
Abstract
Background: The International Classification of Functioning, Disability and Health (ICF) is comprehensive but difficult to use in clinical practice. ICF Core Sets are one method of increasing the use of the ICF in clinical practice. To develop a condition-specific core set requires identification of the concepts measured in current clinical practice.
Objective: To identify and quantify concepts contained in functional measurements used in published clinical studies utilising the ICF as a reference, for individuals with an amputation of the lower limb.
Study Design: Systematic literature review.
Methods: The concepts of published clinical and outcome measures used in individuals with a lower limb amputation were extracted and linked to the categories of ICF.
Results: The 113 outcome measures identified in the literature search contained 2210 functional concepts. Of the identified concepts, nearly 90% could be linked to ICF categories. The identified concepts linked to 44 categories in the domain of body functions and structures, 56 categories in the domain of activities and participation and 30 categories in the domain of environment.
Conclusions: Using the ICF as a reference, we could identify and quantify the majority of concepts in the outcome measures used in published clinical studies. The ICF categories identified will assist in the development of ICF Core Sets for persons with an amputation.
The ICF is available in over 25 languages. Improving the usefulness of the classification for clinicians will assist in standardising clinical practice and in comparison of outcomes nationally and internationally. ICF Core Sets are designed to use a manageable number of categories from the ICF to allow application in day-to-day clinical practice.
Keywords
Introduction
Lower limb amputation is a common chronic health condition and a cause of long-term disability. Lower limb amputation has a major impact on almost every aspect of a person's life. The numerous clinical studies and research reports on function and health-related quality of life following amputation describe a wide range of outcomes. There are multiple interactive variables that contribute significantly to the functional outcome, including medical co-morbidities, the surgical level of amputation, cognition, age, pre-morbid level of function, personal coping style, level of social support, environmental factors and financial resources available. 1 – 9 The current functional classification systems and outcome measures for persons with amputation are often tailored to local needs, and there is a lack of consensus regarding uniform or the most appropriate outcome measures. 10 – 12 For example, the K classification system mandated in the USA and in some Australian states, classifies only the functional mobility with the use of a prosthesis for a person with an amputation. Although the K classification is a relatively simple functional scale, there are no clear guidelines for the exact process of how to categorise an individual into the five levels of function in the classification. 13
Outcomes in prosthetic rehabilitation are influenced by various factors including psychological and cognitive aspects, medical co-morbidities, pre-morbid level of function and compliance. Therefore research on outcomes is difficult and at times conclusions from studies are conflicting and confusing. 10 – 12
One of the methodological issues is the lack of consensus on what standardised outcome measures should be used or what concepts should be measured.11,12
There is no globally agreed clinical classification. Very few outcome measures can be applied across cultures to enable healthcare professionals to share and compare the functional outcomes of persons with an amputation. Research data are often collected and stored in information ‘silos’ and cannot readily be compared with other interventions. 14
This situation supports the need for an internationally accepted classification of function, including health-related quality of life for individuals with an amputation.
Since the endorsement of the International Classification of Functioning, Disability and Health (ICF) by the World Health Assembly in May 2001, 15 a comprehensive and universally accepted framework to describe and classify functioning, disability and health in individuals with amputation has been available. The ICF is based on a model of functioning which is conceptualised as the dynamic interaction of the person, their function or functional limitations, their underlying health or physical condition and the environment in which they live. Personal factors may further modify these complex dynamic interactions.
The ICF classifies functioning into the components of body structures and functions, activities and participation, environment and personal factors. Personal factors are currently not categorised in the ICF. Each of the components is divided into a number of domains and within each domain there are numerous ICF categories which are the basic units of the classification, referred to as level two in the classification. Some categories are subdivided further, referred to as level three. For example the second level category d450 walking is further subdivided into d4500 walking short distances, d4501 walking long distances, d4502 walking on different surfaces and d4503 walking around obstacles.
As the ICF has 1454 categories, it is too unwieldy to use in the clinical setting in its entirety.16,17 In response to the challenge of implementing the ICF in clinical practice, a series of joint projects were initiated by the ICF Research Branch of the World Health Organization (WHO) Collaboration Centre at Ludwig-Maximilians University in Munich and the Classification, Assessment and Surveys team at WHO in 2001. The aim of these projects is to select those categories of the whole ICF classification that are essential for a specific health condition, a core set of descriptors. The collection of these categories should be comprehensive enough to include all the relevant aspects of a health condition and function but at the same time be practical and feasible.18,19 During the process of developing ICF Core Sets a broader perspective from consumer, researchers and healthcare professionals should be considered. This systematic review of published clinical studies of function in individuals with lower limb amputation is conducted to capture these diverse views from the perspective of the researcher. This review is one of the four preliminary studies for the development of an ICF Core Set for individuals with lower limb amputation.
Objective
The objective of this systematic review is to identify relevant published literature on functioning, disability and health of individuals with lower limb amputation and to identify and quantify the concepts contained in functional measurements used in these studies utilising the ICF as a reference document.
Methods
An electronic search of published studies between 1996 and May 2010 was performed in Medline, Embase, PsychINFO and CINAHL. The following search terms: leg amputation, knee amputation, below knee amputation, above knee amputation, traumatic amputation, amputation stump, limb prosthesis, leg prosthesis, rehabilitation, functional status, functional assessment, outcome assessment, treatment outcome, health status, well-being, health survey, outcome variable and quality of life were used. We included observational studies, randomised clinical trials and randomised controlled trials with target populations of age 18 years or over with lower limb amputation. We excluded studies on individuals aged less than 18 years, studies on animals, reviews, comments, correspondence and case series or reports.
All identified studies had a preliminary check of abstracts. Those studies relevant according to the search criteria outlined above were selected for full review and data extraction. In the data extraction phase, the researchers identified the outcome measures used in the studies and then extracted the underlying concepts of the parameters of the outcome measures. These identified concepts were then linked to the ICF categories using the standardised published linkage rules by two researchers independently.20,21 Concepts which were not able to be linked to ICF categories were assigned into several groups. If the concept is related to a health condition it is assigned ‘health condition’. If an identified concept is considered as a personal trait which is not coded in the ICF, it is assigned as ‘personal factor’. If a concept is too general or not specific enough to be linked to any ICF category then the concept is assigned as ‘not defined’. If a concept is not covered by the ICF such as suicide, it is assigned as ‘not covered’.
On completion of the individual linkage to the ICF, the list of ICF codes of the two researchers were compared. In cases of initial disagreement on linked concepts, a consensus linkage to the ICF was performed by the two researchers together, again according to the standardised linkage rule. Agreement was reached by consensus linkage in all cases.
Categorical frequency analysis was applied to the linked ICF categories. If an ICF category was repeatedly coded in any part of a defined outcome measure, it would only be coded once. To be consistent with previous similar studies, we only present ICF categories to second level even when they are linked more accurately at the third or fourth level of the classification. This can be justified as the lower levels of a category share the same attributes of the higher level categories.
Results
A total of 435 studies were identified as potentially suitable by the initial search. After the preliminary abstract check, there were 98 studies selected to proceed to the next stage. A full list of the studies is included as Appendix 1 (see supplementary material). The 98 studies utilised 113 different outcome measures to quantify functioning and health.
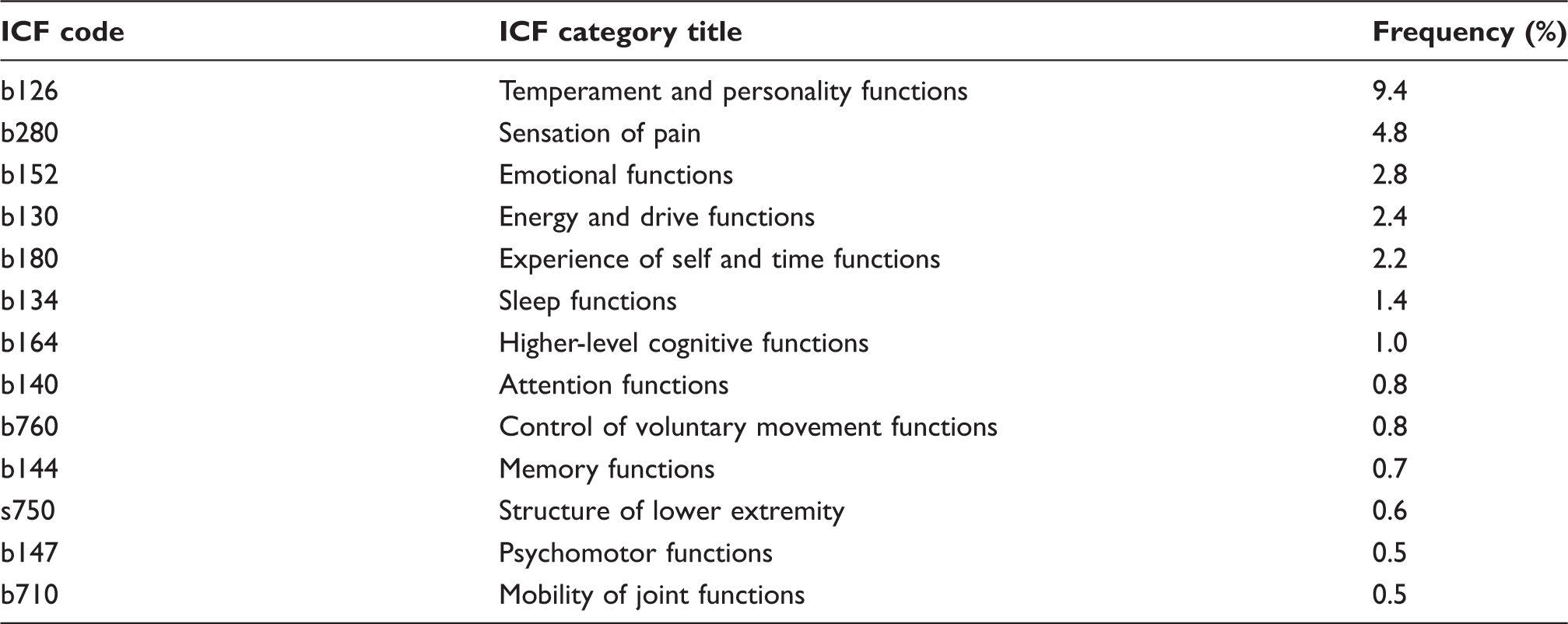
The relative frequency of linked International Classification of Functioning, Disability and Health (ICF) categories in the domains of body functions and structures.
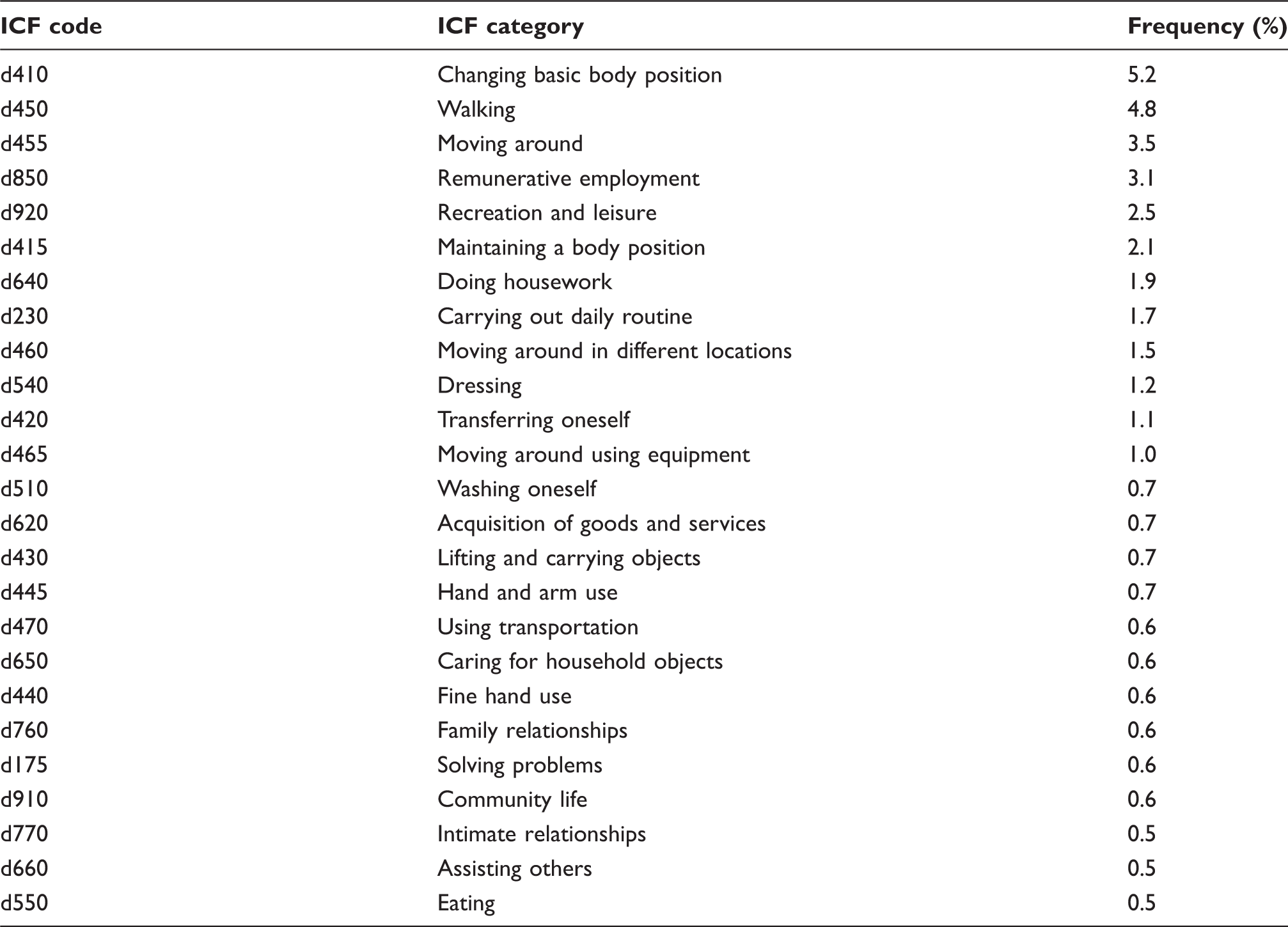
Relative frequency of International Classification of Functioning, Disability and Health (ICF) categories linked to activities and participation.
Relative frequency of ICF categories linked to environmental factors.
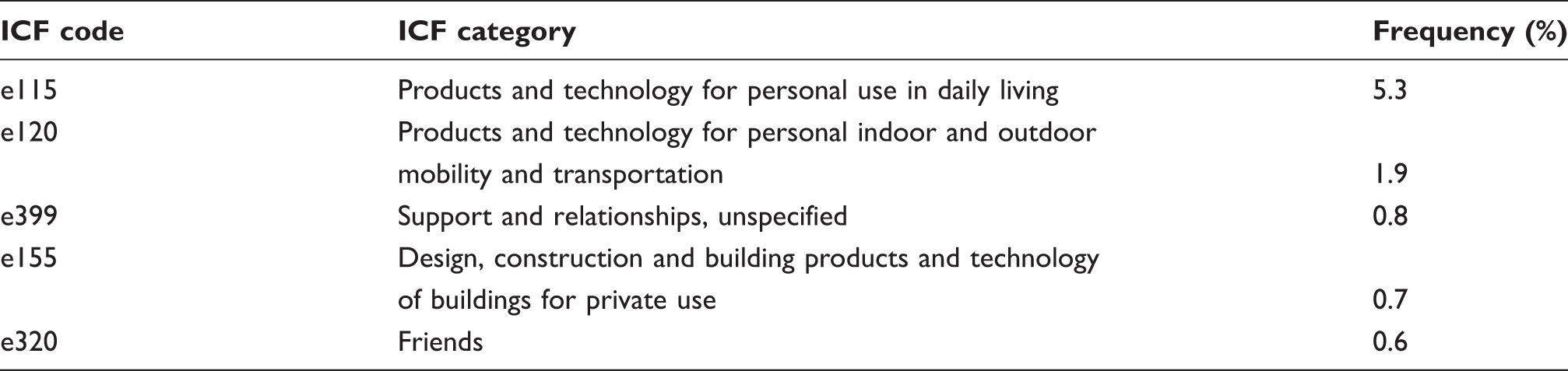
Of the 1973 linkable concepts, 709 (35.9%) were linked to 41 categories in the body functions, and 18 concepts were linked to three categories in the body structures in the domain of body functions and structures. A further 956 (48.4%) of concepts linked to 56 categories the domain of activities and participation. The remaining 290 (14.6%) of linkable concepts were linked to 30 categories in the domain of environment. More details including a list of those categories which were linked with a frequency of 10 or more are listed in Tables 1 to 3, grouped by the domain of the ICF.
Discussion
Clinically meaningful classifications and outcome measures are essential in the health system today. There are significant pressures from funding bodies, healthcare policy makers and frontline healthcare professionals for the development of comprehensive and practical user-friendly measurement tools. The search for an ideal, gold standard, outcome measure for individuals with a lower limb amputation that is meaningful to clinicians, patients and other interested parties is ongoing. The systematic literature reviews on individuals following lower limb amputation published in the last decade highlight the lack of consensus as to what to measure. 10 – 12 The reviews identify a large number of outcome measures being used for individuals with a lower limb amputation, but only a very small proportion of the outcome measures appear to be used regularly. While some of the studies have correlated the outcome measures to the ICF,12,22 our study is unique in correlating the concepts contained in the outcomes measures with ICF categories.
The majority of the outcome measures we identified are generic measures with only 14% being condition specific for lower limb amputation. 11 As generic instruments are more general in application, they would be expected to include a broader range of concepts than condition-specific measures. This is evident in our review, as over half of the concepts identified were only used infrequently. We identified 44 concepts which appeared at least 10 times, and these concepts were predominantly in the domain of activities and participation, with body functions also well represented. Environmental factors were measured less frequently. This can possibly be explained by several factors including the difficulty of meaningfully measuring environmental factors, clinicians concentrating more on clinical factors, and perhaps adaptation of the individual rather than the environment being a more common strategy in rehabilitation, with environmental manipulation being a more recent strategy and, perhaps to some extent, restricted to industrialised countries.
As nearly 90% of all concepts identified from the literature can be coded by the ICF, this is a strong indication that the ICF has considerable potential for increased utilization in the description, treatment planning, classification and measurement of outcomes of individuals following an amputation. Some of the concepts coded as ‘not covered’ were so broad that they could only have been included at the domain or chapter level of the ICF classification and therefore would add little to the description of the individual's limitations.
Another concept which was not covered was satisfaction with the service or prosthetic components. While the ICF covers health services being facilitators or barriers, it does not cover the individual's satisfaction with the services or prosthetic components. Further and more detailed analysis of the 192 concepts which were not covered by the ICF would be valuable, and possibly assist in a future refinement of the ICF classification itself.
As previously published, 12 the predominant concepts contained in outcome measures for persons with an amputation are in the domain of activities of the ICF. Almost half of the concepts that could be linked to the ICF were linked to the domain of Activities and Participation. Representation within this domain is widespread, with a total of 55 level two categories including categories from each of the nine chapters including learning and managing general tasks, communication, mobility, self-care, household tasks, relationship, employment, community and social life. Not surprisingly, the most frequently represented concept is related to various categories of mobility (d410–d499) accounting for a total 491 (22%) of the total identified concepts. This is in line with expectations as the target population of persons with lower limb amputation will almost universally have some mobility limitations. Work, social and community life (d710–d999) are also concepts which are represented frequently accounting for 207 (9%) of all concepts. This most likely reflects the increasing awareness of the importance and relevance of these outcomes by clients and clinicians.
Body functions have the second highest number of ICF categories contributing to 34.5% of the total categories. There is a widespread distribution of these categories with clusters focusing on mental function, pain and musculoskeletal functions. Somewhat surprising was the finding that the linked categories in body functions are predominantly (488 categories) related to mental function (b110–b199). This could reflect the relationship between cerebrovascular and peripheral vascular disease which might have predisposed to the amputation, as well as a recognition that there might be changes in mood as a consequence of an amputation and the related treatment processes. Alternatively, it may imply that functional loss from amputation may be compensated with a prosthesis or mobility aids including a wheelchair, but the functional outcome is influenced by the intrinsic personal traits, cognition, problem solving skills and value systems. We are mindful of the fact that ICF does not categorise personal factors, so some of the concepts (207 or 9%) were linked to categories in the sub-domain of temperament and personality functions. This finding indicates that in rehabilitation of the individual with an amputation, the focus is the whole person outcome and most of the outcome measures related to quality of life have a significant element of measurement of a person's subjective feelings and wellbeing.
Pain is the second most common category in the domain of body function. This is consistent with the high prevalence of phantom pain, pain related to the underlying disease or post-surgical pain in persons with lower limb amputation and the need for ongoing pain management as well as the interaction between pain and prosthetic use.
As outlined by Deathe, it would be useful to include the context in which the functional concept operates. 12 In the ICF, the domain “environmental factors” was developed to enable the integration of contextual factors into the biopsychosocial model of function and disability. Environmental factors contribute 14.6% of total linkable concepts. The concepts of environmental factors include effects at the individual and societal level. The concepts are most frequently related to equipment assisting in activities of daily living and mobility, such as the provision of prostheses and walking aids, environmental manipulation, such as installation of ramps, and the social support network.
Utilisation of the ICF qualifiers facilitates the description of the dynamic interaction between an individual with a lower limb amputation and their environment either at individual or societal level, which is either a facilitator or a barrier.
In other studies for the development of ICF Core Sets, researchers have reported linked ICF categories occurring with more than 10% frequency. 23 – 25 We report in detail on those concepts which were included in measurements 10 or more times. This provides a manageable number of items as well as including common concepts contained in a number of outcome measures used for individuals with a lower limb amputation. A comprehensive list including all details of the categories matched to the concepts we found in the literature is available in Appendix 2 (see supplementary material). The decision as to which categories will be included in the ICF Core Set for persons with lower limb amputation will ultimately be determined at a consensus conference. Details of the process of developing the core set for individuals following lower limb amputation has been published. 14
One limitation of this study is that it only includes studies and outcome measurements available in the English language. We acknowledge that there are other relevant measures in other languages, but in view of the language skills of the researchers, we had to restrict the sample to studies in English. Consultation with colleagues representing some of the Asian and other European languages suggests that the list of concepts is extensive. We accept, however, that there might be some concepts particularly relevant to individuals living in non-industrialised countries that are not captured in this study.
A further limitation might be that the literature search was restricted to the last 15 years. We considered, however, that this timeframe would cover concepts currently thought to be important, but we acknowledge that there might be some concepts in the earlier literature that we did not capture.
As previously described, multiple systematic reviews of the psychometric properties of the outcome measures identified in this review exist, and we did not intend to repeat this form of quality analysis on the outcome measures in the selected studies. 10 –13,22 Our purpose was to describe and quantify the concepts which were used in outcome measures in the published literature and we have restricted our study to this.
Conclusion
Having identified 2210 concepts contained in over 113 outcome measures used in published studies on the management of individuals with lower limb amputation, we were able to successfully crosslink the majority (89.3%) of the concepts to a total of 130 ICF categories in the domains of Body Function and Structure, Activities and Participation and Environmental factors. Based on this, we conclude that the ICF could be used to classify major outcome variables for individuals with an amputation. The ICF categories which we have described will assist in the development of a clinically meaningful and practical ICF Core Set for persons with an amputation.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.