
Abstract
Background:
Within the prosthetics profession, there is a lack of evidence to support many clinical practices. It is therefore important that clinicians systematically document and evaluate their daily practices.
Objectives:
To record preoperative characteristics and functional outcomes for patients with a lower limb amputation and to investigate variations between prosthetic users and non-prosthetic users.
Study Design:
Prospective cohort study.
Methods:
A total of 23 patients (mean age = 80 years, standard deviation = 7.3) who underwent a major lower limb amputation were assessed within 2 weeks of admission and 6 months post-operatively. Locomotor Capabilities Index-5, the Timed-Up-and-Go Test and prosthetic use were used to evaluate functional outcomes.
Results:
A total of 13 participants (57%) received a prosthesis within 6 months of amputation. Mean time to prosthetic fitting was 48 days (range = 28–97). No statistically significant difference was found between prosthetic users and non-prosthetic users regarding age, time to rehabilitation and Locomotor Capabilities Index-5 (p > 0.05). Locomotor Capabilities Index-5 basic was significantly lower at 6 months than prior to amputation (p = 0.039).
Conclusion:
The functional outcome at 6 months indicates a sizable restriction in mobility among lower limb amputees. No variation in preoperative characteristics between prosthetic users and non-prosthetic users could be confirmed in this study.
Clinical relevance
This study highlights the need for prosthetists to better incorporate research findings into their daily practice and presents an example of how to implement a procedure for assessment and documentation of patients’ functional outcomes in a clinical setting. Results confirm difficulties in identifying amputees who will become prosthetic users based on preoperative characteristics.
Background
Many of the daily treatment choices facing prosthetists relate to maximizing functional outcomes of patients with their prosthesis. In order to evaluate success or failure of treatment alternatives and clinical routines, and to predict potential outcomes for groups of patients, it is necessary to first understand baseline characteristics of the patient population. This requires documentation of amputee characteristics, rehabilitation processes, prosthetic fitting and functional outcomes. The use of a standardized clinical assessment and documentation procedure, where the main factors affecting prosthetic treatment and functional outcome for the amputee are collected and consequently evaluated, is a necessary step to take for prosthetic and rehabilitation departments. To contribute to the body of evidence within prosthetics and orthotics and facilitate high-level reviews and meta-analyses, it is also important that these data are shared and made public in peer-reviewed publications. Ramstrand and Brodtkorb 1 stress that prosthetists/orthotists need to become more active in generating research rather than relying on other professional groups to contribute to their professional body of knowledge.
Fortington et al. 2 report that there is a need for standardization in reporting of amputee outcome measures and population characteristics to improve the overall methodological quality of future studies. Today, there is heterogeneity of methods and outcome measures used in studies within the prosthetic field, which makes comparison difficult and, in part, explains conflicting conclusions. 3 Outcome measurements that have been validated and tested for reliability in an amputee population are becoming more readily available. These not only include general measures, such as the Timed-Up-and-Go Test (TUG)4,5 and Locomotor Capabilities Index (LCI),6,7 but also specific outcome measurements, which have been developed specifically for the amputee population, including The Prosthetic Profile of the Amputee questionnaire (PPA), 8 Prosthetic Evaluation Questionnaire (PEQ) 9 and Questionnaire for Persons with Transfemoral Amputation (Q-TFA). 10 Some of these specific outcome measurements are very comprehensive and quite time-consuming to apply. This can make them less suitable to use on a daily basis. We suggest that outcome measurements forming a standardized part of treatment protocols within prosthetic or rehabilitation departments need to be easy to apply and to use in daily clinical settings.
Many different characteristics (e.g. age, cause of amputation) and rehabilitation-related factors (e.g. time to rehabilitation and prosthetic fitting) have been shown to affect the outcome of rehabilitation.2,11–15 To date, there is no consensus in the literature regarding which factors should be included in a standardized treatment protocol. Fortington et al. 2 recommends that characteristics, such as age, sex, cause of amputation, level of amputation and whether the study subjects are unilaterally or bilaterally amputated should be noted in all protocols. In support of this, studies investigating walking ability after lower limb amputation show that age,11,13,14,16–18 cause of amputation11,19 and level of amputation11,12,14,15,20,21 have a significant effect on functional outcomes. Extended time between amputation and prosthetic fitting has been shown to have a negative impact on walking ability 3 and prosthetic use,14,18 making these variables of particular interest. Time to rehabilitation has also been shown to have a substantial influence on functional outcomes after lower limb amputation.14,22
The purpose of this research was to record preoperative characteristics, which may predict functional outcomes and success of prosthetic fitting in patients who have undergone a major lower limb amputation at Southern Älvsborg Hospital, Sweden. An additional aim was to assess functional outcomes for these patients 6 months after amputation, and to investigate variations in preoperative characteristics for those amputees who received prostheses and those who did not receive prostheses within 6 months of amputation.
Methods
Participants and data collection
Between October 2009 and March 2010, a total of 45 persons were amputated at Southern Älvsborg Hospital, 20 of whom were considered to be in poor mental and/or physical condition and were subsequently considered by the rehabilitation doctor in charge as unable to manage with a prosthesis. The remaining 25 consecutive patients at Southern Älvsborg Hospital were invited to participate in this prospective cohort study. Patients were invited to participate on the basis that they had undergone a transtibial (TT), knee disarticulation (KD) or transfemoral (TF) amputation, were identified as potential prosthetic users by the rehabilitation doctor in charge or expressed a desire to try a prosthesis. A potential prosthetic candidate was defined a person who, in the specialist’s opinion, may eventually be able to use a prosthesis for walking, transfers, standing or training.
The regional ethics committee in Gothenburg, Sweden approved methods for the study, and informed consent was obtained from all patients who participated.
Patients who were considered to be potential prosthetic candidates were divided into two groups. Those who received a prosthesis within 6 months (prosthetic users) and those who did not receive a prosthesis within 6 months (non-prosthetic users). All patients were assessed within 2 weeks of admission at the rehabilitation clinic. On this occasion, a researcher (certified prosthetist/orthotist) documented baseline characteristics considered as potentially influencing future prosthetic function and administered a functional capabilities test to evaluate the patients’ perception of their function 3 months prior to their amputation, LCI-5. The prosthetic user group was further assessed on a second occasion (6-month follow-up). On this occasion, the researchers administered two functional tests, LCI-5 and the TUG, and documented the patients’ prosthetic use.
Baseline factors, functional outcome and prosthetic use
The baseline factors analysed as potential predictors of function with a prosthesis were age, sex, level of amputation, cause of amputation and residential situation. Time to rehabilitation, that is, time from amputation until the first day of exercise after admission at rehabilitation unit, and time to prosthetic fitting were also observed as potential predictors for functional outcome 6 months after amputation.
TUG was performed according to procedures outlined by Schoppen et al. 16 Subjects initially sat in a standard armchair with their back against the chair, arms resting on the arms of the chair, and their walking aid at hand. The instructor then counted to three and on ‘three’ the subject got up, walked to a line on the floor 3 m away, turned, walked back to the chair and sat down again. Subjects chose their own comfortable and safe walking speed. 16 A TUG test of 19 s or more increases the risk of having multiple falls in patients with unilateral lower limb amputation. 23 The TUG test is a reliable and valid test for quantifying functional mobility in lower limb amputees.4,5 When using the LCI-5, the patient was required to estimate their capability in performing a variety of different activities with their prosthesis, for example, rising from a chair or walking up and down a staircase. The measuring tool consists of 14 questions and is divided into two parts, basic activities and advanced activities. LCI-5 is a further development of LCI and has been complimented with a fifth alternative to distinguish if the patient performs the activity with or without aids. 6 LCI and LCI-5 have been tested and established for validity and reliability in an amputee population.6,7
Prosthetic use was defined as hours of prosthetic use per day and was divided into intervals (0–3 h, 4–6 h, 7–9 h, 10–12 h and >12 h) and days per week (1–7 days). The same intervals for time per day are used in the Swedish quality register for amputations and prostheses and in earlier studies.10,24
Statistical analysis
Given that this was a small and non-homogenous group, data are presented in a descriptive form and non-parametric statistics are used for group comparisons. Data are presented as means and standard deviations (SDs) or medians and range, as appropriate. A Mann–Whitney U test was performed to see whether there was a difference in the mean age between men and women, and was also used to compare the median LCI-5 scores before amputation, mean time to rehabilitation and mean age between prosthetic users and non-prosthetic users. For prosthetic users, a related samples Sign test was used to compare LCI-5 scores before amputation and at 6-month follow-up. All data were analysed using SPSS 19 (SPSS Inc., 2010, Chicago).
Results
Figure 1 depicts the recruitment of patients for this study. Of 25 persons who underwent a TF, TT or KD, amputation between October 2009 and March 2010, and were identified as potential prosthetic users, 23 agreed to participate in the study (see Figure 1). A total of 13 of these patients received a prosthesis within 6 months. The results of baseline characteristics for patients who participated in the study are presented in Table 1. The mean age for all participants was 80 years (SD = 7.3 years). The mean age for women (10) was 84 years (SD = 3.5 years) and for men (13) was 78 years (SD = 8.4 years), the disparity was statistically significant (p < 0.05). According to the definition of level of amputation provided in ISO standard 8545-2, 15 patients were classified as TT amputees, 4 were KD amputees and 4 were TF amputees. Five of the participants had previously undergone a TT amputation and had been admitted to the rehabilitation unit after an amputation of their contralateral leg (bilateral amputees). Bilateral amputees are shown in a separate row in Table 1.
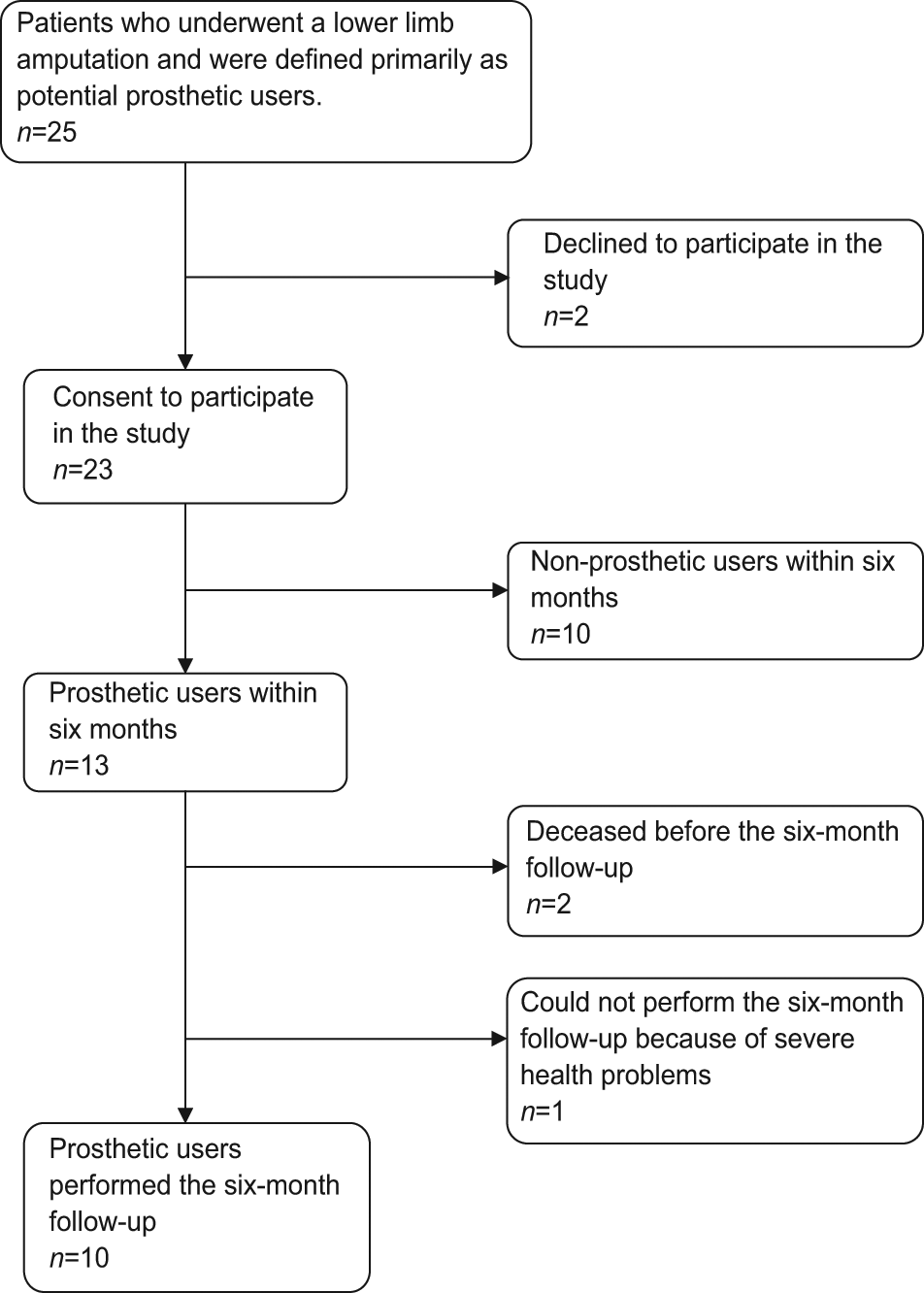
Flow diagram showing participants in the study.
Characteristics, predictors for functional outcome and prosthetic use.
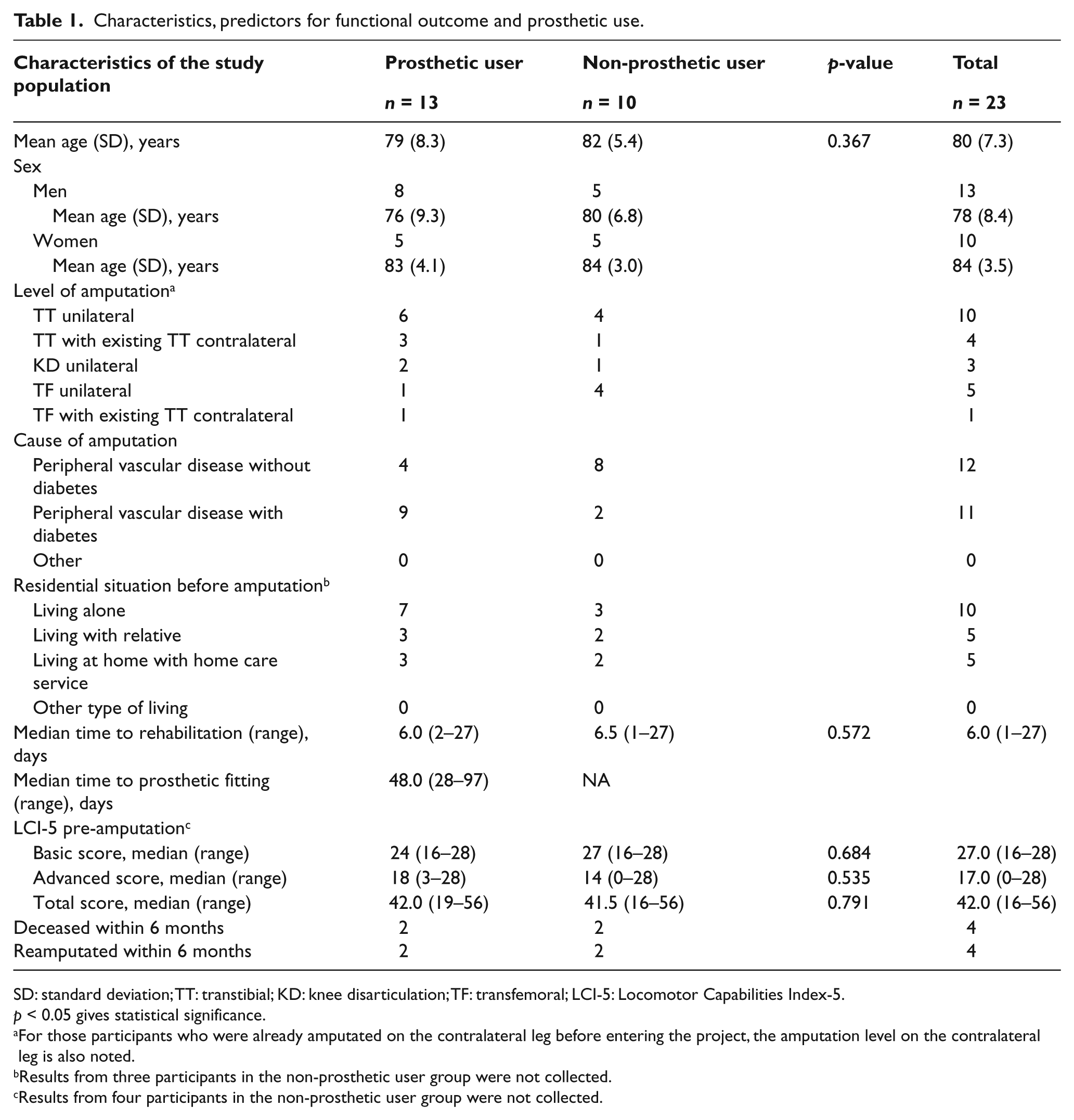
SD: standard deviation; TT: transtibial; KD: knee disarticulation; TF: transfemoral; LCI-5: Locomotor Capabilities Index-5.
p < 0.05 gives statistical significance.
For those participants who were already amputated on the contralateral leg before entering the project, the amputation level on the contralateral leg is also noted.
Results from three participants in the non-prosthetic user group were not collected.
Results from four participants in the non-prosthetic user group were not collected.
The cause of amputation was peripheral vascular disease with or without diabetes for all participants (23), and 11 of them had diabetes. All participants lived in their own home prior to amputation and 25% (5) of the study group had received home care services prior to their current amputation; two of them were previously amputated on the contralateral leg. The median time from amputation to admission at the rehabilitation clinic was 6 days (range = 1–27). The median of total LCI-5 scores for all participants before amputation was 42 (range = 16–56). The median of LCI-5 basic score was 27 (range = 16–28), and the median of LCI-5 advanced score was 17 (range = 0–28).
Three patients underwent reamputation surgery on the ipsilateral side within 6 months of the initial amputation, and one patient, previously amputated at a TT level, had approximately 3 cm of tibia removed but remained a TT amputee. Only two of those who underwent a reamputation or a revision became a prosthetic user within 6 months of the initial amputation. Four participants died within 6 months of amputation.
Prosthetic users versus non-prosthetic users
There was no statistically significant difference between prosthetic users and non-prosthetic users regarding mean age, time to rehabilitation and LCI-5 (p > 0.05), see Table 1.
Prosthetic users results at 6-month follow-up
Within 6 months of amputation, 13 participants were fitted with a prosthesis. The 6-month follow-up was performed on 10 of the prosthetic users. Two participants in the prosthetic user group passed away within 6 months, and one participant suffered from severe health problems (see Figure 1). The characteristics and time to prosthetic fitting for prosthetic users are presented in Table 1. The mean age of patients who were eventually fitted with a prosthesis was 79 years (SD = 8.3 years). Eight prosthetic users were men (mean age = 76 years, SD = 9.3 years), and five were women (mean age = 83 years, SD = 4.1 years). Nine of the prosthetic users were TT amputees, two were TF amputees and two were KD amputees. Four of the bilaterally amputated patients received a prosthesis within 6 months of amputation. In the prosthetic user group, nine participants had peripheral vascular disease with diabetes. The median time from amputation to admission at the rehabilitation clinic in this group was 6 days (range = 2–27).
The median time from amputation to prosthetic fitting was 60 days (range = 28–202). The median scores for LCI-5 (total, basic and advance scores) for prosthetic users are presented in Table 2. The difference between LCI basic scores before amputation compared to the 6-month follow-up was statistically significant (p < 0.05), but the difference was not statistically significant for LCI-5 total and advanced scores. One patient scored the maximum 56 points before and 6 months after amputation. Two of the participants received a better score at the 6-month follow-up than they recorded before amputation.
Functional outcome and prosthetic use at 6-month follow-up.
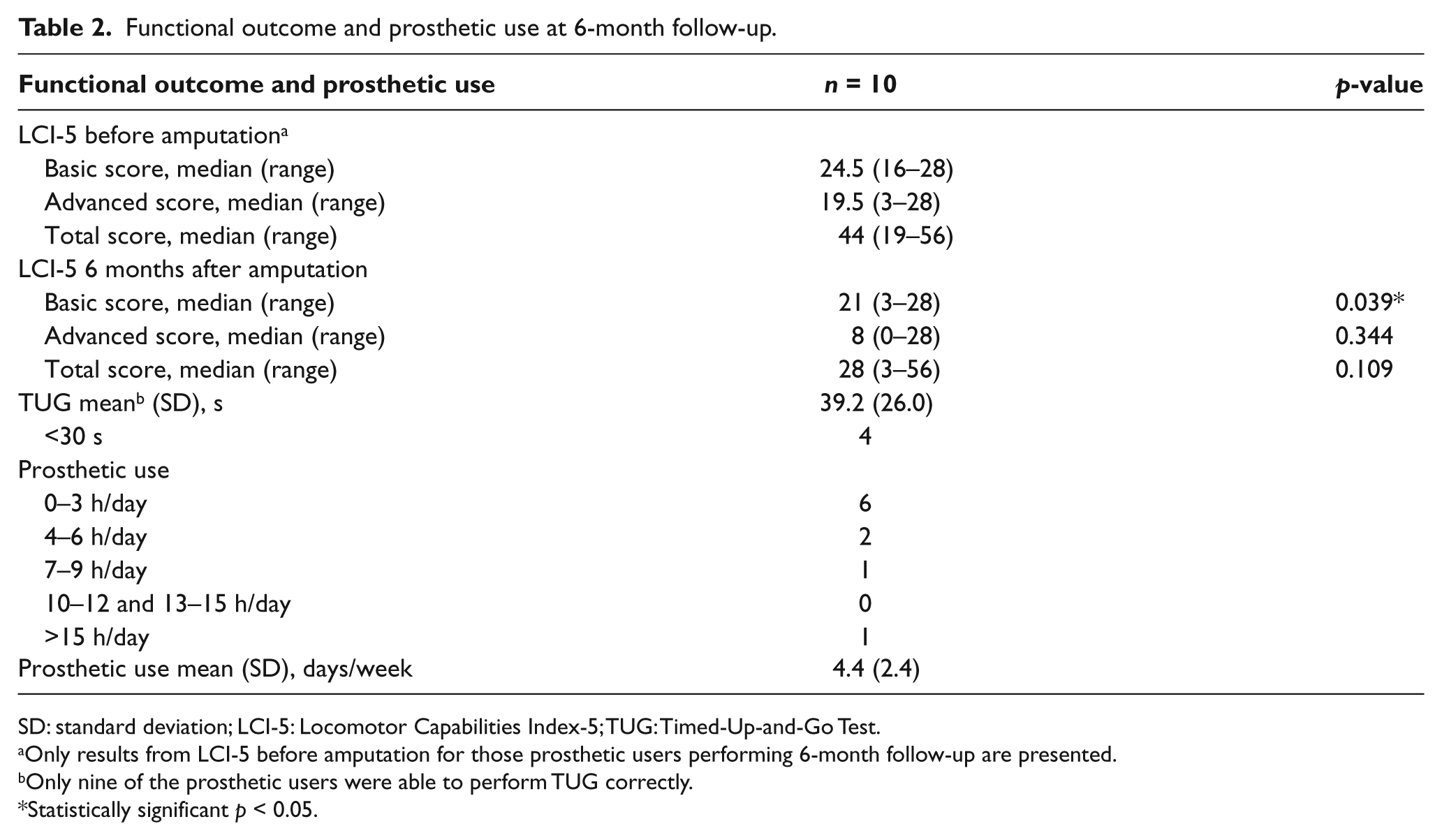
SD: standard deviation; LCI-5: Locomotor Capabilities Index-5; TUG: Timed-Up-and-Go Test.
Only results from LCI-5 before amputation for those prosthetic users performing 6-month follow-up are presented.
Only nine of the prosthetic users were able to perform TUG correctly.
Statistically significant p < 0.05.
Nine of the participants managed to perform TUG in an appropriate way; one bilateral amputee could only walk in the parallel bars. The mean of TUG was 39.2 s (SD = 2.4 years). Two of the participants used their prosthesis more than 7 h per day, all week long. Six of the participants used their prosthesis less than 3 h per day, and five of those used their prosthesis 2–3 days a week. On average, participants used their prosthesis 4.4 days per week. Four of the participants used their prosthesis every day. None of the participants had problems in donning or doffing their prosthesis independently.
Discussion
This study has demonstrated that it is possible to create and apply a systematic procedure in a clinical setting, where the main factors affecting prosthetic treatment and functional outcome for the amputee are collected and consequently evaluated. Data collected in this study, and that which continues to be collected, are important to establish a baseline by which future treatments can be compared and by which other facilities can potentially compare their own clinical outcomes.
The mean age of this study population was high, 80 years. Other published articles from Scandinavia have reported a mean age of 75–79 years for a group with similar patient characteristics.25–27 Mean age for participants who received a prosthesis within 6 months was also high compared to previous Swedish studies.25,28 In contrast to this study, however, these included only unilateral amputees with peripheral vascular disease. Women in this study were significantly older than men. Results are consistent with other studies,26,29,30 and this is likely to reflect the fact that life expectancy for women in the Swedish population is more than 4 years higher than men. 31 No difference was found when comparing the proportion of men and women who received a prosthesis. While these results are consistent with those report by Johannesson et al., 28 two other Scandinavian studies have reported that men are significantly more likely to receive a prosthesis after a lower limb amputation than women.25,32 This may reflect different treatment methods in use or variations in the patient populations under investigation.
All participants in this study were amputated because of vascular disease and approximately half of them had diabetes. The proportion of amputees with diabetes who received prostheses was greater than without diabetes. A possible reason for this is that people with diabetes often are younger at the time of their first amputation than those who are amputated because of other peripheral vascular diseases. 30
Mean time to prosthetic fitting in this study was 48 days, with a range of 28–97 days. A Finnish study reported an average time from amputation to prosthetic fitting of 117 days, the study population included TT and TF amputations and all types of amputation causes. 33 British data report that the mean time to delivery of prostheses was 182 days for a similar study population as the Finnish study. 34 Johannesson et al. 28 evaluated outcomes of a standardized surgical and treatment programme after TT amputation in patients with peripheral vascular disease. Time to prosthetic fitting in their study was 41 days, with a range of 12–147 days. 28 The large variation in mean time from amputation to prosthetic fitting can be influenced by variations in population characteristics and differences in surgical and manufacturing procedures. The need for a well-functioning rehabilitation team and clear guidelines for rehabilitation of amputees is highlighted in these results.
In this study, no variations in preoperative characteristics between prosthetic user and non-prosthetic users were confirmed regarding age, time to rehabilitation and LCI-5 prior to amputation. This is in contrast to some other studies that have found that age is a predictor for receiving a prosthesis.16,25 Time to rehabilitation and LCI-5 have not previously been evaluated as predictors of prosthetic use; however, time to rehabilitation has been reported as a predictor of walking potential. 18 A variation in attitude within different rehabilitation departments regarding which amputees should be given the opportunity to receive prosthesis could be one explanation why the results in this study do not coincide with other studies. All mean scores of LCI-5 (total, basic and advanced) were lower at the 6-month follow-up post amputation when compared to patient perceptions of their mobility prior to the amputation. Given that the average time to prosthetic fitting was 48 days, one can expect further improvement in patient mobility in the future. Frlan-Vrgoc et al. 12 note that time to the first prosthetic fitting positively affects functional outcomes.
A mean of TUG of 39.2 s (SD = 26.0 years) indicates that the participants in this study have a high risk of falling. Dite et al. 23 showed that a TUG test of 19 s or more increases the risk of having multiple falls. A Dutch study noticed a mean TUG time of 23.9 s (SD = 13.2 years) for amputees with a mean age of 73.9, 1 year after amputation. 16
One limitation of this study is the low number of participants. This reduces statistical power and the conclusions that can be drawn from the study. With the exception of two patients who did not wish to participate, this study did include all patients who became amputees over a 6-month period at Southern Älvsborg Hospital. The study reports follow-up with patients at 6 months from their amputation, and it would be beneficial to observe patients over a longer period. The participants in this study were of high mean age, many of them had concomitant health conditions, and their general physical status was rather poor. We consider 6 months to be a relatively short time for recovering after a major lower limb amputation. Data collection is continuing as part of a larger longitudinal study.
Conclusion
Quality care of amputees requires that prosthetic facilities continually evaluate their own practices and how they affect patient outcomes. This requires a systematic approach to patient management, which includes documentation of patient progress over time. This study presents an example of how this can be done in a clinical setting. Results have demonstrated that new amputees treated at Southern Älvsborg Hospital, Sweden, have a relatively high age. The initial prosthetic fitting is typically done within 48 days of amputation, and there are, on average, considerable restrictions in mobility at 6 months post amputation. No difference in preoperative characteristics between prosthetic users and non-prosthetic users could be confirmed.
Footnotes
Acknowledgements
The authors would like to thank Kjell-Åke Nilsson, Ulf Henriksson and Jakob Vikström for their assistance in this study.
Conflict of interest
The authors report no conflict of interest.
Funding
This project was funded in part by FoU Sjuhärad välfärd, Sweden, a centre for research and development in the field of welfare, and Department of Research and Development at Southern Älvsborg Hospital, Sweden.