
Abstract
Background:
Hyperkyphosis increases the risk of falls for elderly people by reducing postural balance. Spinomed orthosis and the posture-training support are two available options for improving postural balance but have never been compared.
Objectives:
To compare the effect of the Spinomed orthosis and the posture-training support on balance in elderly people with thoracic hyperkyphosis.
Study Design:
This study is a clinical trial on an accessible sample of elderly people with thoracic kyphosis.
Method:
Eighteen participants (16 women and 2 men), aged 60–80 years, with thoracic kyphosis greater than 50°, completed the study procedure. Subjects were randomly allocated to two groups, namely, Spinomed orthosis and the posture-training support groups. Sensory organization test and limits of stability were assessed using the EquiTest system and the Balance Master system, respectively. Balance score, directional control, and reaction time were measured to evaluate balance with and without orthosis in a random order.
Results:
In the posture-training support group, significant changes were observed in the studied balance parameters: balance score (p < 0.001), directional control (p = 0.027), and reaction time (p = 0.047). There was a significant change in balance score (p < 0.001) and directional control (p = 0.032) in the Spinomed group. However, there were no significant differences in the effect of the two orthoses, the Spinomed orthosis and posture-training support, on balance factors.
Conclusion:
Both Spinomed orthosis and posture-training support may improve balance in the elderly with thoracic hyperkyphosis in a similar manner.
Clinical relevance
Despite the importance of falls suffered by elderly people, not much attention has been paid to balance improvement and fall prevention while managing hyperkyphosis. This study evaluates the effect of the Spinomed orthosis and posture-training support on balance in hyperkyphotic elderly people. It provides some new insights into reducing the risk of falls for elderly people.
Background
Falling is one of the most important risks for elderly people that may be associated with serious consequences. 1 Studies in the United States considered falling to be the sixth cause of mortality in people older than 65 years. 2 About 30% of individuals aged over 65 years experience at least one fall per year, and the condition requires medical care in 20% of the cases.3,4
Postural stability, or balance, is the ability to maintain the center of mass (COM) within the limits of base of support. The COM is equal to the center of total body mass and is determined by finding the weighted average of the COM of each body segment. Movement of COM outside the limits of the base of support could result in postural instability and loss of balance. 5 Postural instability, which increases with age,6 –8 is one of the influencing factors of falls.8 –10 Changes in the spinal curve along with hyperkyphosis are among the main factors leading to postural instability.8,11,12 Most often, natural kyphosis in the thoracic spine increases with age. 13 Excessive increase in this curvature, also known as hyperkyphosis, is reported in 20%–40% of the elderly.14,15
Kyphotic posture may cause anterior displacement of the COM and instigate the COM to be located out of the limits of stability (LOS) in standing posture, 8 thereby increasing the risk of falls by reducing postural balance.8,12
Despite the importance of falls for elderly people, not much attention has been paid to balance improvement and fall prevention while treating hyperkyphosis. Using a spinal orthosis is a modality in the treatment of hyperkyphosis in the elderly. These orthoses help in improvement of balance and preventing falls16 –18 as well as correcting posture.16,19 –21 Pfeifer et al. 16 showed that the use of the Spinomed orthosis resulted in a decrease in COM sway and subsequently improved balance in elderly women. Sinaki and colleagues17,18 noted that using posture-training support (PTS) and getting involved in an exercise program can improve balance and decrease the risk of falls. However, no study has been carried out on the effect of PTS without an program; therefore, the isolated role of this orthosis has never been defined clearly. Although the Spinomed orthosis and PTS are the two best known and the least invasive orthotic management for correcting elderly people’s posture, with supporting studies to demonstrate their therapeutic effects on strength of back muscles, posture correcting, pain management, and improvement of balance,16 –18 there have been no other studies to compare these two orthoses. Therefore, this study aims to assess the effects of the Spinomed orthosis and PTS without exercise program on balance in the hyperkyphotic elderly population.
Materials and method
The subject population in this study taken as a sample comprised elderly persons between the ages of 60 and 80 years. Subjects with thoracic hyperkyphosis were recruited from nursing homes, orthopedic clinics, general practitioners, and elderly support groups. A total sample size of 18 was determined to be enough to provide an 80% power, after carrying out a pilot study on 5 participants using each of the two orthoses (total of 10 participants) and calculating the standard deviation of the balance score, as the main outcome measure. The balance score was considered in the role of the main outcome measure as it is a common and recommended criterion to evaluate the risk of falling,12,22,23 demonstrating an acceptable test–retest reliability and predictive validity. 24 Individuals with thoracic hyperkyphosis (with Cobb angle greater than 50°) on lateral spinal radiographs capable of walking without assistive devices and of standing independently for at least 2 min were included. The exclusion criteria were as follows: alcohol or drug use affecting balance or influencing central nervous system (within 48 h before testing); history of neurogenic or myopathic disorders impairing sensory or motor functions; scoliosis; any history of joint arthroplasty in lower limbs; having visual and auditory disorders not correctable by glasses or hearing aids; history of fracture or surgery of spine or lower limbs within at least 1 year before the study; history of participating in spinal balance exercises (within a month before testing); and back or neck pain at the time of examination reported to be higher than 3 on the Visual Analogue Scale (VAS), because lower pain intensity on VAS does not affect postural sway in patients. 25 This study was a single blinded clinical trial with a convenience sample of 18 elderly persons with thoracic hyperkyphosis. All the participants voluntarily signed an informed consent form. The study procedure was approved by the Ethics Committee of the institution in which the study was conducted (Letter No. 221).
The immediate effect of wearing Spinomed orthosis and the PTS on postural balance was evaluated in this study. These two orthoses are the best known and least invasive orthotic recommendation for dorsal kyphosis in elderly. 26 The Spinomed orthosis consists of an abdominal pad; posterior padded metal upright; and pelvic, waistline, and shoulder straps. According to the manufacturer’s guideline, the posterior padded metal upright extends cephally up to the 1–5 cm under C7 and extends caudally down to the coccygeal level. 27 According to the patient’s spinal curvature, the middle part of this metallic upright is shaped without applying any heat; the pelvic, waistline, and shoulder straps are also adjusted to fit the patients’ size. The orthosis weighs approximately 450 g (Figure 1).

The Spinomed orthosis consists of an abdominal pad; posterior padded metal upright; and pelvic, waistline, and shoulder straps. The posterior padded metal upright extends cephally up to the 1–5 cm under C7 and extends caudally down to the coccygeal level.
The PTS orthosis consists of a posterior bag, which is 10–20 cm in length and 5–10 cm in width. The bag is placed exactly under the inferior angle of the scapula.26,28 Three 110 g weights and a 440 g weight are placed in this bag. The PTS in this study was provided by Trulife, and the weights were adjusted according to the recommendations in the guideline of Sinaki’s 28 patent (Figure 2).

Posture-training support consists of a posterior bag that is 10–20 cm in length and 5–10 cm in width. The bag is placed exactly under the inferior angle of the scapula.
Both of the orthoses were fitted on the participants by a certified orthotist who adjusted the straps with the same tension in all participants. Balance assessment in this study was performed by scores of sensory organization test (SOT) and the LOS test. A SOT was performed using the NeuroCom EquiTest system according to the manufacturer’s protocol.
29
The system consists of two force plates, placed parallel to each other and connected by a pin joint and delimited by a visual surround in three directions (front, left, and right) as follows: The two force plates are supported by four force transducers established symmetrically on a supporting plate. A fifth transducer is bracketed to the center plate directly beneath the pin joint.
29
The load cells in the force plates transmit force information to the computer 100 times per second. The SOT evaluates the subjects’ ability to effectively use visual, vestibular, and somatosensory inputs to maintain balance. In this test, the average three balance scores gathered from six test configurations were used to calculate the total score, which ranged between 0 and 100. Score 0 indicates highest level of impairment and imbalance, whereas score 100 shows the individual’s total independence.22,23,29
The LOS test was performed by the NeuroCom Balance Master according to the manufacturer’s protocol.
29
The system consisted of two parallel force plates. Vertical forces applied by the subject’s feet, the location of COM, and its relative movement were measured and reported by four force transducers placed under the plates as follows: The transducers are mounted along the front-to-back center line of each plate (one 29.25 inches behind and the other 29.25 inches in front of the pin joint.) The lateral distance between left and right plate transducers and center is 8.25 inches.
29
Visual feedback about COM was provided for subjects through a monitor. 29 The LOS test evaluates the subject’s ability of volitional control of COM. In this study, the measured quantities in LOS test were reaction time and directional control. The reaction time (microseconds) is the time required for the patient to respond to a visual stimulus. Directional control (%) is “the accuracy of movement from the central square to the target and reported in percentage”; 30 a score of 100 shows that the patient’s movement toward the target had occurred in a straight line.
In this study, balance was evaluated by measuring the balance score, reaction time, and directional control. The previous studies have established the association between risks of falls and balance score and LOS test scores;22,23,31 moreover, validity and reliability of balance score, reaction time, and directional control have been confirmed in earlier studies.24,32
Protocol
Subjects selected based on the study’s inclusion and exclusion criteria were provided with sufficient information regarding the research aim and procedure. A spine specialist evaluated the participants and measured the Cobb angle. On a standing lateral radiographic image of the thoracic spine, two lines are drawn, one along the upper surface of the T4 (4th thoracic) vertebral end-plate and one along the lower surface of the T12 vertebral end-plate. Two perpendiculars are drawn to these two lines, and the angle at their cross-point is measured with a protractor. Subjects who had Cobb angle >50° were included.
Recruited subjects were randomly allocated to use either the Spinomed orthosis or PTS. The randomization procedure was to pick the name of the orthosis from a bag including the names of both orthoses. Before measuring the baseline measurements, the height and weight of all subjects were recorded. The participants were informed about the test procedure and were given enough time to learn the correct method of test performance. SOT and LOS balance tests were performed with and without orthosis. The sequence of tests in these configurations was random in order to limit the effect of learning and fatigue: 1-h interval was considered between trials with and without orthosis and 10-min rest between SOT and LOS tests. All subjects in the two groups were asked to wear the orthoses for 1.5 h to get used to them. Pfeifer et al.’s 16 study noted that Spinomed orthosis must be worn approximately 2 h/day, and Sinaki et al. 17 in their study recommend to wear the PTS daily for 1.5 h in the morning and 1.5 h in the afternoon, and therefore, in this study, 1.5 h was considered as a suitable orthotic adaptation time. In performing the SOT test, the subject was asked to stand on the force plate of EquiTest system and put his or her feet on certain points on the force plate and look straight forward through his or her visual limit. This test was performed in six different sensory configurations, each repeated three times. The force plate was stable in stages 1–3. In stage 1, subject’s eyes were open; in stage 2, subject’s eyes were closed; and in stage 3, the visual surround in front of subject was moving. The force plate was moving from stages 4 through 6, and the visual condition was the same as the three first stages. With regard to the speed of the tilt in the force plates, sway gain setting of 1 was chosen. In sway gain setting of 1, force plates follow the patient’s sway exactly, and normative data are only available for this sway gain. 29 In order to eliminate any learning effect, sequence of these stages was entirely randomized. Each testing stage lasted for 20 s. 29
In performing the LOS test, the subject was asked to stand on the force plate of the Balance Master system, hanging his or her arms at the sides in a comfortable position, and putting his/her feet on certain points on the force plate and positioning the pointer that appeared on the monitor showing the position of the COM in the central square on the monitor. In addition to the central square, there were eight peripheral squares, which showed the subject’s LOS up to 100%. In each stage, one of these squares was determined by yellow color, and starting of movement was indicated when a blue circle appeared in the target square. The patient was asked to move pointer toward the target square, rapidly and carefully, by shifting body weight and using an ankle strategy without displacing his or her feet placement on the force plate and keeping the pointer in that position until the blue circle disappeared. Each testing stage was selected randomly and lasted 8 s, after which the pointer disappeared. 29 Reaction time and directional control were the variables evaluated in each stage. NeuroCom systems include a self-calibration feature, which calibrates the system on start of the application. This will make it unnecessary to calibrate the system manually unless in the case of changing the position of the force plates, which is performed with the NeuroCom system Init utility provided with version 7 system software, according to the manufacturer’s recommendations. 29
Data analysis
Data analysis was performed with the SPSS software (version 16). The Kolmogorov–Smirnov test was used to test the normality of distribution of variables. Normal distribution was observed for variables in both groups. Independent sample t-test was used to evaluate the groups’ congruency for height, age, weight, degree of kyphosis, and balance parameters. Balance parameters within the groups (i.e. with and without orthosis) were compared using a paired t-test with and without orthosis. To compare the changes in balance parameters between the two groups, an independent sample t-test was used. A p-value <0.05 was considered to be statistically significant.
Results
Eight participants were allocated to the PTS group and 10 participants were allocated to the Spinomed orthosis. The inequality of the size of each group was related to the group allocation method as describe earlier. In total, 16 women and 2 men with the mean age of 66.72 ± 4.77 years, height of 156.33 ± 6.43 cm, weight of 66.88 ± 9.68 kg, and Cobb angle of 70.61° ± 9.87° participated. The statistical analysis (independent sample t-test) revealed no significant difference in subject’s age (p = 0.06), weight (p = 0.391), height (p = 0.406), angle of kyphosis (p = 0.959), balance score without orthosis (p = 0.443), directional control without orthosis (p = 0.118), and reaction time without orthosis (p = 0.141) among two groups on baseline measurement. The use of Spinomed orthosis had a significant impact on both the balance score (p < 0.001) and directional control (p = 0.032) but not the reaction time (p = 0.29) (Table 1).
The mean (± SD) for balance parameters in Spinomed group (without and with orthosis).
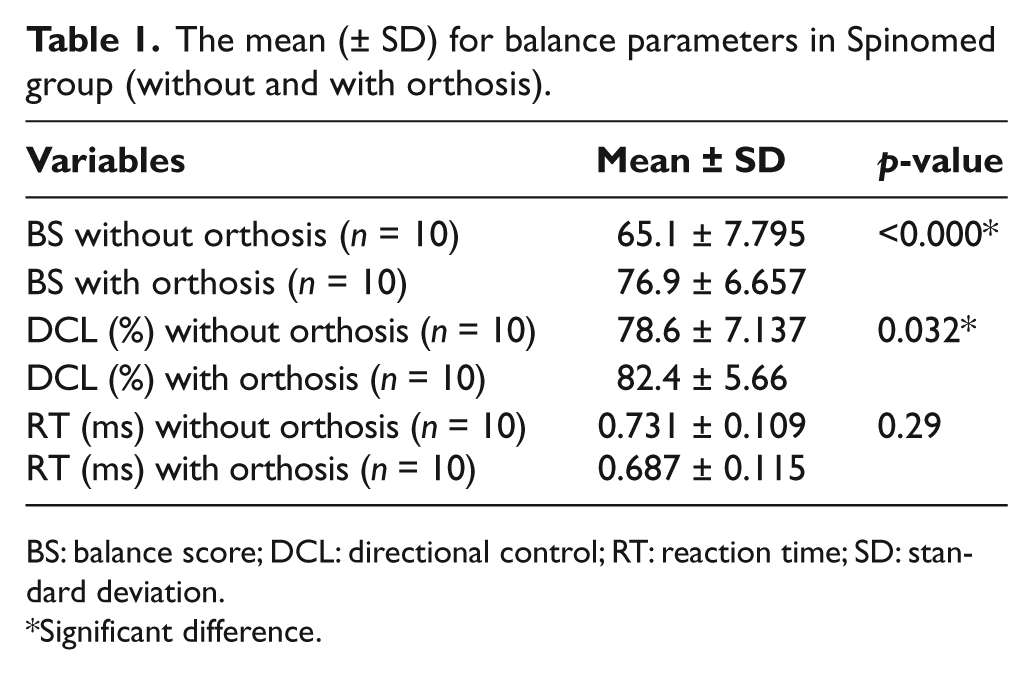
BS: balance score; DCL: directional control; RT: reaction time; SD: standard deviation.
Significant difference.
The use of PTS, however, had a considerable effect of using this orthosis on all the three studied variables (balance score (p < 0.001), directional control (p = 0.027), and reaction time (p = 0.047); Table 2). There were, however, no significant differences between the effects of Spinomed orthosis and the PTS on total balance score (p = 0.583), directional control (p = 0.791), and reaction time (p = 0.152) (Table 3).
The mean (± SD) for balance parameters in PTS group (without and with orthosis).
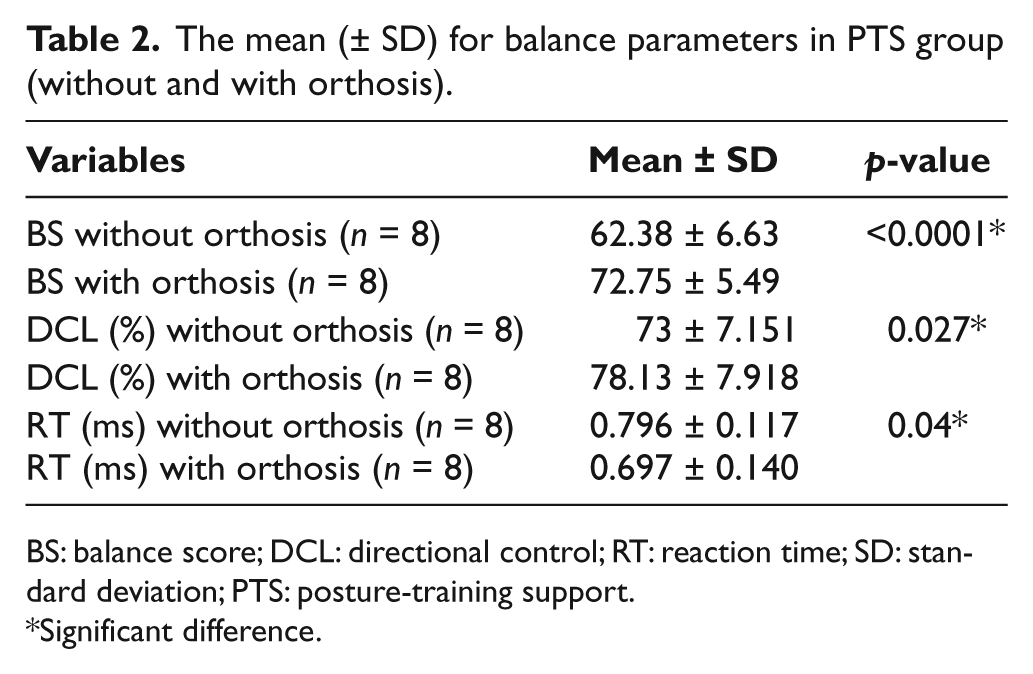
BS: balance score; DCL: directional control; RT: reaction time; SD: standard deviation; PTS: posture-training support.
Significant difference.
The mean (± SD) for comparing the changes of balance parameters between the two groups (Spinomed and PTS).
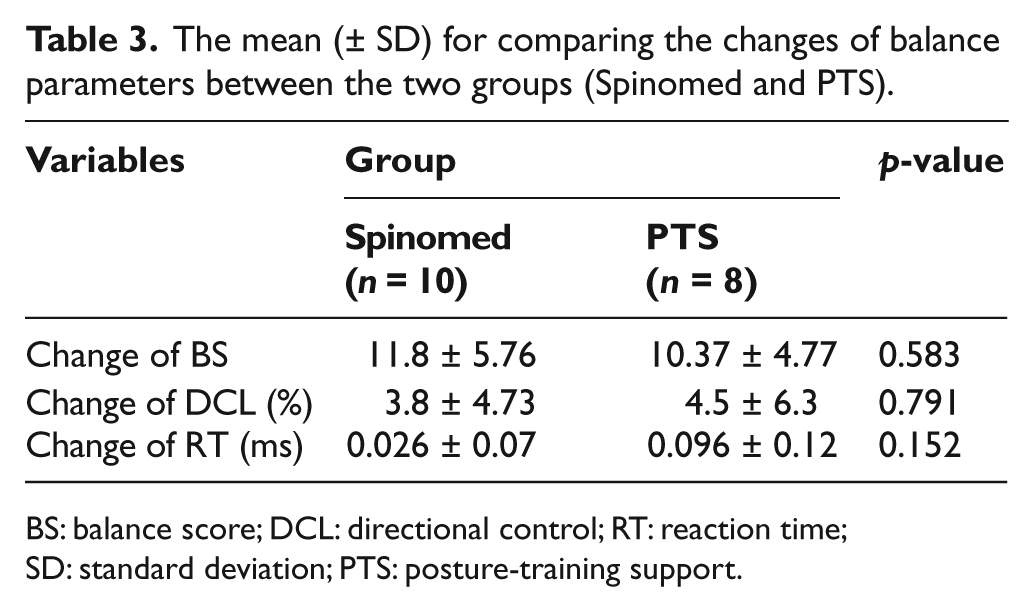
BS: balance score; DCL: directional control; RT: reaction time; SD: standard deviation; PTS: posture-training support.
Discussion
This study aimed to compare the effect of PTS and Spinomed on balance in elderly people with thoracic kyphosis. In order to determine the net effect of the orthoses, no exercise was included in the protocol. Other researchers also considered the effect of orthosis without performing any exercise. 16 This may reveal the pure effect of orthosis. However, as it is common to prescribe the combination of the orthosis and exercise, the interpretation of results of this study should be considered with caution in this regard.
The results revealed an increase in the balance score following the use of both of the studied orthoses. This finding indicates the positive effect of these devices in improving postural stability and balance. This is in line with Pfeifer et al.’s 16 study on 62 elderly women with osteoporosis and hyperkyphosis, which also reported that the use of the Spinomed orthosis without engaging in any exercise programs resulted in a decrease in COM sway and subsequently improved balance. However, in studies by Sinaki et al.17,18 on elderly women with osteoporosis and hyperkyphosis, the improvement of the balance score was referred to the using of PTS and getting engaged in sport programs. Putting together the studies of Sinaki et al., Pfeifer et al., and this study reveals that the improvement of balance in the Sinaki et al. studies might have been achieved as a result of using the orthosis, and not because of the exercise program, or at least the orthosis had an effect on improvement of balance in the subjects studied. Proprioception change is often considered as one of the main consequences of orthosis use. 26 These devices increase proprioception through increasing skin inputs.33 –37 This is caused by increasing the activity of not only the afferent receptors in the skin but also the mechanoreceptors through increased pressure on muscles and the articular capsule. Newcomer et al. 34 and McNair et al. 33 showed that lumbosacral corsets improve proprioception and lower repositioning errors by causing more afferents in the case of body position. Increased awareness about spinal position also prevents erroneous postures and reduces stress on spine.33,34 The correction of forward inclination and helping the COM to be placed within base of support are among other mechanisms identified for Spinomed orthosis and PTS.17,18,26 Hyperkyphotic posture displaces COM forward so that it falls out of LOS and, consequently, cause imbalance.10,12 Thus, these orthoses are designed to counteract these deforming forces; in the PTS, this mechanism works by applying force under the scapula, whereas the Spinomed orthosis retracts the shoulders through shoulder straps. 26 Therefore, these orthoses generate extension moments on the spine, displace the COM backwards, and maintain it within base of support, as a result, improving balance and decreasing falling risk.16 –18
In the LOS test, use of the PTS and the Spinomed orthoses is associated with an increase in the degree of directional control, implying better balance capabilities and less falling risk. Palumbo et al., 30 in their study on examining the effects of backpack on dynamic stability in standing position in 50 healthy university students, showed that carrying a backpack increases directional control in the frontal plane but lowers it in the sagittal plane. These changes demonstrate no lateral bending when carrying bags on both sides; forward bending, however, is significant in these cases. 38 Thus, postural compensations in the sagittal plane may be more considerable than in the frontal plane. In order to compensate for the changes in COM, caused secondary to the backpack weight, postural changes such as forward bending occur so that these changes may alter activation modes of anterior and posterior muscles to maintain dynamic balance. These changes in the activation mode of the muscles may explain the reduction noted in anterior and posterior directional control. Liaw et al. 39 showed that Knight–Taylor orthosis is associated with decreased directional control in individuals with osteoporosis and compressive vertebral fractures. These results are contrary to the findings of this study due to the different characteristics of applied orthoses between two studies. Liaw et al. used Knight–Taylor orthosis, which is a rigid spinal orthosis and limits functional activity, so that its utilization for a long time can result in atrophy of abdominal and spinal muscles. However, it is supposed that the Spinomed and PTS orthoses, activate spinal muscles better and increase their isometric strength.16,40 These orthoses, unlike conventional rigid braces, cannot maintain spine in an upright posture but encourage people to keep their spines upright using spinal muscles. 26
In this study, the use of Spinomed orthosis did not significantly affect the reaction time. PTS, however, reduced the reaction time. The visual reaction time is the time interval between observing visual stimulus and the start of the attempt to displace the COM toward the determined target by the patient. 29 Although these orthoses may not be influential on the first part of the nervous pathway that dispatches the information related to observing a visual stimulus to the brain cortex, they would be effective on the second part, that is, attempting to displace the COM toward the determined target. Therefore, the orthosis increases the muscle tone through increasing the activity of the skin receptors and consequently, enhances awareness of body position in space. This would improve the person’s safety and lower reaction time. In theory, it is expected that both orthoses will reaction time. This expectation is supported in the group with the PTS, but reaction time did not change in the Spinomed orthosis group. This may be as a result of the structure of this orthosis because the pelvic straps that are located under the hip may resist hip joint movement and, consequently, limit hip function, thereby reducing the speed of reaction while the PTS orthosis does not induce any limitation in the hip area.
Study limitations
A control group that uses a placebo orthosis could have been employed to determine the net effect of the interventions; however, due to the nature of orthotic intervention, employing a control group and developing a real placebo orthosis is not convenient. The other limitation of this study was the duration of the intervention. Due to the time limit of the study, it was not possible to assess the long-term effects of the intervention; thus, the results should be considered with caution as immediate effects of the intervention have been studied.
Conclusion
It could be concluded that the Spinomed orthosis and PTS are both effective in improving balance in hyperkyphotic elderly people. It should be stressed that, based on our results, there is no significant difference in the efficacy of these two orthoses in improving balance factors.
Footnotes
Conflict of interest
We certify that no party having a direct interest in the results of the research supporting this article has conferred, or will confer, a benefit on us or on any organization with which we are associated.
Funding
This study was fully funded by Tehran University of Medical Sciences (grant No 813). The protocol of this study was approved by the Ethics Committee of the institution in which the tests were conducted (Letter NO. 221).