
Abstract
Background:
Ankle-foot orthoses are usually used in combination with footwear. Shoe design can have a significant effect on kinematics of the lower limb joints and line of action of the ground reaction force during walking. But, ankle-foot orthosis–footwear combination is not appropriate for indoor barefoot walking in some Asian cultures. In this study, we have modified a solid ankle-foot orthosis in order to set it in the same position as a solid ankle-foot orthosis–footwear combination.
Objective:
To investigate the effect of a modified solid ankle-foot orthosis; a solid ankle-foot orthosis which can be locked in different positions on gait and balance performance in comparison with a conventional solid ankle-foot orthosis, a common solid ankle-foot orthosis–shoe combination in asymptomatic adults.
Study Design:
Cross sectional.
Methods:
Two standard solid ankle-foot orthoses were manufactured with the ankle joint in neutral position. Then, one of these solid ankle-foot orthoses was modified in order to allow locking in a different alignment. Walk across, limit of stability, and sit-to-stand tests of the balance master system were performed while participants wore the modified solid ankle-foot orthosis aligned in 5°–7° anterior inclination without a shoe and a conventional solid ankle-foot orthosis–shoe combination.
Results:
There was no significant change in walking speed, step length, and step width with the conventional and modified solid ankle-foot orthoses. In addition, movement velocity and maximum excursion of the center of gravity during the limit of stability test were not different, although the maximal forward excursion of the center of gravity was longer when wearing the modified solid ankle-foot orthosis compared to the conventional solid ankle-foot orthosis–shoe combination (P = 0.000). Sway velocity of the center of gravity did not change during the sit-to-stand test.
Conclusion:
The results demonstrated that the modified solid ankle-foot orthosis had the same effects as the conventional solid ankle-foot orthosis–shoe combination on the gait and balance performance of asymptomatic adults.
Clinical relevance
The findings of the present study can be used as the basis for further investigations on the efficacy of the modified solid ankle-foot orthoses in different neuromuscular populations in order to help people who do not wear shoes at home, as is the custom in some Asian cultures.
Background
A person who is suffering from an injury to the central or peripheral nervous system often experiences alternations in the walking ability, postural stability, and balance.1–3 Literature findings suggest that ankle-foot orthoses (AFOs) can be used in the management of different neuromuscular and lower limb disorders. AFOs had positive effects on spatiotemporal gait parameters, kinematics, balance, and energy costs.4–8
Solid ankle-foot orthoses (SAFOs) are the most commonly applied AFOs for people with neuromuscular disorders such as cerebral palsy, 9 postural instability, 10 and excessive ankle plantar flexion 11 in order to provide safe ambulation by improving mediolateral stability in stance phase, facilitating toe clearance during swing phase and decreasing body sway. 12
AFOs are used in combination with footwear. 13 Shoes can control foot movements of all directions through the ground reaction force (GRF). The role of the shoe becomes at least equal to that of the orthosis during weight bearing throughout the gait cycle, since shoe design can have a significant effect on kinematics of the lower limb joints and alter the line of action of the GRF during the gait cycle. 14 So, an appropriate AFO–footwear combination would realign the GRF to optimize the biomechanical alignment of the lower limb in order to improve kinetics and kinematics of gait. 14 A proper heel raise (heel height) of a shoe used in conjunction with an AFO may modify the shank to vertical angle (SVA). The SVA is the angle formed by the shank of the tibia, to an imaginary line perpendicular to the ground. 15 The SVA and the orientation of the GRF have been suggested as key indicators for tuning. 11 An inclined position of the shank places the knee joint center over the center of the foot and creates a stable distal support mechanism as well as contributes to stability in stance. 16
Previous studies advocated that the combination of shoes and orthoses can have positive effects on improving gait parameters and balance performance.13,17,18 According to the clinical experience, some neurological disorders such as stroke seem highly susceptible to small changes in the alignment of their AFOs or to small changes in the design of the footwear. 19
On the other hand, footwear is not used indoors in some Asian countries. Therefore an AFO–footwear combination is not appropriate for indoor barefoot walking. Then patients often use AFOs without any footwear at home in those cultures such as Iran . In some societies, anterior AFOs have been used as they are appropriate for walking barefoot indoors as well as for walking with shoes.20,21 It has been reported that wearing anterior AFOs were as useful as posterior AFOs for correcting hemiplegic gait. 22 However, the anterior AFO has been recommended for patients who need more ankle movement to adjust their upright posture. 21 Therefore, an anterior AFO is not suitable for patients who need to wear a SAFO, since SAFOs are designed to provide a high degree of control to ankle-foot complex movements. 23 In this study, it was hypothesized that if we kept the ankle alignment of the SAFO in the same position when wearing a SAFO with and without a shoe, it may have the same effect on gait and balance performance indoor (without shoe) and outdoor (with shoe) in those societies.
Therefore, the purpose of this study was to investigate the effect of the modified SAFO, which can be used with and without shoe on gait and balance characteristics in comparison with the conventional SAFO, a standard SAFO that was used in combination with footwear—in asymptomatic adults. It has been suggested that there is only a small range of SVA where it is possible to incline the thigh in order to improve kinetics and kinematics of gait and preserve balance during walking. It is 7°–15° inclined. 16 Although the SVA of 10°–12° incline is the optimum position of the shank specifically in children using the AFO–footwear combination, 16 it may not be possible to set the ankle angle of the AFO at both neutral (i.e. 90° between the tibia and the foot) and 10°–12° inclination of the tibia in participants with neuromuscular problems. As a result, the minimum degree (5°–7° inclination of the tibia) has been used in the current study. In addition, the efficacy of the modified SAFO was examined in healthy participants in order to test the theory that this modification of the SAFO may have the same effect as the conventional SAFO on gait and balance performance. Therefore, this theory should be examined before applying the modified SAFO to patients who wear an AFO without shoes inside their houses.
Methods
Participants
Healthy participants were recruited to participate in this study. Selection of asymptomatic participants was based on the following exclusion criteria: previous head injury resulting in a loss of consciousness, 24 history of lower extremity injury occurring within the past year, 25 pregnancy, 24 severe malalignment of lower limb such as genu valgum or varum, and fracture or dislocation of the lower limb within the last 6 months and history of any orthopedic surgery. 26 The study was approved by the Institutional Review Board (IRB) of Teharn University of Medical Sciences. The participants provided informed consent in accordance with the procedures outlined by the IRB and were informed that they could withdraw from the study at any time.
AFO fabrication
A trained orthotist manufactured two standard custom-made SAFOs for the same leg (nondominant limb) of all participants. The participant’s dominant leg was determined based on the limb that the participant used in at least two of the three following tests: step-up, balance recovery, and kicking a ball through a gate.24,27 The SAFO was manufactured from 0.4 cm thick polypropylene and it extended proximally to below the neck of the fibula. It was trimmed to the middle of the medial/lateral malleoli and secured with an upper strap across the proximal tibia. 10 The medial/lateral trimlines of the footplate were terminated proximal to the metatarsophalangeal (MTP) joints and the plantar surface of the footplate extended to the tips of the toes.
The ankle joint of both SAFOs were set in a neutral position. Afterward, one of these AFOs was cut across the rear of the ankle in order to attach a metal bar vertically. This metal (stainless steel) bar had holes that allowed locking of the modified SAFO in two different positions (Figure 1). First, the modified SAFO was locked in a neutral position inside the shoe for use outdoors. When the modified SAFO in the neutral position was placed in the footwear, the calf section was inclined 5°–7° anteriorly because of the difference in heel to forefoot sole thickness of the footwear. The shoes were the same sport type for all the participants with an approximately 1 cm heel height (i.e. the difference in thickness between the heel and sole). 19 Second, the modified SAFO without a shoe was locked in 5°–7° anterior inclination to imitate the alignment of the calf section in the conventional SAFO–footwear combination. The distance of these holes on the metal bar was calculated based on the tangent equation (tan θ = (Y/X), where Y is the distance of the next two holes and X is the length of the plantar surface of the shoe). Finally, the alignment of the modified SAFO without shoe was checked by a manual goniometer while participants stood upright. A removable strap was used across the ankle joint when participants wore the modified SAFO without a shoe. A pair of socks with specific material on the plantar surface was also used in order to prevent slipping. Each participant performed all measurement tests: wearing the modified SAFO aligned in 5°–7° anterior inclination without shoe and the conventional SAFO–shoe combination. The modified SAFO has been compared to the conventional SAFO in order to identify differences between the conventional and modified SAFO. Participants were instructed that they could rest as necessary during the test and testing order was randomized.

A modified solid ankle-foot orthosis, which can be locked in 5°–7° of anterior inclination and neutral position.
Equipment and measurement
The Balance Master System (version 8.0.3, Neurocom International, Inc., Clackamas, OR, USA) was used to test dynamic standing balance.7,28 Limit of Stability (LOS) and sit-to-stand (STS) test protocols were used to record the participants’ dynamic balance. The main purpose of the present study was to help people who wear SAFOs without shoes at home. Most indoor activities require weight shifting in various directions without losing balance. In addition, standing from a chair is included in activities of daily living. So the LOS and STS test protocols have been selected in order to reflect the effect of the modified SAFO on balance performance inside the house in comparison with the conventional SAFO.
The LOS test was performed requiring participants to control their center of gravity (COG) by weight shifting. The location of the participant’s COG was displayed on the screen as a cursor. This test evaluates the ability to control movement and speed of the COG in one of four directions that is, forward, backward, AFO side, and sound side in order to evaluate this ability during tasks that require weight transfer in different directions without losing balance, stepping, or reaching for assistance. 29 The participants were instructed to stand on the force plate (0.45 m × 0.45 m) with their arms at their sides and to not move their feet throughout the testing procedure (Figure 2). Movement velocity was the average speed in degrees per second of the rhythmic COG movement along the specified direction. Maximal excursion was measured as the distance of the COG movement toward the selected target, expressed as a percentage of maximum LOS distance.30,31
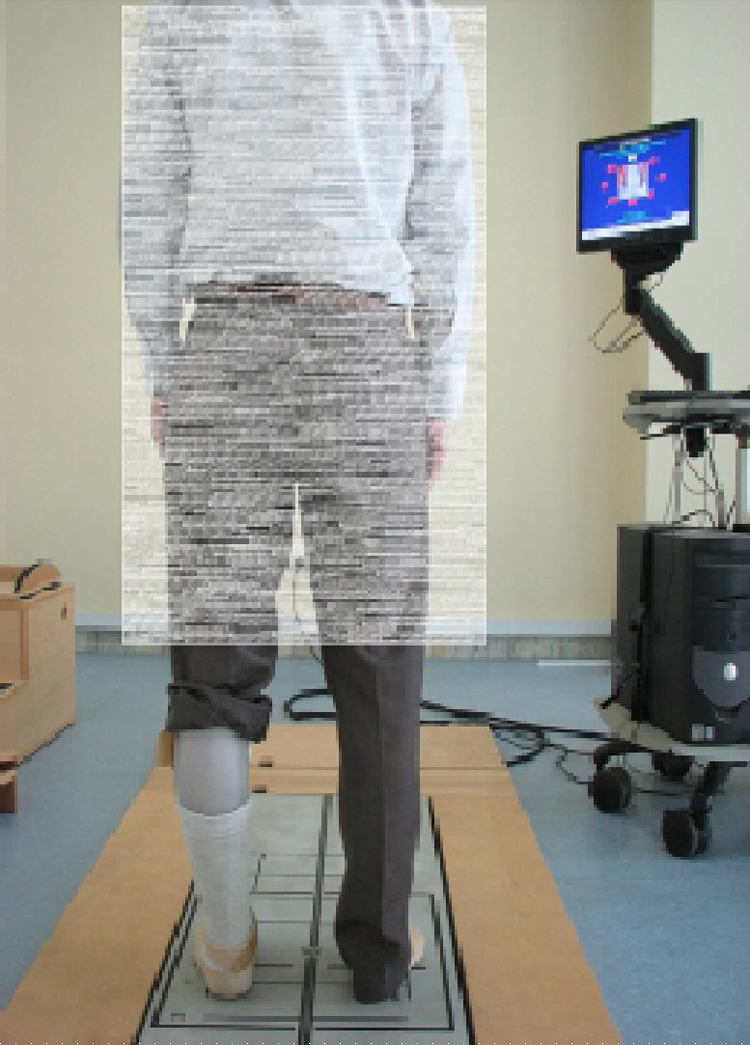
A participant during the LOS test of the Balance Master System.
The STS test of the Balance Master System was the second test of the present study. During this test, the average scores of three trials for weight transfer time (in seconds) and sway velocity of the COG (in degrees per second) were recorded while participants stood up as quickly as possible without upper extremity assistance and held that standing position for approximately 5 s. 7
In addition, Walk across (WA) testing of the Balance Master System was used to record participants’ gait parameters. 32 For each condition, data were collected at 100 Hz, while the participants completed three walking trials at a self-selected walking speed in a straight line across a long force plate (1.5 m × 0.45 m). They started walking 1 m before the plate, finishing 0.5 m after the plate. Gait parameters included gait speed (cm/s), step length (cm), and step width (cm).
Data analysis
The NeuroCom analysis software (version 8.0.3) derived the various kinematics output measures based on the published anthropometric data described in the principles of operation section of the user manual, and the vertical GRFs of participants’ movements, which were recorded by force transducers embedded in the corners of the force plate.
The normality of the data distribution was estimated with the Kolmogorov–Smirnov test. The data were normally distributed and therefore met the assumptions needed for parametric analysis. So paired sample t-tests were used to compare the average gait and balance performance when wearing the modified SAFO without shoe and the conventional SAFO with shoe. The critical p value was defined as 0.05.
Since this study was mainly aimed at comparing modified and conventional SAFOs to determine the efficacy of the modified SAFO at the level of gait and balance performance for indoor barefoot walking, if the comparisons were not significant then the results would imply that the modified SAFO has the same efficacy as the conventional SAFO–footwear combination in correcting participants’ balance and gait performance.
Results
A total of 24 healthy, able-bodied participants (12 males and 12 females) participated in this study. The mean age of the participants was 24.7 ± 4.84 years (range: 19–34 years). In addition, 7 wore SAFOs on the right leg and 17 wore SAFOs on the left leg.
The means and standard deviations of WA test results in Table 1 shows that there were no significant differences in walking speed between the conventional and modified SAFOs. The same findings have been proved regarding step width as well as step length during walking with the two types of SAFOs.
Mean ± standard deviation for gait parameters between wearing the conventional SAFO–shoe combination and the modified SAFO.
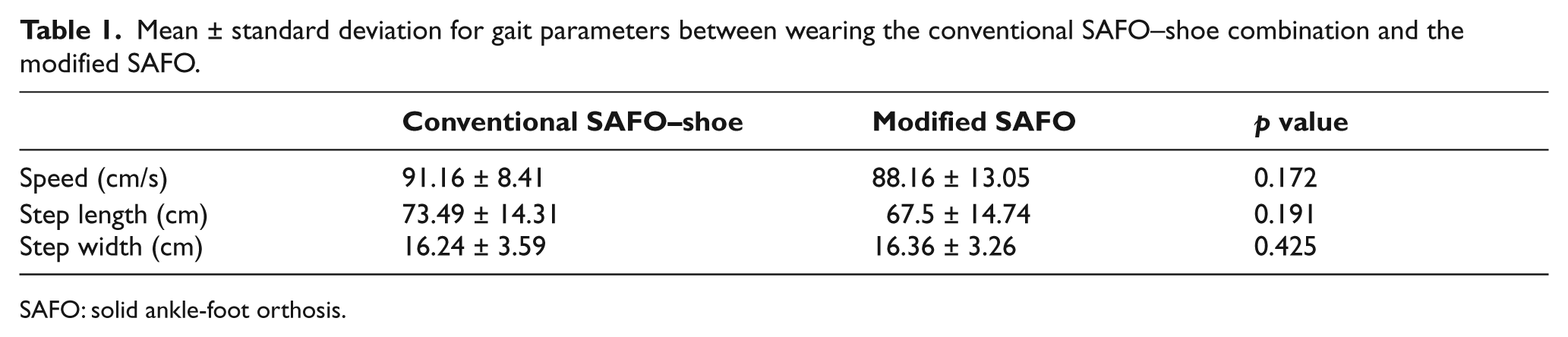
SAFO: solid ankle-foot orthosis.
Table 2 shows the means and standard deviations of balance performance while participants wore the modified SAFO and the conventional SAFO–shoe combination. According to the results of the LOS test, movement velocity and maximum excursion of the COG were not significantly different between the conventional SAFO and the modified SAFO, although the maximal forward excursion of the COG was longer when wearing the modified SAFO in contrast to the conventional SAFO–shoe combination.
Mean ± standard deviation for limit of stability test and sit-to-stand test of dynamic balance between wearing the conventional SAFO–shoe combination and the modified SAFO.
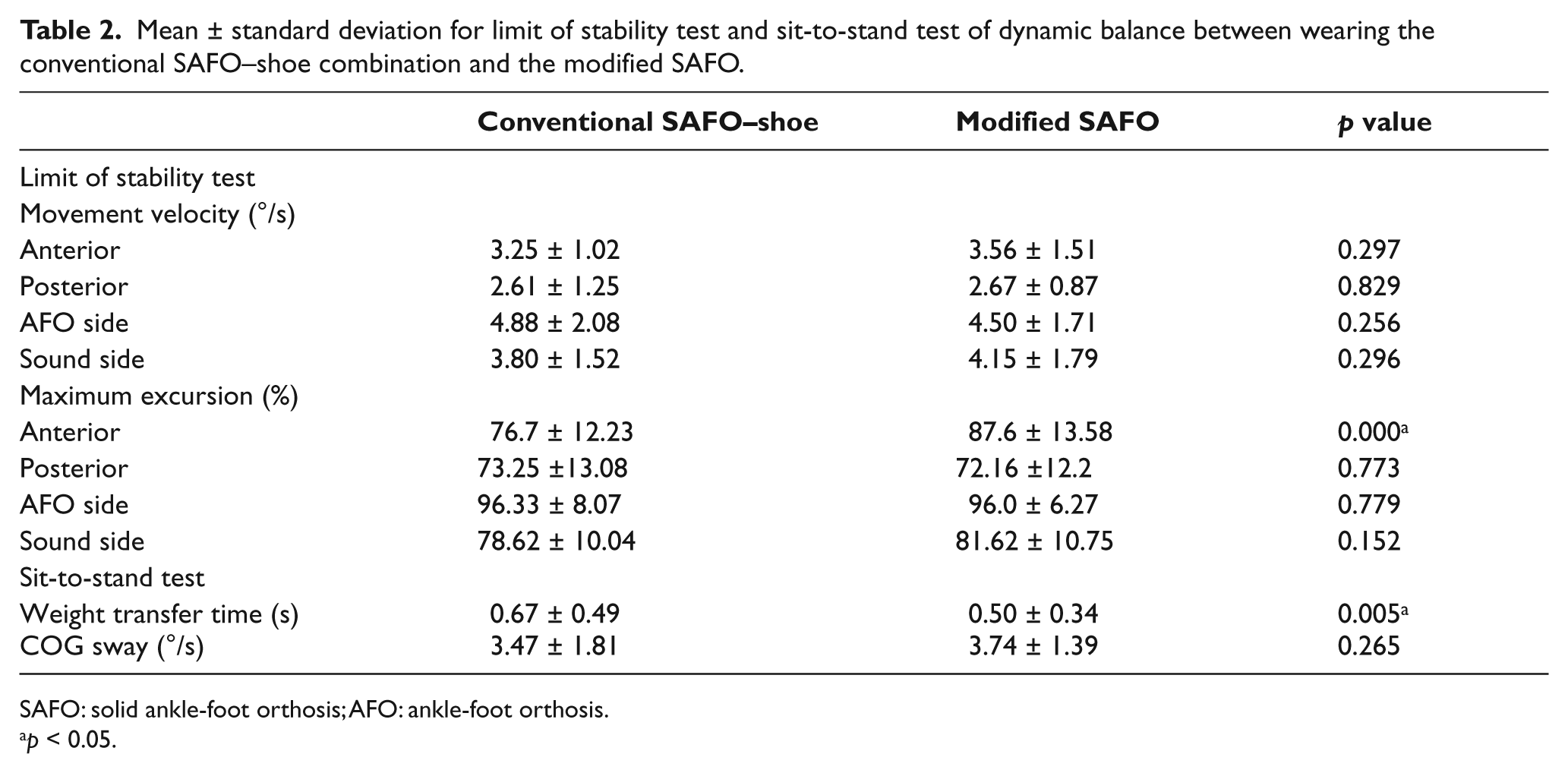
SAFO: solid ankle-foot orthosis; AFO: ankle-foot orthosis.
p < 0.05.
Finally, the weight transfer time reduced while wearing the modified SAFO without a shoe in comparison with the conventional SAFO–shoe combination, although sway velocity of the COG did not change during standing from the chair with the two different kinds of SAFOs.
Discussion
SAFOs are applied in combination with footwear. Rigid AFOs can be prescribed to manipulate the alignment of the GRF by controlling the SVA. 11 This is achieved by modifying the shoe design through, for example, adding wedges and changing the height of the heel. 11 Our previous study of asymptomatic participants showed that with conventional SAFO–footwear combination, the ankle joint was placed in 5°–7° anterior inclination and can improve the level of balance performance. This is in comparison to a conventional SAFO without a shoe where the ankle joint was set in a neutral position. 18 We found that the maximal backward excursion of the COG during the LOS test was increased when participants wore the conventional SAFO–footwear combination in contrast to the conventional SAFO without footwear. In addition, wearing the SAFO combined with a shoe declined sway velocity of the COG during the STS test of the Balance Master System. These findings suggested that the combination of shoes and orthoses influences the ability to maintain postural control. 18 Moreover, the combination of SAFOs with shoes had positive effects on improving some gait parameters such as speed and step length.17,33 As a result, in those cultures that do not use shoes indoors, the SAFO is not able to provide the same biomechanical effects indoors and outdoors.
The main purpose was to investigate the effect of a modified SAFO that could be used with and without a shoe on gait and balance ability of asymptomatic people in comparison with the conventional SAFO–footwear combination. The findings of this study indicated that movement velocity and maximum excursion of the COG were not different between the modified and conventional SAFOs in the LOS test, even though the modified SAFO increased the maximal forward excursion of the COG in contrast to the conventional SAFO. This indicates that, wearing the modified SAFO enhanced the participants’ ability to maintain postural control during activities like reaching forward to open a door or placing something on a shelf. 34 It is possible that wearing a shoe with the conventional SAFO may restrict the movement of the ankle-foot complex shifting the body in various directions. In addition, the SAFO was trimmed proximal to the MTP joints on the medial and lateral sides of the foot, so the flexibility of the footplate may have influenced the ability of weight transfer when wearing the modified SAFO without shoe. There are limited studies that have emphasized the effect of AFOs on balance in different populations. The results of previous studies mainly focused on dynamic balance with respect to lateral weight shifting and weight bearing through the affected side. It has been shown that AFOs improve lateral weight shifting and decrease body sway in hemiparetic patients.6,28 Rao and Aruin 35 concluded that AFOs could contribute significantly to postural control in individuals with peripheral neuropathy. However, Simons et al. 36 found no significant effects of different kinds of AFOs on dynamic balance control. Results of previous studies indicated that their effects on balance were largely dependent on the design characteristics of the orthosis used. Although rigid designs seem to be beneficial in static balance tasks, more flexible designs seem to be superior under dynamic balance conditions. 37
The findings of the current study showed that the modified SAFO could improve balance in the forward direction and perhaps avoid falls in this direction although the postural stability of participants in the backward AFO side and sound side directions were not significantly different between the conventional SAFO–shoe combination and the modified SAFO. In addition, the time taken to stand from a chair reduced when the participants wore the modified SAFO; however, sway velocity of the COG was not notably different when wearing the conventional and modified SAFOs during the STS test. Therefore, overall it was concluded that the modified SAFO almost had the same effect as the conventional SAFO–shoe combination on postural stability in asymptomatic adults.
Positive effects of AFOs have been found for various gait parameters in different studies. Improvements in walking speed and stride length have been documented.5,12,28 In the present study, no significant differences in gait characteristics (including walking speed, step length, and step width) were evident when comparing the modified and conventional SAFOs.
In conclusion, the findings of this study demonstrated the same gait and balance performance for the modified SAFO and the conventional SAFO–footwear combination when both had the same SVA of 5°–7° anterior inclination.
Limitations and need for future research
There are several limitations to this study. First, the participants of this study were healthy people as we preferred to examine our hypothesis regarding new design of the SAFO on asymptomatic people prior to studying the effect of the modified SAFO on patients. Although the results of the present study proved our hypothesis that the modified SAFO had the same effect as the conventional SAFO–footwear combination on gait and balance parameters, our study needs to be replicated in adult participants with neuromuscular disorders like stroke. It is important to clarify the effect of the modified SAFO on patients as different compensatory patterns, muscle strength, and ankle range of movement might exist in participants who have impaired motor control and balance. Additionally, the minimum forward inclination of the tibia was selected for the modified SAFO in order to test the hypothesis, so the optimum inclination of the tibia that the neurological population may tolerate should be considered in the future. Although Owen 16 describes the Angle of the Ankle in the AFO (AA-AFO) and the SVA of the AFO–footwear as independent, in this study, the AA in a SAFO without a shoe was modified to imitate the alignment of the SVA in the conventional SAFO–footwear combination. Further research on the modified SAFO is needed to determine the differentiation between AA-AFO and the SVA since there is poor recognition of these issues in the literature. 38 In addition, it would be beneficial to examine kinetics and kinematics of the modified SAFO in future studies. Finally, the immediate effect of gait and balance has been tested in this study. Further research is required to explore the long-term effect of the modified SAFO on neuromuscular patients.
Conclusion
The results of the present study demonstrated that the modified SAFO had the same effects as the conventional SAFO on gait and balance performance in asymptomatic adults. Although the modified SAFO improved the maximal forward excursion of the COG during the LOS test in comparison to conventional SAFO, our study needs to be replicated in adult participants with neuromuscular disorders before clinical recommendations can be made.
Footnotes
Funding
This study was part of an MSc thesis supported by the Tehran University of Medical Sciences (grant no. P/905).