
Abstract
The purpose of the study was to describe the demographics, the causes of amputations, the amputation levels, the clinical outcomes, the durability of prostheses in unilateral lower limb amputee among workers entitled to non-state related work insurance, the ACHS, Chile, between 1974 and 2001. It was a retrospective descriptive study based on selected clinical files. One hundred files, with the minimal data required, were selected with a diagnosis of traumatic lower limb amputation, the levels ranging from Boyd's foot amputation to hip disarticulation, as defined by the Occupational Accidents Act from 1974 to December 2001. The mean age was 35.5 years, 96% were males, with an average follow-up of 7.7 years. In 50% of the cases the education level did not exceed elementary school. Ninety-eight percent were blue collar workers. The traumatic injury resulting in amputation took place during work in 89% of the cases the main causes being crushing injury (50%), traffic accident (19%), run over by car (14%) and burns (6%). The most common amputation levels were trans-femoral (40%) and trans-tibial (47%). Amputations were performed within the first 24 h in 49% of the cases. The hospitalization stay reached 8 weeks in 56.7%. Early complications were dehiscence (9.4%), superficial infection, (14.6%) and deep infection (26%). Late complications detected were soft tissue lesions (34.1%), exostosis (3.6%), painful neuroma (12.5%) and phantom limb pain (12.5%). Prostheses durability was on average 3 years. The average period to resume work was 1 year for 60% of the cases.
Introduction
Most of lower limb amputees within the general population are older than 50 years and the amputation is predominantly secondary to complications of chronic diseases such as diabetes mellitus and chronic obstructive arterial disease (Gittler 2002). Amputations secondary to trauma are a considerably smaller proportion and account for 5% of all amputations according to studies carried out in population groups outside Chile (Ebskov 1994; Christensen 1976). In Chile there are no statistics concerning this situation, however, the clinical hospital experience points to similar facts (Promis 2002).
Lower limb amputees attending the Hospital del Trabajador of the ACHS (Asociación Chilena de Seguridad) are actively working persons, usually healthy, with a traumatic amputation secondary to an occupational accident occurring either at the workplace or during their journey to and from work.
A worker suffering an accident is provided complete care at the ACHS from the first episode of emergency care to final discharge, including rehabilitation and all the special treatments required for the eventual sequelae for the rest of his/her life.
Thus, it has been possible for almost 30 years to follow the slow growth of this population consisting of patients with major sequelae being treated at the Rehabilitation Unit of the Hospital. These persons experience a permanent deficit with functional restrictions for the rest of their lives, which makes a significant impact on their quality of life and their working capacity.
In such cases, it is expected that an adequate medical-surgical therapy and a complete rehabilitation scheme will contribute greatly in order to regain function and to attain a satisfactory social and occupational reinstatement, to a better level than expected for chronic disease-related amputees.
The present study was carried out with the aim of knowing the demographics, clinical, functional and psycho-social aspects of the lower limb amputee population under study during a period of rehabilitation and follow-up of at least 6 months since amputation.
In view of the large amount of data available, the present study was divided in three segments:
Demographic aspects and global evolution until discharge
Functional aspects
Psycho-social aspects.
The present work corresponds to item 1.
Materials and methods
All clinical cases with a diagnosis of traumatic amputation of the lower limb, as described by the Occupational Accidents Act, during the period 1974 to December 2001 were selected from the database of the Hospital del Trabajador of Santiago, Chile. They included all levels of lower limb amputation from Boyd's foot amputation to hip disarticulation. Altogether there were a total of 149 cases. All the patients were survivors of the accident and were referred to the hospital from different parts of the country.
For the detailed data analysis, 49 cases were excluded: 10 cases had bilateral lower limb amputation, one with a hemipelvectomy and 38 cases with incomplete clinical files.
The remaining 100 clinical files were retrospectively evaluated, and data regarding demographic variables, the type of accident, the period of time elapsed between the accident and the amputation, the length of hospital stay, complications, the follow-up and the durability of the prosthesis were collected.
Results
The mean age of patients was 35.5 years with a range between 17 and 63 years. Distribution according to gender showed a male predominance of 96%.
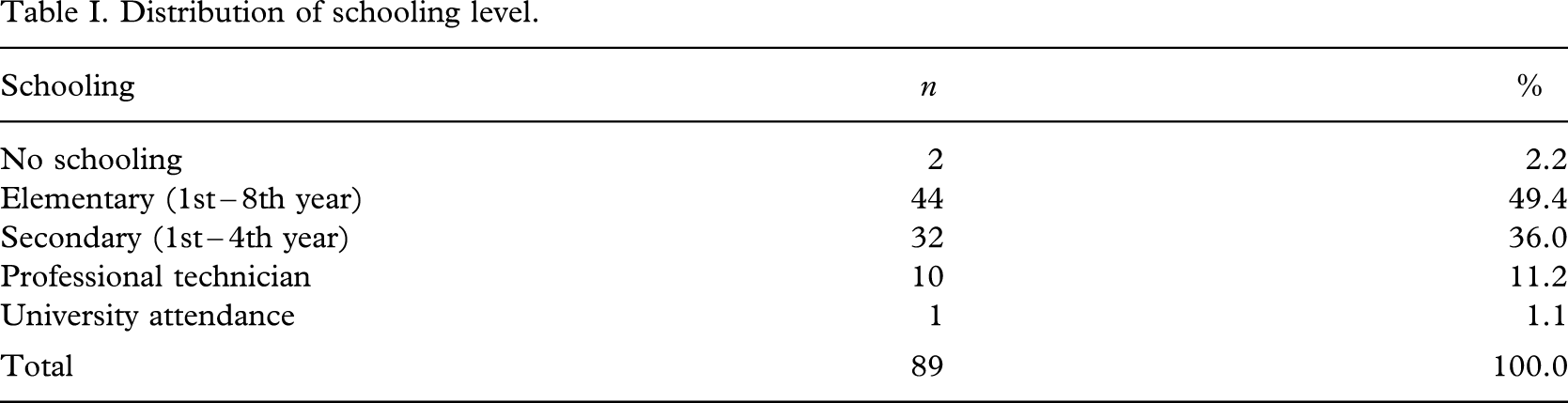
Schooling was stated in 89 cases and is shown in Table I, the cases being allocated according to the last year of school attendance and the educational level attained.
Distribution of schooling level.
As for the kind of work carried out by these patients, 98% were blue collar workers, 1% was administrative technicians and 1% was professionals. Among the previous medical history there was a 4% prevalence of diabetes mellitus, the prevalence of high blood pressure was 3%, chronic obstructive arterial disease was 1% and chronic venous failure was 2%. There was no history of morbidity in 84.7% of the cases.
Trauma occurred at the workplace in 89% of the cases and in 11% it took place during the journey between home and work. Among the causes of trauma to the lower limb leading to amputation, crushing was observed in 50 cases (50%), car accident in 19 cases (19%), run over by car in 14 cases (14%), burns in six cases (6%) and other causes were seen in 11 cases (11%). Lower limb amputation levels were distributed as follows: Boyd's foot amputation in five cases (5%), Syme's amputation in six cases (6%), trans-tibial in 47 cases (47%), knee disarticulation in two cases (2%), and trans-femoral in 40 cases (40%). In 48% of the cases amputations affected the right limb, while the left side was affected in 52% of the cases.
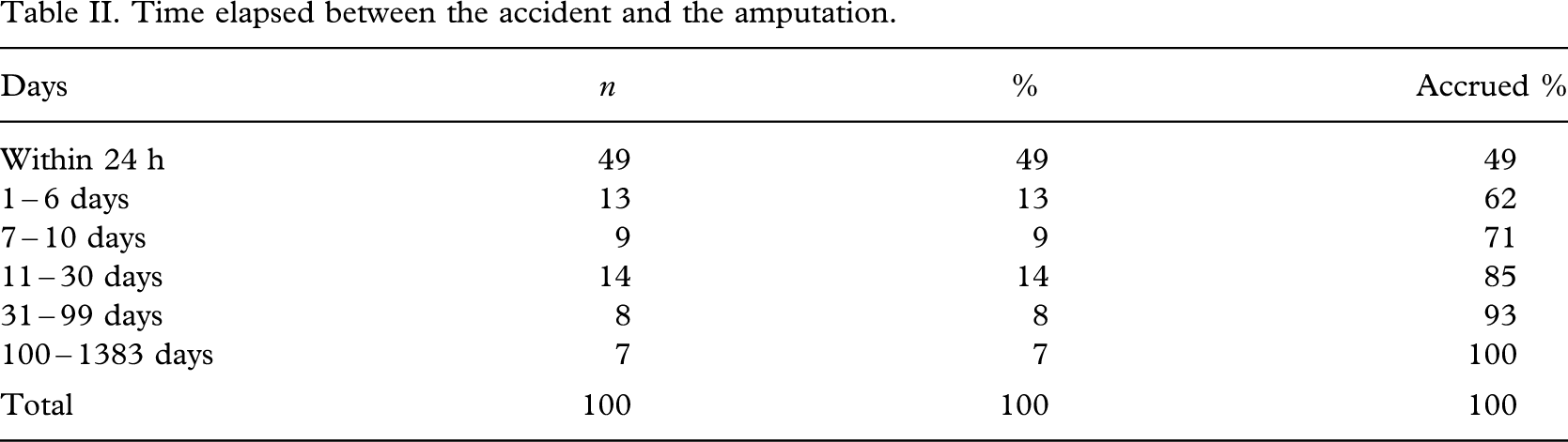
The time elapsed between the accident and the amputation is highly variable and Table II shows its distribution. Almost 50% of amputations occurred during the first 24 h, and 80% took place within a maximum period of 30 days (late secondary), with a mean period of 51 days.
Time elapsed between the accident and the amputation.
Initial hospitalization extended across several weeks in all cases, and reached more than eight weeks in almost 40% of the patients (Table III). The average hospitalization stay was 11 weeks for the 28 years covered by the study. Over the last 10 years, the average hospitalization stay has been 9.6 weeks and during the last five years it has reduce to 8.8 weeks. The minimum hospitalization stay in the study was two weeks.
Initial hospitalization stay.
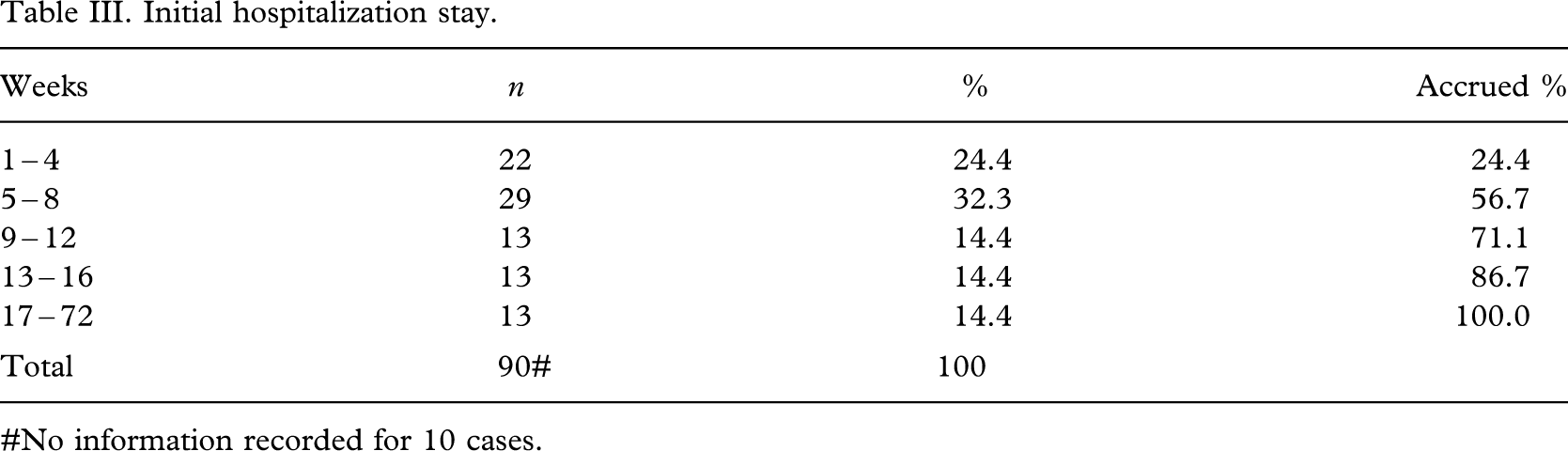
#No information recorded for 10 cases.
In 55.8% of the 96 record files which contained information about the presence of early complications post-amputation (during hospitalization) the most common recorded complications were dehiscence in nine cases (9.4%), superficial infection in 14 cases (14.6%), and deep infection in 25 cases (26%).
Data to establish the presence or absence of late complications (developed after discharge) were collected from 88 medical files. Late complications described were: Soft tissue injury in 30 cases (34.1%), exostosis in 12 (13.6%), painful neuroma in 11 (12.5%), soft tissue redundancy in 3 (3.4%), bone overgrowth requiring surgical therapy in 2 (2.3%) and other causes in 23 (23%).
Revision surgery of the stump was carried out in 18 cases (20.5%) none of which resulted in a reamputation of the stump. Phantom limb pain was reported in 11 cases (12.5%). There was no report of late complications in 27 of the 88 cases (30.7%).
All patients were fitted with a prosthesis and received gait training with good results. Only one medical file lacked both data regarding the fitting of a prosthesis and records of follow-up after discharge.
The time between the accident and discharge from outpatient rehabilitation service ranged between 3 and 46 months, with an average of 12.6 months. Sixty percent of patients were discharged within the first year.
There is a complete and reliable record of fitting of new prostheses, which range from 1 and 5, in 59 cases. The latter are generally the most recent patients with the more recent medical file records and shorter follow-up. Taking such facts into account, the resulting useful life of lower limb prosthesis lies within the large range of 6 – 111 months (9 years), with a mean value of 35.3 months and a median value of 30 months.
The total follow-up period for patients was also highly variable, ranging between a minimum of 6 months and a maximum of 28 years. The mean follow-up was 93 months (7.7 years) and the median was 79 months (6.6 years) (Table IV).
Total follow-up period.
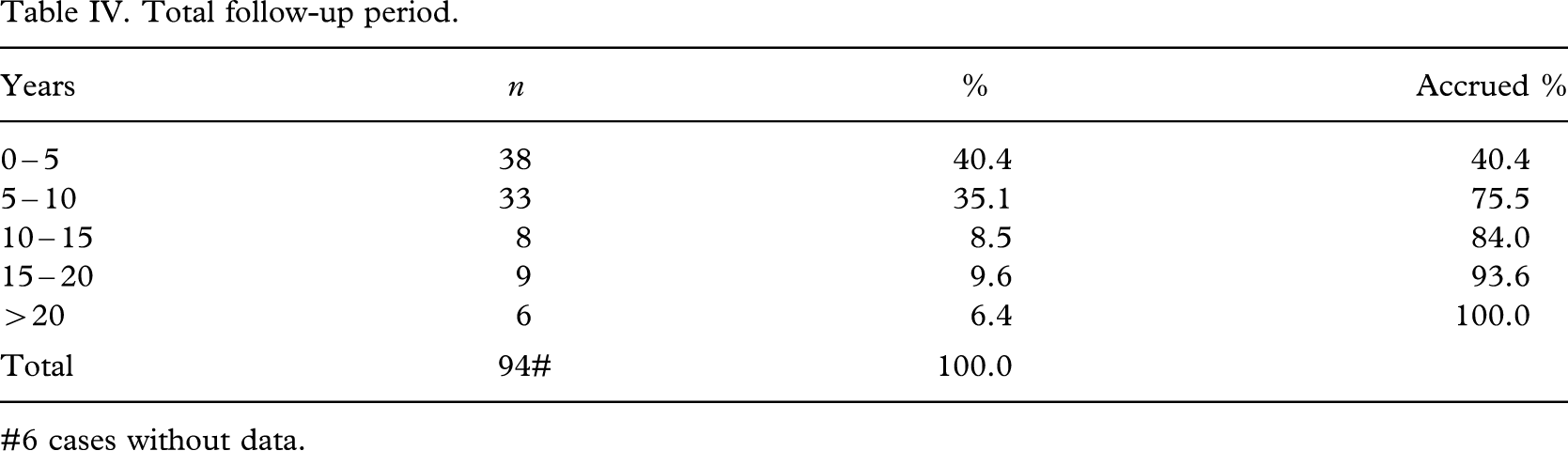
#6 cases without data.
Other sequelae were described in 22 patients: Musculoskeletal injuries in seven cases, nerve injury in four cases, a second amputation in four patients, chronic pain from other causes in four patients and various others in three cases.
Discussion
The data obtained were collected from patients followed-up during a period of 28 years at the same hospital, with an average follow-up of 7.7 years.
The lower limb traumatic amputees which were analysed in the present study are entitled to a non-state related work insurance. Trauma resulting in amputation occurred in relation with work, the vast majority taking place at the workplace while a lesser proportion occurred during the journey to or from work. In practically all the cases, work activity is unqualified (blue collar workers).
The study population is relatively young, with a mean age of 35.5 years. Other epidemiological studies regarding traumatic amputees in the general population reveal a greater mean age. In Denmark, Ebskov (1994) found a mean age of 49.4 (44.8 years among males, and 58.8 among females) for lower limb traumatic amputations. In the USA, Dillingham et al. (1998) found a mean age of 43.5 for major traumatic amputations, including upper limb amputations. Pezzin et al. (2000) reported a mean age, similar to the present study, of 32 years in the USA. On the other hand, amputations derived from medical conditions which occurred in patients aged on average 67 years (Pernot et al. 2000).
In the present study, amongst actively working patients, males account for more than 90% of lower limb amputees. The prevalence in the male gender is also higher in the general population in other studies: Pezzin et al (2000) reported 87% males, Ebskov (1994) reported a male:female ratio of 2:1and Dillingham et al. (1998) reported a ratio of 2.3:1.
When considering amputations of the lower limb only or when including all kind of traumatic limb amputations referred to the Hospital del Trabajador (Maturana & Carbonell 1999), demographic aspects including age, gender and occupation rates are the same.
As for the accident causes leading to amputation among this study's population, the most relevant two were limb-crushing injury at the workplace (50%) and traffic accidents (33%). Such data are similar to those of Dillingham et al. (1998) who reported the following rates among general population: Amputations due to traffic accidents accounted for 29%, falls accounted for 22.6%, equipment or motor-driven tools accounted for 29.1% and among the remaining percentage, a non-negligible proportion was due to firearms. Pezzin et al. (2000) reported a high rate of 77% for traffic accidents.
The length of hospitalization stay described by Ebskov (1994) was 49 days at the department of surgery; 56% of the cases were discharged home and the remaining was discharged to other hospital departments, foster homes or rehabilitation centers.
Dillingham et al. (1998) reported for trans-femoral amputations a maximum length of acute care hospital stay of 34 days which is shorter than that reported in this study over a period of 28 years, which were on average 11 weeks (77 days), with a decrease in the last few years to 63 days. The latter results partly from the complexity of injuries and the fact that amputation is not always considered as a first resort therapy, but as reconstruction surgery of the limb. The other cases with very long periods between the initial lesion and the amputation were due to failed treatment of osteomyelitis, late complications of surgically treated fractures or soft tissue lesions. However, it could also be explained by the fact that the early stages of rehabilitation of patients referred from different regions of the country are included in this period of hospitalization.
The distribution of rates for the different amputation levels of this study's group of patients showed a greater prevalence for trans-tibial (47%) and trans-femoral (40%) amputations. A similar situation was also described by Ebskov (1994) who reported almost 40% for both trans-tibial and trans-femoral amputations with no significant changes over a 12-year study.
Pezzin et al. (2000) reported a 38% prevalence for trans-tibial and with 22% for trans-femoral amputations and 15% for knee disarticulation, showing a rising tendency for knee disarticulation over 12 years.
The study carried out by Smith et al. (1995) described an average of 3.4 new prostheses delivered during the first three years after amputation and of 4.4 devices during the first five years resulting in an average of 10 and 13.6 months of use respectively. Within the authors' population the average life of prosthesis was almost 36 months.
The average resting period after the accident was approximately 12 months, during which all medical actions and complete rehabilitation therapies were completed, leaving the patient in good conditions to resume work. These findings are similar to Livingston et al. (1994) and Bruins et al. (2003) with an average period of 12 – 14 months between the accident and the effective restarting of labour, in those cases in which the patient resumes work. The results of Schoppen et al. (2001) show an average of 2.3 years before resuming work.
Besides amputation, approximately 22% of the cases had other considerable sequels resulting from the same accident.