
Abstract
Background:
Technological advances in prosthetic design include the use of microprocessors that adapt device performance based on user motion. The Proprio ankle unit prepositions the foot to adjust for walking on slopes and increases foot clearance during swing to minimize gait deviations.
Study design:
Comparative analysis.
Objectives:
To investigate the effect of a prosthesis with adaptive ankle motion on physiological gait performance during slope walking.
Methods:
Six persons with a unilateral transtibial amputation completed treadmill walking tests at three slopes (−5°, 0°, and 5°). The participants were tested wearing a customary device, active Proprio (Pon), and an identical inactivated Proprio (Poff).
Results:
Metabolic energy expenditure, energy cost for walking, and rating of walking difficulty were not statistically different between the Pon and Poff for all tested slopes. However, for slope descent, energy expenditure and energy cost for walking improved significantly by an average of 10%–14% for both the Pon and Poff compared to the customary limb. Rating of walking difficulty also showed an improvement with slope descent for both the Pon and Poff compared to the customary device. An improvement with slope ascent was found for Pon compared to the customary limb only.
Conclusions:
Adaptive ankle motion provided no meaningful physiological benefit during slope walking. The Proprio was, however, less demanding than the customary device for slope descent. Differences in the mechanical properties of the prosthetic feet likely contributed to the changes.
Clinical relevance
While the adaptive ankle motion did not affect metabolic energy expenditure or energy cost for walking, the results suggest close attention should be paid to the mechanical properties of the foot component. Assessment of gait on nonlevel surfaces is recommended to better understand the implications of different prosthetic design features.
Introduction
For individuals living in the community, the ability to safely and efficiently negotiate walking up and down sloped surfaces is functionally important. Accommodating nonlevel walking surfaces is easily accomplished in able-bodied individuals by adapting the motions of the lower extremities. 1 In persons with a lower extremity amputation, inherent limitations in the range of motion and power production of conventional prosthetic devices 2 increase the pressure on residual limb within the socket, 3 perception of walking difficulty, 4 oxygen consumption, 5 and risk for falling 6 while walking up and down graded surfaces.
Recent advances in prosthetic technology have produced devices aiming to address some of the design limitations. The Proprio (Ossur BV) was the first commercially available microprocessor-controlled prosthetic system for use by persons with transtibial amputation. The device uses accelerometer data to determine the orientation and motion of the leg and then adapt device performance with the end goal of improving stair and slope walking. Specifically, a motor is used to preposition the foot in either dorsiflexion or plantarflexion prior to loading during slope ascent or descent and to actively dorsiflex during swing to improve foot clearance. Fradet et al. 7 compared the commercially available Proprio and its adaptations in ankle motion with an identical device modified so that the ankle remained in neutral. The results demonstrated that during slope ascent increased stance phase ankle dorsiflexion facilitated more normalized knee kinetics and ultimately tibial advancement. Conversely, walking kinematics and kinetics did not change for slope descent. However, subjective feedback indicated that the participants perceived several benefits while walking downhill with the Proprio including feeling safer, feeling more support during rollover, and a reduction in the stress at the knee joint. The benefits of the Proprio during overground walking 8 and stair climbing 9 have also been reported. Unfortunately, no study has investigated the physiological consequences of the biomechanical changes an adaptive ankle provides.
It is well documented that individuals with a lower extremity amputation require more energy while walking than nonamputees.5,10 Normalizing the physiological demands is a goal for many device designers, and previous research has demonstrated new innovative prosthetic designs can improve gait performance for walking on slope surfaces.4,11 In studies comparing energy storing and return (ESR) feet with solid ankle and cushioned heel (SACH) feet, Casillas et al. 11 found ESR feet to lower the oxygen consumption by approximately 15%, and Macfarlane et al. 4 reported a decrease in the perception of walking difficulty. It is not known whether adaptive motion as provided by the Proprio device results in further reductions in metabolic cost or perceived walking difficulty compared to ESR feet. Therefore, the purpose of the study was to investigate the effect of a microprocessor-controlled ankle with adaptive ankle motion on metabolic energy expenditure during slope walking in persons with a transtibial amputation. We hypothesized the metabolic demands would be lower during slope ascent and descent with a device providing adaptive ankle motion when compared to an inactive version of the device and conventional ESR feet in people with a transtibial amputation.
Methods
Participants
Seven people with a traumatic unilateral transtibial amputation who had received or were currently receiving rehabilitation at a specialized care center for people with amputations volunteered to participate in this study. The individuals were aged between 25 and 37 years, able to walk without an assistive device on slopes for a minimum of 1 month prior to enrolling, and did not have any pain, cardiopulmonary, or musculoskeletal problems that would compromise the safety of testing. This study was approved by the Institutional Review Board at Brooke Army Medical Center, and all participants provided written consent prior to testing.
Data collection
A repeated measures design was used in which the participants underwent a physiological gait assessment while walking with their customary limb, the microprocessor-controlled device (Pon), and an identical Prioprio device in which the control unit was deactivated (Poff). In the Poff condition, the device performed as a standard low-profile ESR foot. A minimum of 3 weeks was provided between testing with each foot to allow for acclimation.
During testing, participants walked at three treadmill speeds (0.89, 1.11, and 1.34 m/s (2.0, 2.5, and 3.0 mph)) at each of three slope conditions (−5°, 0°, and 5°). Breath-by-breath oxygen consumption and heart rate data were continuously collected by a computer interfaced portable metabolic unit (K4b2, Cosmed, Rome, Italy), which was calibrated for gas concentration, turbine flow, and delay before each test according to manufacturer guidelines. Each stage lasted approximately 5 min to allow the participant to achieve physiological steady state. Averaged steady-state data from the final 2 min of each stage were used to calculate the metabolic energy expenditure (EE, J/kg/min). As is often reported, the EE was also expressed relative to the walking speed as a measure of the energy cost for walking (EC, J/kg/m). EC reflects the amount of oxygen consumed per meter traveled and is typically a U-shaped curve in which the minimum value reflects the most economical walking speed. 12 For persons with a transtibial amputation, the EC values plateau between 1.12 and 1.56 m/s, with the most economical walking at 1.34 m/s. 12 In addition, the walking difficulty was assessed using a modified 6–20 rating of perceived exertion (RPE) scale. 13 Prior to the walking stages, a baseline rest stage was completed for a minimum of 10 min. Rest stages were also completed between slope conditions and lasted approximately 20 min. The EE, heart rate, and subjective feedback were used at the conclusion of rest stages between slopes to confirm the participant returned to the pretest resting condition. The total time duration for each session was approximately 2 h.
Statistical analysis
Descriptive statistics (means and standard deviations) were calculated for basic participant data. Two-factor (prosthetic foot × walking speed) repeated measures analysis of variance (ANOVA) was used to compare the effect of the prosthetic feet on EE, and EC for each of the slope conditions. An analogous two-factor Friedman test was used for RPE data from each slope condition. Differences in the main effects were judged to be significant at p < 0.05. Follow-up pairwise comparisons for EE and EC were performed with Tukey t-tests and for RPE with Bonferroni adjusted Wilcoxon signed-rank tests. Statistical analyses were completed using SPSS v.19 (SPSS Inc., Chicago, IL, USA).
Results
Of the seven participants enrolled in this study, six completed all three test sessions. One participant completed two test sessions but moved from the local area and was unavailable for the final test session. Data from the remaining six participants who completed testing with all three devices (five males and one female) were used in the final analysis. Table 1 presents their demographic characteristics.
Participant demographics.
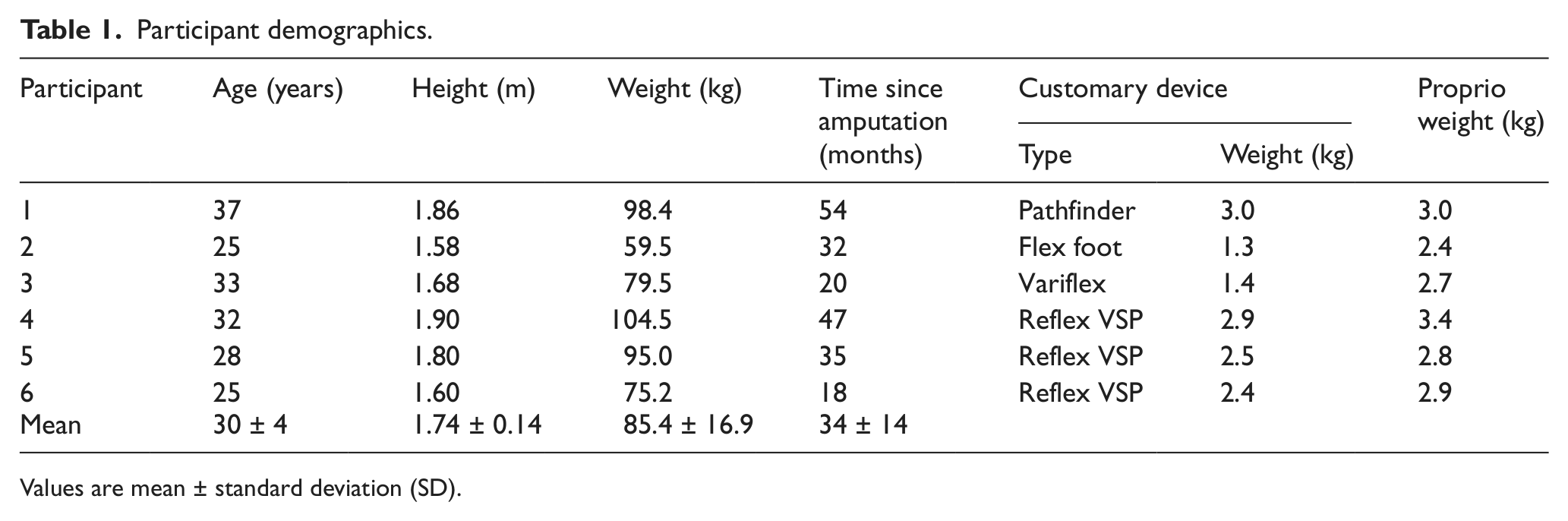
Values are mean ± standard deviation (SD).
For each of the six participants, the EE progressively increased with faster walking speeds for each of the slope conditions (Table 2). Statistical comparisons revealed nonsignificant interactions between the prosthetic foot type and the walking speed for each of the slope conditions. The main effect of interest, prosthetic foot type, was significant (p < 0.01) during slope descent. Post hoc testing revealed that the EE for walking with the customary foot was on average 13.5% higher for slope descent than with the Pon (p < 0.05) and 10.3% more than with the Poff (p < 0.05). This pattern of improvement with the Pon or Poff was uniform across the participants. A nonsignificant difference in the EE of approximately 3%–5% was found for post hoc comparisons between the Pon and Poff. No statistically significant differences were found for EE during level walking and, despite as much as 7% decrease for the Pon and Poff compared to the customary devices, for slope ascent. EE differed by less than 2% for the Pon and Poff during level walking and slope ascent.
Mean ± SD (range) for the metabolic energy expenditure (J/kg/min) of slope walking with each device.
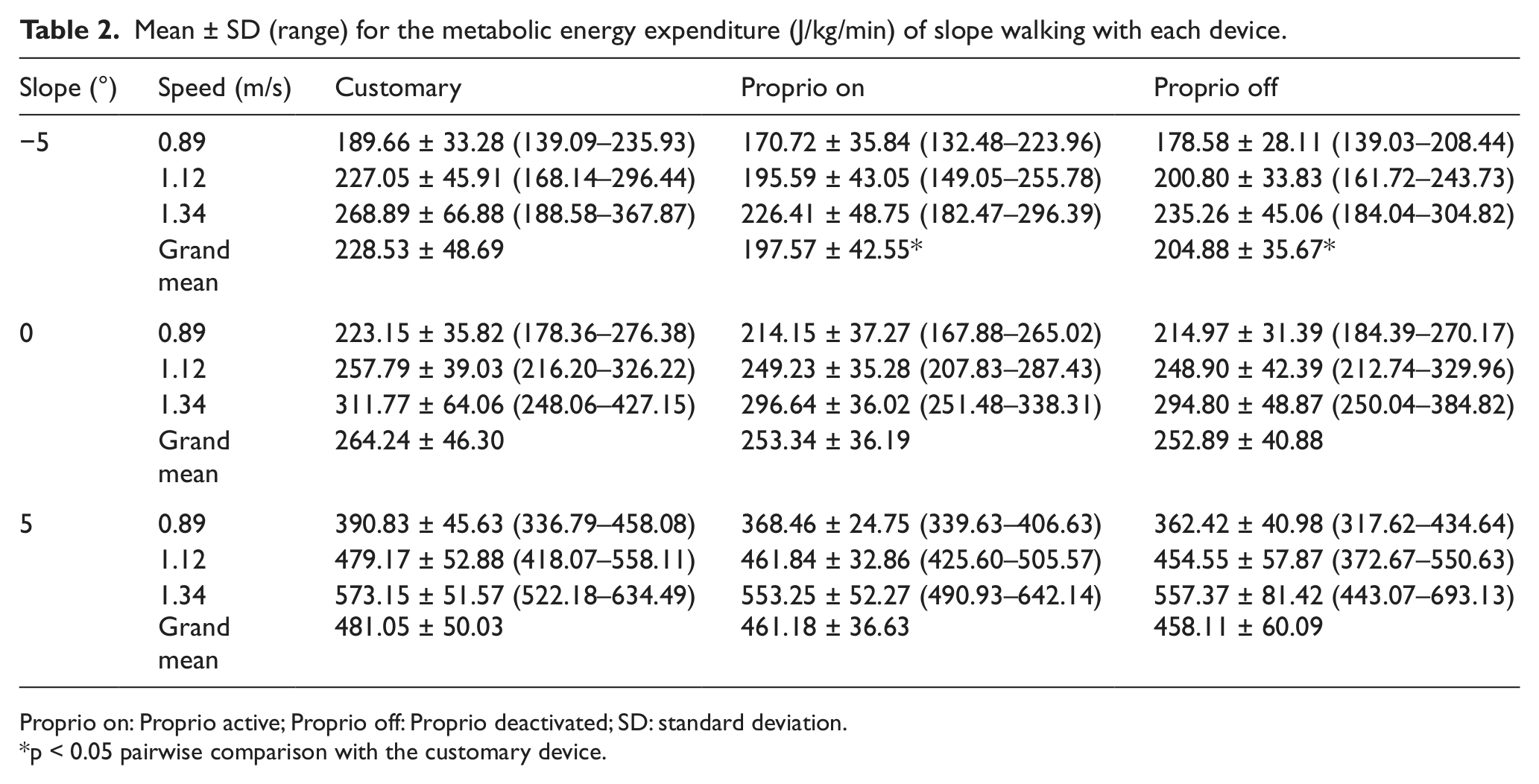
Proprio on: Proprio active; Proprio off: Proprio deactivated; SD: standard deviation.
p < 0.05 pairwise comparison with the customary device.
Mean EC values decreased (improved economy) as speed increased during slope descent and level grade walking. The lone exception being a small increase in the EC value during level walking with the conventional device between 1.12 and 1.34 m/s (Table 3). Individually, the most economical walking speed varied based on the prosthetic device and walking condition. Most frequently, the lowest EC value occurred at 1.12 m/s for one participant and 1.34 m/s for three other participants. The two remaining individuals exhibited essentially equal EC values for 1.12 and 1.34 m/s. Similarly, all participants exhibited the most economical walking at 1.12 or 1.34 m/s during slope ascent. However, mean values for the group did not reflect an overall improved EC as speed increased. For the three participants with a minimum EC value at 1.12 m/s, increases in EC values at 1.34 m/s were larger than observed between speeds during slope descent or level walking, and in effect countered the improved economy demonstrated by the three individuals with lowest EC values at 1.34 m/s. Consistent with EE, statistical testing revealed nonsignificant interactions for all slope conditions and a significant effect for the prosthetic foot type (p < 0.01) during slope descent only. Pairwise comparisons also revealed similar results with a less-economical gait with the customary feet compared to the Proprio devices (Pon 14.0%, p < 0.01, Poff 10.5%, p < 0.05) but no difference between Pon and Poff.
Mean ± SD (range) for the energy cost (J/kg/m) of slope walking with each device.
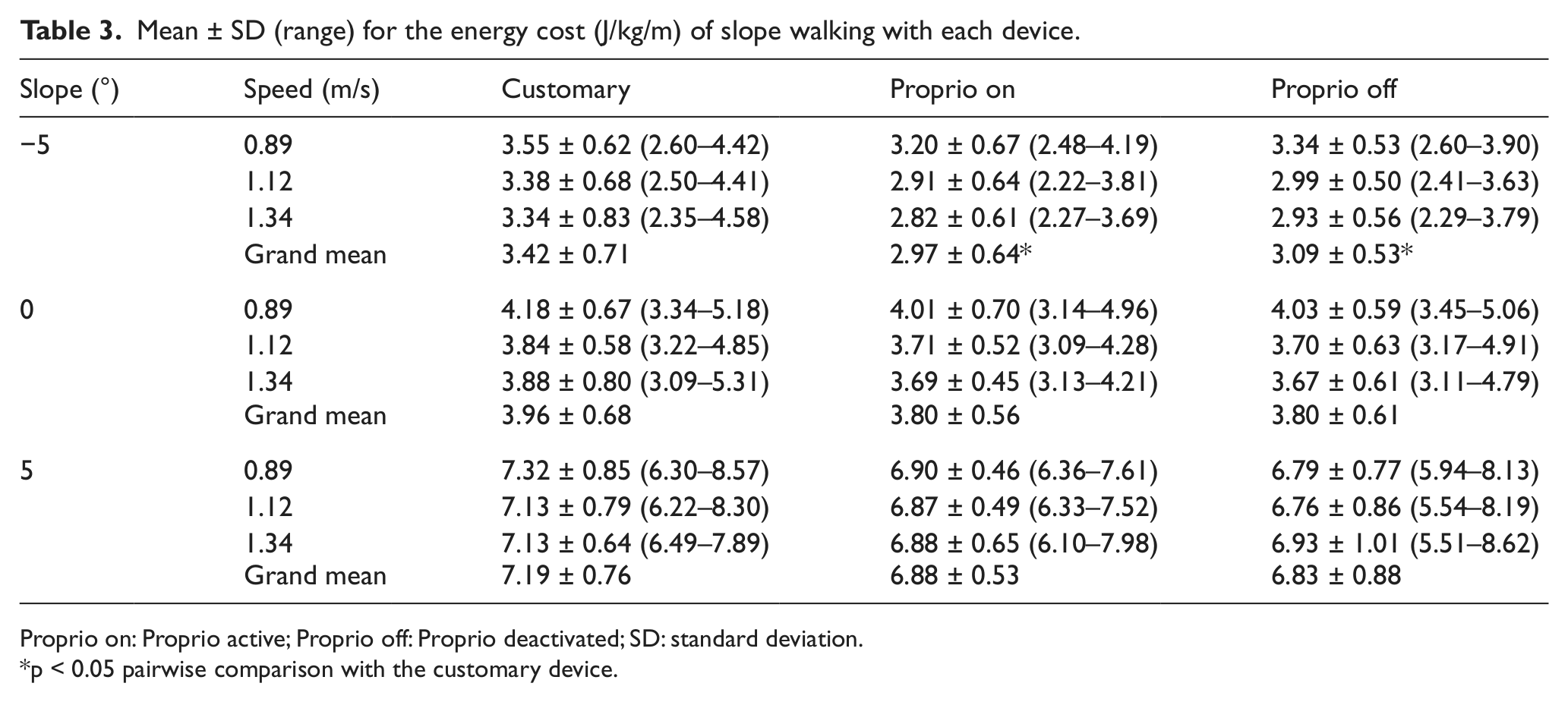
Proprio on: Proprio active; Proprio off: Proprio deactivated; SD: standard deviation.
p < 0.05 pairwise comparison with the customary device.
In a similar fashion to EE, each participant perceived the walking to become more difficult as the walking speed increased (Table 4). Results again revealed a significant device effect for slope descent (p < 0.01). RPE values decreased with the Pon by an average of 2.2 on the 6–20 scale when compared to the customary (p < 0.01) and 1.8 with the Poff compared to the customary device (p < 0.01). No significant changes in the RPE were found for level walking. Unlike the other study parameters, a significant device effect was found for slope ascent (p < 0.01). A decrease in the RPE of 1.4 with the Pon was significantly lower than the customary device (p < 0.01). The Pon was no different than the Poff for each walking condition.
Mean ± SD for the rating of perceived exertion (RPE) of slope walking with each device.
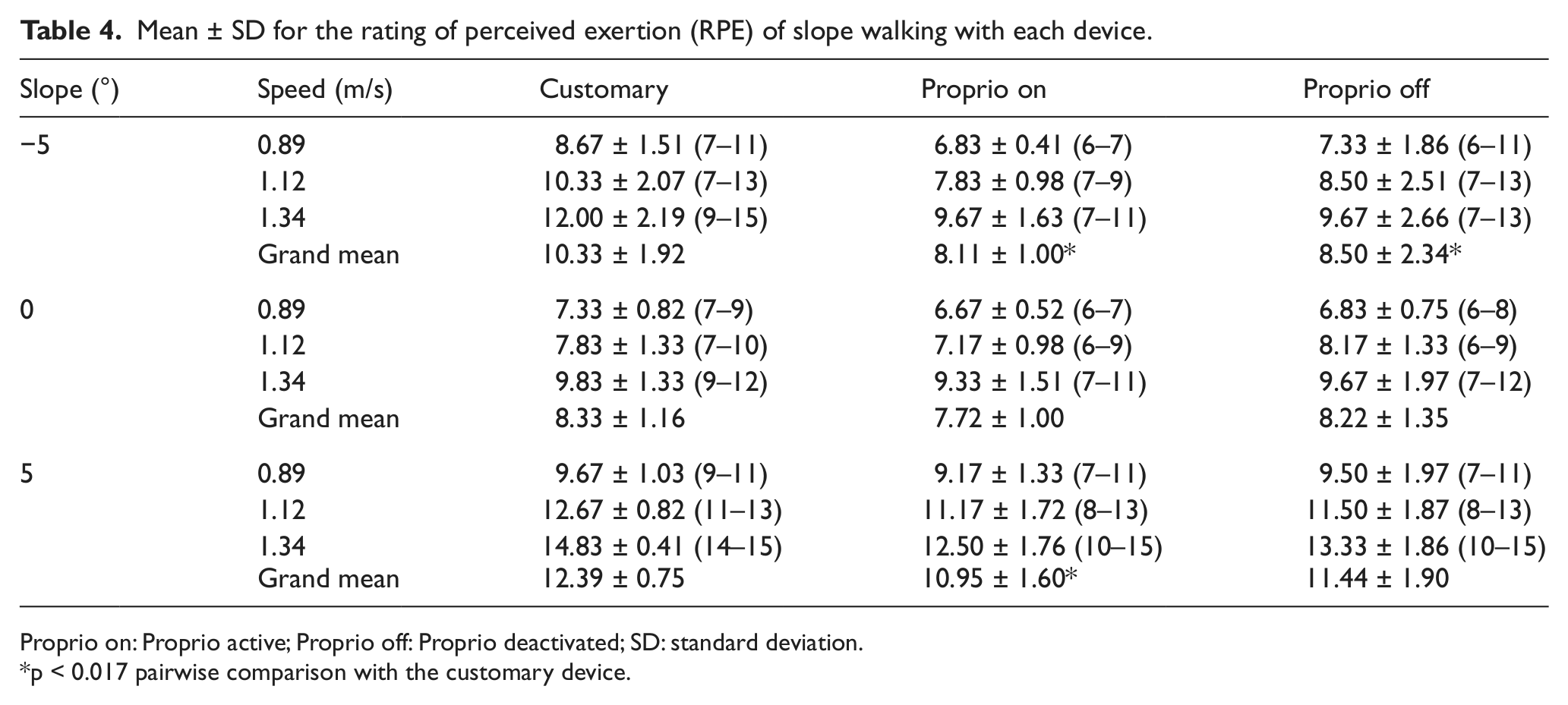
Proprio on: Proprio active; Proprio off: Proprio deactivated; SD: standard deviation.
p < 0.017 pairwise comparison with the customary device.
Discussion
The Proprio, a microprocessor-controlled prosthetic foot, was designed to improve gait performance by prepositioning the foot to accommodate walking on sloped surfaces and actively dorsiflex the ankle during swing phase to increase foot clearance. The results of the current study demonstrate that the adaptive ankle motion did not have a significant effect, but that the physiological demands of slope descent were 10%–14% higher with the customary feet.
For level walking and slope ascent, the adaptive ankle motion had a minimal effect on the physiological response. The mean values of the Pon and Poff conditions differed by less than 2%, which is not statistically different and unlikely to be clinically meaningful. 14 This result suggests the participants in this study either did not exhibit the kinematic and kinetic benefits observed in the Fradet et al.’s 7 study or the reported biomechanical changes have a minimal effect on the physiological effort of slope ascent. Comparisons between the Pon and Poff devices and the customary devices, however, revealed the EE for slope ascent was as much as 7% higher with the customary devices. Though nonsignificant, this trend suggests that there may have been consistent, though subtle, differences between the customary devices and the Proprio during slope ascent. A post hoc power analysis suggested that a statistically significant difference may have been observed with data from an additional 18 participants.
In the current study, EE for slope descent differed by a nonsignificant 3%–5% between the Pon and Poff. Results suggesting the adaptive ankle motion does not provide a meaningful improvement are consistent with the biomechanical analysis by Fradet et al. 7 The significant decrease in EE and EC for the Pon and Poff compared with the customary device was, however, unanticipated. In particular, we expected the Poff device would be similar to the customary device because the participants were using fixed ESR feet in both conditions. Finding a significant difference in EE between the devices suggests that factors other than the adaptive ankle motion were important in improving the physiological gait performance during slope descent.
Multiple factors could have contributed to the unexpected differences observed between the Proprio and customary devices. The increased and distally positioned mass of the Proprio device may have affected the participant’s physiological response. However, previous studies assessing the effect of limb mass on physiological gait performance reported no change or an increase in the EE with similar amounts of added and/or distally centered weight.15–18 These findings do not support mass as a likely contributor to the observed differences. Instead, differences in the mechanical properties, including heel and forefoot stiffness, 19 may have affected the participant’s walking mechanics and contributed to the observed changes.
In the Fradet et al.’s 7 study, a large dorsiflexion moment was observed during loading response and mid-stance, suggesting the heel of the Proprio was compliant. Feedback from prosthetists involved with the current study and anecdotal evidence from clinical gait analyses also suggest that the Proprio has a more compliant heel than the customary devices tested. Two explanations may provide a better understanding of how differences in heel compliance between the feet may contribute to the physiological effort. The first explanation relates to the transitioning of the body weight off the intact limb and onto the prosthetic device during initial contact and loading response. This step-to-step transition period has recently received significant attention, with research suggesting the magnitude of the impact or “collision” that occurs as the leading limb contacts the ground is important for redirecting the body’s center of mass and efficient walking.20 –22 During loading response, a stiff heel component could result in a collision that slows the body’s forward progression more than a compliant component (increased negative work) and could, therefore, increase the energetic requirements of the trail limb. The second explanation relates to the forward rotation of the shank (tibial progression) as the person progresses through the stance phase of gait. Ordinarily, the prosthetic heel compression allows the foot to simulate normal ankle plantarflexion. A stiffer heel component would result in an earlier tibial progression and could create a subjective feeling of falling forward during slope descent. Not surprisingly, RPE data suggest that slope descent is viewed to be as difficult or slightly more difficult than level ground walking even though the EE is lower (Tables 2 and 4). 4 Increased cocontraction in the residual limb knee musculature, 2 which would increase the EE, may be a compensation used to control shank position and provide overall limb support while walking with the customary devices. The participant’s potentially adopting a more stable gait pattern despite the added physiological cost is consistent with reports of young healthy nonamputees selecting a more stable gait pattern over an energetically optimal pattern while walking down moderate slopes. 23 Future research is needed to substantiate if increases in residual knee muscle cocontraction elevate the EE for walking.
The ESR properties of the prosthetic forefoot segment may have also contributed to the improvements. During preswing, energy that has been stored in the prosthetic foot during mid-stance and terminal-stance is released. This push-off is critical for the forward propulsion of the body during level or uphill walking. 24 Assuming similar forefoot properties, low-profile devices, such as the Proprio, would store and return less energy than full height customary devices because the keel does not extend up into a deformable shank. Consequently, the Proprio would provide lower ESR capabilities than the more compliant non-low-profile customary devices. 25 During level walking, a smaller push-off by the prosthetic limb increases the work requirements of the leading intact limb and the overall metabolic EE whereas a biomimetic push-off force decreases the step-to-step transition work.22,26–28 However, for descending slopes (5° or more), the trailing limb functions less to propel the body forward, instead acting more to brake against gravity. 24 Compliant feet or powered devices providing higher energy return at push-off may, in this manner, actually increase the leading limb collision and transitional work of walking during slope descent. Similarly, suboptimal stiffness characteristics can produce inappropriately timed energy return and increase the EE. 29 The ESR properties of the forefoot could also affect walking energetics by altering the foot rollover arc and effective foot length. Highly compliant forefeet shorten the foot rollover arc and effective foot length resulting in a loss of limb support (“drop-off”), 30 compensatory increases in the muscle activity, 25 and ultimately an increase in EE. 31
In this study, several differences in the design characteristics between the prosthetic feet may have contributed to the observed changes in physiological gait performance. However, several limitations identified in this study may have also affected the results. First, the participants were provided the prosthetic devices during the course of clinical care. Despite the intent to randomize the testing order, the conventional limb was tested first most often. It is possible that there was an order effect. However, all participants had performed multiple similar treadmill-based testing procedures prior to the current study as part of clinical care or participation in other research studies. Second, the alignment was not identical between tests. Research suggests misalignment of prosthetic devices can change the rollover shape of the foot. 32 However, the prosthetists involved in this study were highly experienced practitioners and likely aligned feet to achieve a similar “ideal” foot performance. 33 Finally, the added functionality of the Pon was described by the prosthetist to the patient, but no formal device-specific gait training was provided. Anecdotally, it did not appear participants dramatically changed their walking strategy with the adaptive ankle motion provided by the Pon. For example, it was noted that several participants displayed equal toe clearance between the prosthetic side and the intact side except for when walking with Pon. With the Pon, the toe clearance appeared greater with the prosthetic limb than the intact side. This observation suggests that the participants may have maintained their habitual gait pattern, even though an extended period of time was provided between tests to allow for acclimation to each prosthetic device. Unfortunately, motion capture techniques to quantify potential differences in toe clearance or other gait mechanics were not included. Nevertheless, it is possible that focused device-specific training would have been beneficial in modifying established gait patterns.34,35
Conclusions
In our study, adaptive ankle motion did not provide meaningful physiological benefit during level walking and slope ascent. However, walking with the Proprio (Pon or Poff) was less demanding than with a customary device for slope descent. Differences in the mechanical properties of the heel and forefoot potentially contributed to the improvements with the Proprio. Future research is needed to identifying optimal stiffness characteristics for prosthetic feet while walking on slopes. Furthermore, it would be useful for practitioners to include assessments of gait on nonlevel surfaces in order to better understand the implications of different prosthetic design features.
Footnotes
Conflict of interest
The authors affirm that they have no financial affiliation (including research funding) or involvement with any commercial organization that has a direct financial interest in any matter included in this article, except as disclosed in an attachment and cited in this article.
Disclaimer
The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, the Department of the Army, Department of Defense or the U.S . Government, or the National Institutes of Health.
Funding
Support for this project was provided by the Military Amputee Research Program and by CTSA award No. KL2TR000057 from the National Center for Advancing Translational Sciences.