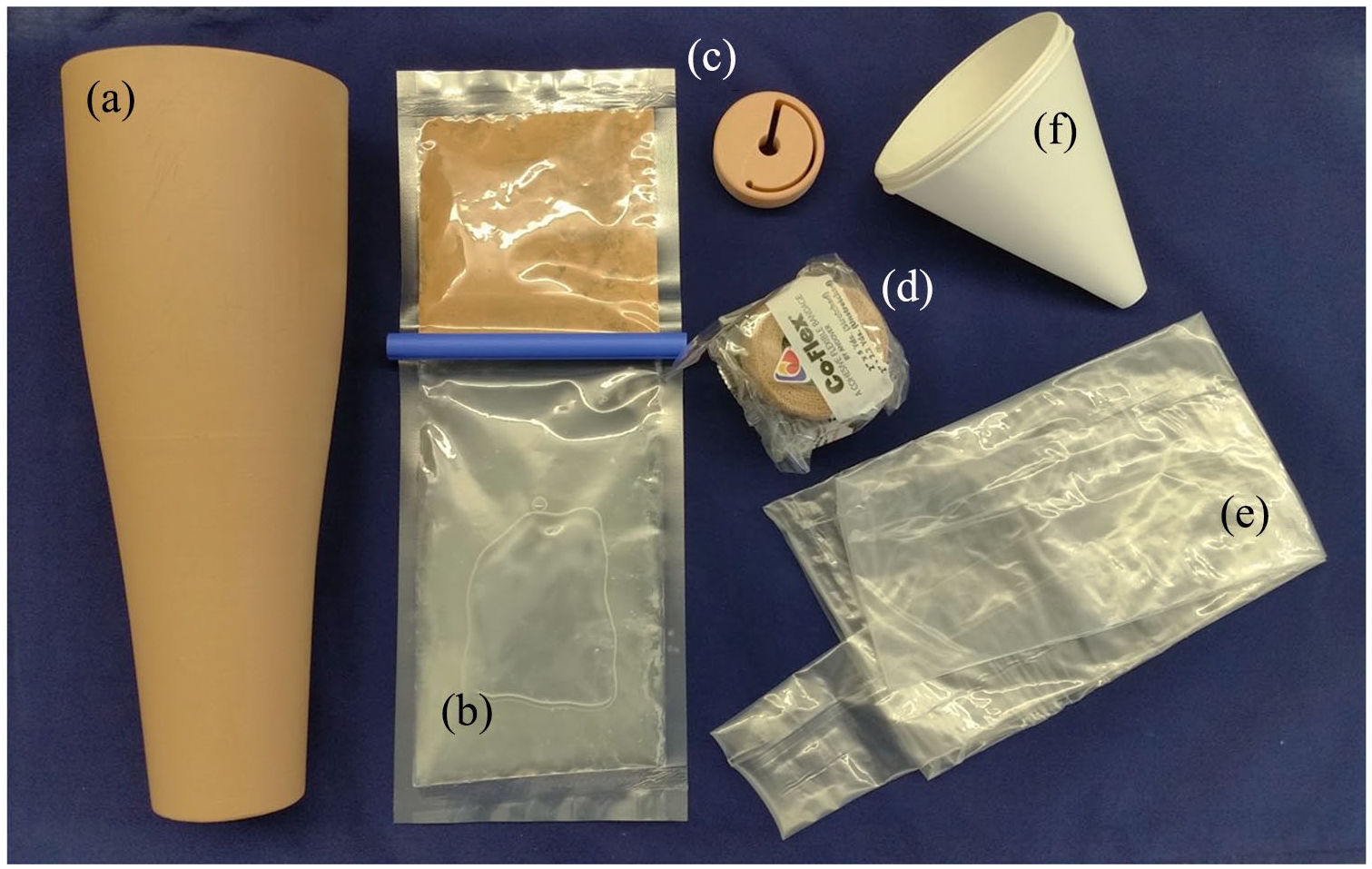
Socket fabrication kit: (a) limb-shaped hard plastic outer shell (three-dimensional (3D)-printed prototype, painted to approximate skin color), (b) polyurethane foam resin packaged in a dual chamber pouch, (c) 3D-printed model of the one-piece friction wrist, (d) self-adherent wrap to seal the protective sleeve over the shell, (e) protective sleeve or gel sheath, and (f) funnel for guiding foam resin into the mold.
A two-part polyurethane coating (Smooth-Cast 57D, Smooth On Inc., Macungie, PA, USA) was applied over the interior surface to seal the inner surface of the foam, reduce friction, and improve aesthetics.
A reusable gel sheath (ALPS Skin Reliever Gel Sheath, St. Petersburg, FL, USA) (Figures 1 and 2(e)) was used to protect the residual limb from heat generated by the exothermic curing of the foam and to prevent the foam from adhering to the skin.
Socket fabrication procedure
The shell was cut to length with a customary U-shaped trimline at the cubital fold. The gel sheath was donned and the outer shell positioned over the limb. The proximal edge of the sheath was then folded back over the shell (Figures 1 and 2(a)) and sealed using self-adhesive wrap (Figure 2(d)). The shell could touch the residual limb but not fit so tightly that the flow of foam around the residual limb would be obstructed. The foam resins were mixed, then poured through the opening (gate) at the distal end of the shell (Figure 1). The shell was held in place on the arm as the foam expanded to capture the shape of the limb, forming a smooth interface, and bonded with the outer shell, which was incorporated into the final socket. The gate functioned as an escape valve to contain the flow of expanding foam and to create backpressure to ensure that foam filled all space between the limb and outer shell. Terminal devices with standard ½”-20 threads were attached to the socket using a one-piece 3D-printed prototype friction wrist (Figure 2(c)).
Socket evaluation
Sockets were fitted to four male individuals with unilateral transradial-level upper limb amputation, recruited as a convenience sample for this pilot feasibility study (inclusion criteria: regular prosthesis use, no open wounds, skin conditions, or other injury to the residual limb). Subjects had a range of residual limb lengths and shapes, including one wrist disarticulation (Table 2). All subjects gave written informed consent to participate in this study. An engineer with no formal prosthetic training performed each socket fitting under the supervision of a certified prosthetist. A voluntary open hook and a figure-of-eight, body-powered harness with flexible hinges (Fillauer, Chattanooga, TN, USA) was attached to each prosthesis. Prosthetic socks were used to adjust the fit. Completed sockets were evaluated by a certified prosthetist, based on sock ply fit, subjective comfort, and participants’ ability to perform the box and block test. 14
Socket fitting and evaluation.
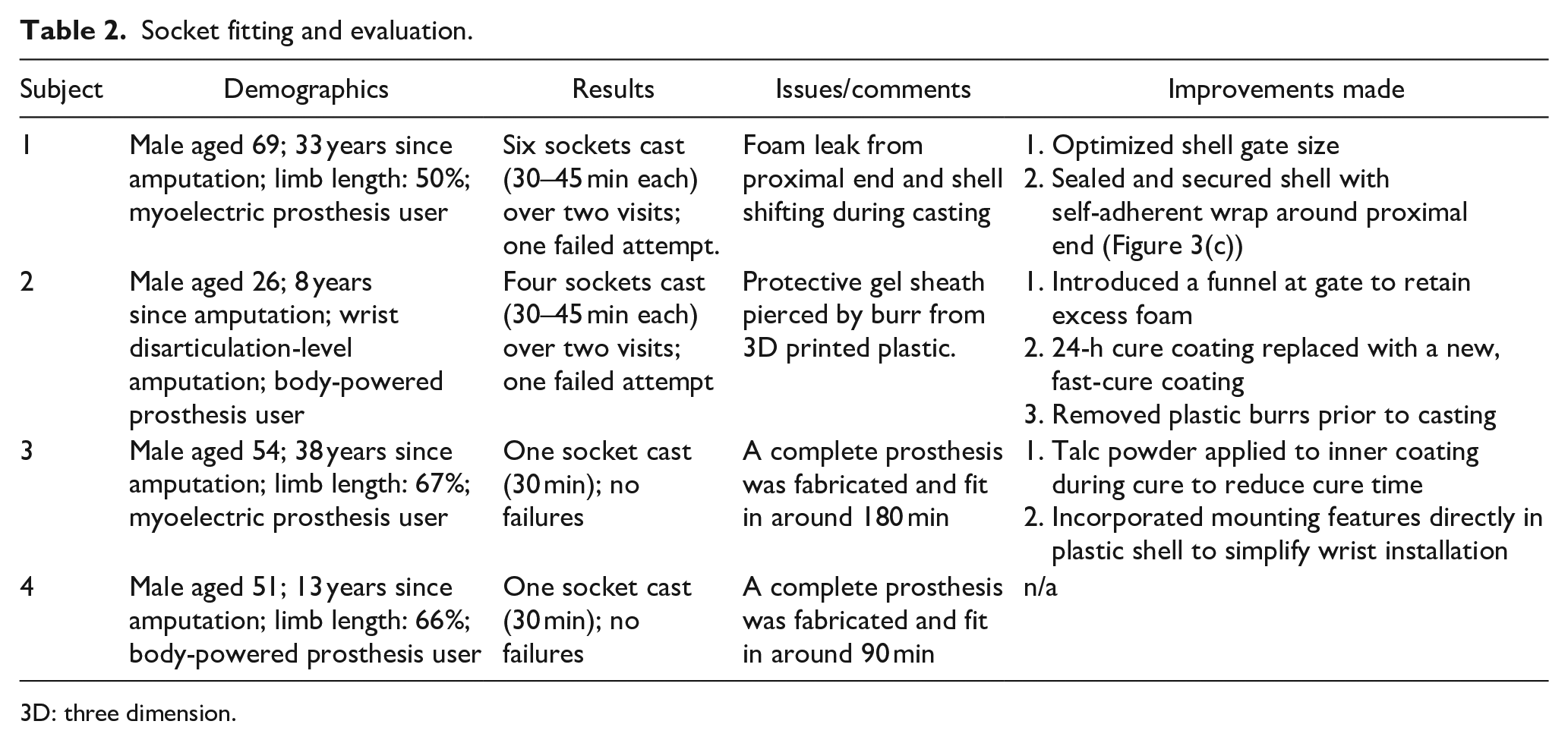
3D: three dimension.
Results
All four subjects were successfully fitted. Results from each fitting were used to optimize the method. Early fittings focused on troubleshooting and modifying the socket design and fitting protocol accordingly. Subsequent fittings progressed to reducing fabrication time, downtime, and number of steps (Table 2). The final subject was fit with a complete system (socket, harness, and terminal device) in less than 2 h. Although the foam reached temperatures of above 65.5°C during curing; the skin surface temperature only reached 43°C, which subjects found comfortable. The average weight of the socket and wrist was 329 g (N = 4, standard deviation (SD) = 8.2).
All subjects achieved a comfortable fit with a three-ply sock, which is clinically appropriate. Each was able to perform basic tasks such as picking up common household objects and performing the box and block test. 14 Subjects were queried about comfort throughout approximately 1 h of use and none reported socket discomfort. Complaints were limited to the harness, as not all subjects were used to a figure-of-eight harness with a body-powered device. No other issues or limitations were noted (Figure 3).
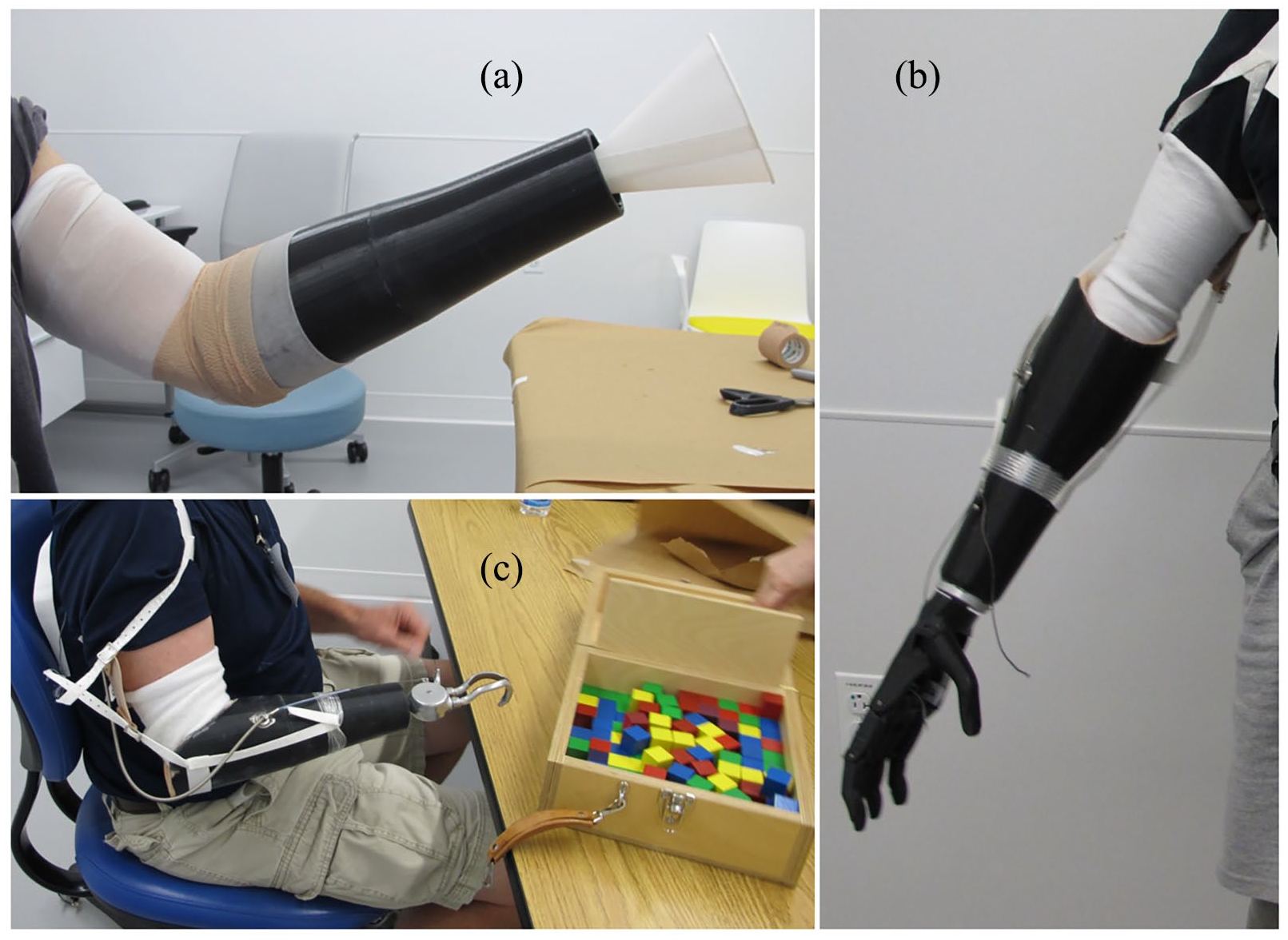
(a) Casting the socket: The protective sheath is placed over the residual limb, and a plastic shell is placed over the limb. A cavity is created for the foam by folding the protective sleeve over the proximal end of the shell and sealing with self-adherent wrap. Foam is poured into the distal opening (gate) through a paper funnel and expands up and out to fill in the shell around the residual limb. (b) A socket, complete with trim lines and interior coating, harnessing, and a three-dimensional (3D)-printed body-powered hand. (c) Subject performing box and block task with completed prosthesis.
Discussion
We demonstrate an innovative simple socket fabrication method that eliminates the need to create a plaster wrap/cast and thermoform/laminate a socket and forearm. Sockets were fabricated by an engineer without clinical training and without special equipment or resources—including electricity.
This is not the first direct socket fabrication method proposed. The IceX System (Ossur, Iceland) was originally presented as a fabrication system on the residual limb, 11 and other low-cost systems are noted in the literature,9,15,16 such as the widely used polypropylene systems from the ICRC, introduced in 1988. Our method allows rapid fabrication of a functional, aesthetic socket at very low cost, using materials—including a terminal device and harnessing system—that can be provided in an easily-distributed kit, which may be a practical option in LMICs. Eliminating the need for expensive ovens or lamination systems for socket fabrication would allow use of the kit in rural locations.
The outer shell can be mass-produced using durable, inexpensive, injection molding techniques, allowing for a variety of skin colors and a realistic texture. Mounting features (e.g. for the cable and other hardware) can be incorporated directly into the shell. The shell can be cut to the correct length, thus one or two shell sizes would fit most individuals. 12 Rigid foams, used to form the inner socket, are inexpensive, relatively easy to use, and can expand to almost any shape. They are often used for reinforcement, improving stiffness and impact resistance with minimal additional weight. 17
The current cost of a kit (excluding harness and terminal device) is approximately US$100. Manufacturing the outer shell by injection molding will significantly reduce volume costs. Together with other refinements (e.g. a lower cost alternative to the gel sheath), we anticipate that kit costs could be reduced to below US$50.
In preliminary in-lab testing, the sockets performed well and were comfortable during in-lab use. Although perhaps not as durable as traditionally fabricated, custom systems, this simple, low-cost socket fabrication method could fill the unmet need of millions of people in LMICs with upper limb amputation.
Further studies are needed to test our system in LMIC settings to evaluate long term socket comfort, durability, and performance; to develop a low-cost harness or self-suspending socket; and to evaluate implementation of this system by individuals with less training (e.g. International Society for Prosthetics and Orthotics (ISPO) personnel categories II and III 1 ). Additional work is needed to develop instructional materials in an appropriate format that overcomes language barriers, for example, a pictorial fabrication manual or online videos that could be narrated in different languages. Such materials should include information on fabrication, fitting, and basic training in prosthesis use. Fabrication of transtibial sockets may also be possible using this method; however, for weight-bearing use, more research on socket integrity, suspension, and alignment would be required.
Conclusions
A simplified, inexpensive method has been presented for socket fabrication on the residual limb, using expandable foam with an integrated cosmetic/structural covering (i.e. an exo-skeletal system), for persons with transradial amputation. The socket can be fabricated in around 90 minutes and the fabrication materials, including all materials and tools as well as printed instructions, can be provided in kit form. With this technique, specialized equipment and electricity are not required. Instructional materials for fabrication and fitting can also be provided in multiple languages using online videos.
Footnotes
Acknowledgements
The authors thank Dr Ann Barlow for assistance with editing and refinement of the article and Ms Malaka Graci Finco, CPO, for assisting and supervising in the fabrication of the test systems.
Author Contributions
All authors contributed equally in the preparation of this article.
Ethics Review and Approval
Study procedures were approved by the Northwestern University IRB (Approval No. STU00023480).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this article were developed through a generous donation from the Bohnen Foundation and under grants from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR Grant Nos. 90RE5014 (2013–2028) and 90REGE0003 (2018–2023). NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this article do not necessarily represent the policy of NIDILRR, ACL, or HHS, and one should not assume endorsement by the Federal Government.