
Abstract
Background and aim:
Turning is an inherent problem in all lower limb amputees and more so in older dysvascular amputees. This study aimed to compare the turning performance of dysvascular amputees with that of the traumatic amputees.
Technique:
Six dysvascular transtibial amputees (69.83 ± 6.3 years) and six traumatic transtibial amputees (68.3 ± 6.6 years) completed the Step Quick Turn test of the NeuroCom® Balance Master and the Timed Up and Go Test. The measures used for comparison were as follows: turn time and turn sway of Step Quick Turn test, turning 180° to both the prosthetic and sound side and time taken to complete the Timed Up and Go Test.
Discussion:
The Mann–Whitney U test demonstrated a significant difference (p < 0.05) between the dysvascular and traumatic groups in turn sway to the prosthetic (70.7 ± 14.2 and 43.3 ± 9.7) and sound sides (72.5 ± 16.1 and 43.5 ± 8.2). Similar results were observed in turn time to the prosthetic (4.1 ± 1.4 and 1.7 ± 0.46) and sound sides (4.0 ± 1.3 and 2.1 ± 0.5). No significant difference was observed for the Timed Up and Go Test.
Clinical relevance
The observed differences suggest that dysvascular amputees are less able to adapt to the challenges associated with turning. More attention is required in the rehabilitation of dysvascular amputees in turning tasks particularly towards the prosthetic side.
Background and aim
Turning is an inherent problem in all persons with a lower limb amputation 1 affecting their quality of life. Persons with a dysvascular amputation (DA) face additional demands due to their compromised neuro-vascular function, 2 which may potentially lead to a fall during activities of daily living. Clinical observations suggest that persons with a DA have compromised balance ability and have difficulty in the execution of functional activities when compared to persons with a traumatic amputation (TA).
Few investigations on persons with DA corroborate these observations using clinical measures of gait and balance;3,4 however, these measures are inadequate to explain the nature of impairment. More recently, the Step Quick Turn (SQT) test measures of the NeuroCom® Balance Master (BM) have shown acceptable reliability and concurrent validity in persons with transtibial amputation. 5 Similarly, the Timed Up and Go Test (TUG), which is traditionally used in a clinical scenario has also been recently recommended as a measure of turning in other clinical populations. 6 Therefore, the aim of this exploratory study is to compare the turning performance of persons with a TA with that of the persons with a DA, using the SQT and the TUG.
Technique
Participants
A total of 12 male and female participants with transtibial amputation (dysvascular (n = 6) and traumatic (n = 6)) participated in the study. The mean age ± standard deviation (SD) of the participants of the DA and TA groups were 69.83 ± 6.3 years and 68.33 ± 6.6 years, respectively. Participants were recruited from the regional artificial limb centre, and all participants were able to walk 500 m without any supportive aids. Participants were free from residual limb issues such as open wounds and constant phantom limb pain and none of the participants had known vestibular problems and cognitive impairment. The mean ± SD time since amputation of the DA and TA groups were 4.6 ± 4.3 and 20.7 ± 18.3 years, respectively. The study was approved by the University of Otago Human Ethics Committee, and written informed consent was provided by all participants prior to participation.
Tests and measures
The SQT required the participants to stand at one end of the NeuroCom® BM force platform and on cue, take a step forward, turn 180° and then return to the starting position (Figure 1). The two variables generated by the NeuroCom software package utilised to quantify the turning performance were turn time (TT) and turn sway (TS). The TT is the time (in seconds) taken to complete an 180° turn, while TS demonstrates the sway (in degrees) exhibited by the subject during the 180° turn. These measures have been explained in detail elsewhere. 5 The TUG (in seconds) was also used as an adjunct measure for comparison.

Step Quick Turn test of the NeuroCom Balance Master.
Procedure
All participants signed a written consent and completed a self-reported questionnaire to screen their eligibility to participate in the study. The participants also completed the Locomotor Capability Index (LCI) as a measure of their self-perceived mobility capability. Participants then completed two trials of the TUG and three trials of SQT, turning to the sound and the prosthetic sides. The order of side of turning in the SQT was randomised.
For the SQT, all participants stood at one end of the BM force platform and on cue, took a step forward, turned 180° and returned to the starting position. When turning to the prosthetic side, the lead step was taken with the sound limb and vice versa for turning towards the sound side. The trial was repeated when the participants failed to complete the test as required, and all participants were instructed to perform the test ‘as quickly as possible’. The TUG performed by the participants sequentially included getting up from an arm and back rest chair, free style walking along a marked 3 m distance, 180° turn, walking back 3 m distance, turn 180° and sitting on the chair.
Statistical analysis
The Mann–Whitney U test (z statistic) was used to compare the means of two trials of the TUG, three trials of the turn time to the prosthetic (TTP) and sound side (TTS) and three trials of the turn sway to the prosthetic (TSP) and sound side (TSS). The alpha level of p < 0.05 was used to determine the statistical significance. As the study included a small sample in each group, the effect size was also estimated to determine the strength of the findings. An effect size of ≥0.30 is regarded as an acceptable magnitude of observed effect. 7
Results
The descriptive statistics for TT and TS (to the sound and prosthetic) of the groups and the results of the Mann–Whitney U comparisons are detailed in Table 1. The mean TT (seconds) and TS (in degrees per second) were higher for the DA group than for the TA group. The Mann–Whitney U test demonstrated significant difference between the groups for all measures (TTP, TTS, TSP, and TSS) with the effect size ranging between 0.74 and 0.79 (Table 1). No statistical difference was demonstrated between the two groups for the TUG.
Mean (SD) and Mann–Whitney U test results for the main measures.
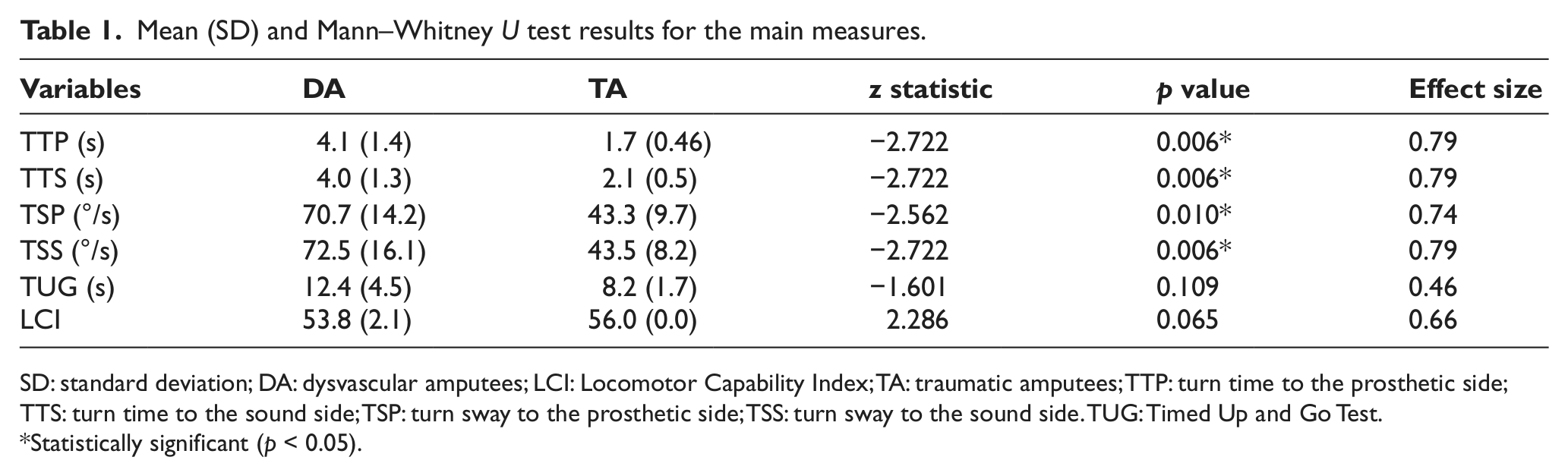
SD: standard deviation; DA: dysvascular amputees; LCI: Locomotor Capability Index; TA: traumatic amputees; TTP: turn time to the prosthetic side; TTS: turn time to the sound side; TSP: turn sway to the prosthetic side; TSS: turn sway to the sound side. TUG: Timed Up and Go Test.
Statistically significant (p < 0.05).
Discussion
The purpose of this exploratory study was to compare the turning performance between persons with a TA and those with a DA as measured by the SQT and the TUG. The results demonstrated a statistically significant difference between the groups in the TT and TS measures of the SQT, to both sound and prosthetic sides, but not in the TUG, which included other movement components in addition to turning. The TS is the measure of sway exhibited by the individual’s support leg of the turning side, while the TT is the time taken to complete the 180° turn. The DA group took a longer time to execute the 180° turn and also demonstrated a greater magnitude of sway in comparison to the TA group, when turning in both directions.
The complex task of turning demands a change in the direction of the centre of mass progression without compromising stability and therefore requires a high neuromuscular control to maintain the centre of gravity within the base of support. 8 Although the differences observed in the SQT measures of this study do not necessarily imply that the persons with a DA are compromised in their turning performance, it does suggest that there might have been some difference in the strategies of turning as a compensatory mechanism.
Commonly different types of strategies have been explained to exist while performing a turning task or when changing directions.8–10 However, the two major components that can occur in different combinations are the trunk yaw and the weight acceptance. By and large, lower limb amputees are limited in their ability to transfer weight to the prosthetic limb due to various factors such as the weight acceptance ability and torsional force required at the knee joint for any turning manoeuvre. Able-bodied older adults generally exhibit limited trunk yaw and also use a different strategy to overcome this limitation.10–12 These instinctively suggest that older adults with an amputation will effectively be limited in their turning ability, and this may potentially lead to a stumble and/or a fall.
The compromised neuromuscular function/control in persons with a DA may have led to increased sway and fear of falling, which in turn is reflected as increased TT. Although the differences in experience with the prosthesis between the groups (range = 0.75–11.0 years in DA and range = 0.5–44.0 years in TA) might be one of the reasons underlying the differences observed, this difference was not exhibited in the TUG. The additional elements in the TUG, other than turning, such as getting up from the chair, walking and sitting down on the chair may have impacted the overall score of TUG leading to no statistical difference between the groups. However, further work is required to confirm this speculation.
To the authors’ knowledge, this is the first investigation to demonstrate turning performance in persons with DA using objective and detailed measures of turning. Although the variables of the SQT were clearly defined by the NeuroCom® Clinical Operations Guide, the precise estimation of each of the variables was unclear, which is a limitation of the study. Future investigations should determine the strategies of turning performance in persons with DA so as to understand and tailor their rehabilitation needs accordingly.
Key points
Persons with dysvascular amputation are less able to cope with the movement attributes underpinning the task of turning when compared with persons with a TA.
The results suggest that more attention is required in the rehabilitation of dysvascular amputees in turning tasks particularly to the prosthetic side. The TUG may not necessarily detect the differences in turning performance between the DA and TA sub-groups.
Footnotes
Acknowledgements
We thank the Dunedin Artificial Limb Centre staff who assisted in recruitment of participants for the study. We also thank all participants involved in the study.
Conflict of interests
The authors declare that there are no conflicts of interest.
Funding
This work was supported by the New Zealand Artificial Limb Board, Wellington (Grant number PL10674001PLX).