
Abstract
Background:
Hyperkyphosis may cause balance impairment in elderly people. Although the effectiveness of orthoses for improving balance in hyperkyphotic elderly people has received much attention, the mechanisms by which devices affect balance remain unknown.
Objectives:
The objective of this study was to evaluate changes in balance performance, thoracic kyphosis angle, craniovertebral angle, back muscle endurance and joint position sense after 3 months of wearing a Spinomed orthosis. The study also included a secondary exploratory analysis to determine whether changes in any of the above-mentioned outcome measures can predict balance performance improvement in elderly people with hyperkyphosis.
Study design:
Parallel group randomized controlled trial.
Methods:
In total, 44 hyperkyphotic elderly people were randomly allocated to an experimental group, who wore a Spinomed orthosis and a control group, who did not. No other treatment or change in physical activity was permitted during the study. A blinded assessor evaluated thoracic kyphosis angle, joint position sense, craniovertebral angle, back muscle endurance, Timed Up and Go Test time and Berg Balance Scale score at baseline and after 5, 9 and 13 weeks. All dependent variables were measured without the orthosis and analyzed separately using a 2 × 4 (time × group) mixed model analysis of variance. Based on the results of correlation analysis, thoracic kyphosis angle, back muscle endurance and joint position sense were selected as independent variables in a stepwise multiple regression model.
Results:
The two-way (group × time) interactions were significant in terms of Berg Balance Scale (F = 11.6, P ⩽ 0.001,
Conclusion:
Wearing a Spinomed orthosis for 3 months improved the posture, position sense and muscle performance of hyperkyphotic elderly people. Orthoses may improve balance performance by correcting spinal alignment and increasing proprioceptive information.
Background
Hyperkyphosis, defined as excessive forward curvature of the thoracic spine, is a common age-related postural deviation that may affect up to 40% of elderly people.1,2 Due to the multifactorial etiology of this deformity, it is considered a geriatric syndrome. 3 Low bone mineral density, vertebral compression fracture, degenerative disk disease, routine poor posture and back muscle weakness are risk factors associated with the development and progression of hyperkyphosis.4,5 Hyperkyphosis is a disfiguring condition that affects respiratory capacity, physical function, quality of life and ability to carry out daily activities.4,6
The mortality rates and fall risks among hyperkyphotic elderly people have attracted health practitioners’ attention in recent years. 7 A range of medical modalities, including different types of spinal orthoses, have been developed to manage hyperkyphosis and prevent its adverse consequences. Spinal orthoses such as dorsolumbosacral corset, weighted kypho-orthosis and Spinomed have been designed to create an extension moment to counteract the excessive flexion of a hyperkyphotic spine.8,9 Research has indicated that these spinal orthoses are effective in relieving pain, modifying posture and promoting function.10,11 Most importantly, they may improve balance and reduce the risk of falls, which have been considered as two serious consequences of hyperkyphosis in elderly people.12,13
Although the effectiveness of spinal orthoses on postural balance in elderly people with hyperkyphosis has been evaluated in several studies,13,14 the underlying mechanism for balance performance improvement is still unclear. A suggested mechanism of action of a spinal orthosis is that it improves proprioception through activating skin and muscle mechanoreceptors.13–16 Proprioception is defined as afferent neural information received by various mechanoreceptors including muscle spindles, Golgi tendon organs and joint and cutaneous receptors. 17 Proprioception is a component of motor control and plays a substantial role in balance stability and locomotion.18–20 Furthermore, proprioception is essential for maintenance of optimal spinal alignment and coordination of muscle activation. 21
Correction of skeletal alignment is another possible mechanism suggested in previous studies for balance performance improvement following orthotic intervention.13,22 It has been postulated that an increase in kyphotic curvature and greater forward lean of the trunk lead to a more anterior position of the center of gravity, which may impair balance performance.23,24 It is possible that a spinal orthosis returns the center of gravity into limits of stability through correction of sagittal malalignment. 25 However, the aforementioned mechanistic explanations may just be scientific speculations suggested in the previous literature to justify the effectiveness of spinal orthoses.
In addition, it is likely that correction of spinal alignment improves balance performance indirectly through modification of trunk muscle activity pattern. It has been confirmed that back extensor muscles are the main supporters of the spinal column and maintenance of normal postural alignment during daily activities are dependent on prolonged activation of back extensor muscles; 26 hence kyphotic posture is strongly associated with weakness and deconditioning of these muscles.26,27 In the same vein, an association between poor back muscle performance and balance impairment has been reported in the literature.28–30 Also, muscle deconditioning may cause changes in afferent input from affected muscles 31 and, thereby, lead to further impairment of balance performance. Intact balance control is fundamental for safe mobility-related activities during daily life. 32 Balance disorders may result in undesirable consequences, such as fall-related injuries or activity restriction due to fear of falling. 33 So, it seems very important to address modifiable physical impairments linked to balance, including spinal alignment, back muscle performance and proprioception. 34 Nevertheless, evaluation of the effect of spinal orthoses on proprioception and back muscle endurance has been neglected in the literature. Spinomed is a semi-rigid spinal orthosis that can be used for orthotic management of hyperkyphosis and has been shown to have high compliance rates relative to other spinal orthoses. 35 The efficacy of this orthosis has been evaluated in women with osteoporotic vertebral compression fractures in previous studies,8,22 but its effectiveness for other populations such as elderly patients with asymptomatic hyperkyphosis is still unknown. Accordingly, the present randomized controlled trial primarily aimed to evaluate the effect of a Spinomed orthosis on balance performance, thoracic kyphosis angle (TKA), joint position sense (JPS), back muscle endurance (BME) and craniovertebral angle (CVA). A secondary aim was an exploratory analysis to determine whether changes in the aforementioned parameters predict balance performance improvement in elderly people with hyperkyphosis. We hypothesized that use of a Spinomed orthosis would improve proprioception, enhance muscle performance and correct spinal alignment. Furthermore, we hypothesized that improvement in the aforementioned variables would be associated with improvement in balance and even predict balance performance.
Methods
This study was a prospective, parallel-group randomized, controlled trial with repeated measures design and blinded outcome assessors. Assessments, interventions and data collection were performed at Iran University of Medical Sciences from September 2017 until January 2018. The project was approved by the Ethics Committee of Iran University of Medical Sciences (Committee Number IR.IUMS.REC.1397.429) and was registered in the Iran Registry of Clinical Trials with registration number IRCT2017080335480N1. This study conforms to the Consolidated Standards of Reporting Trials (CONSORT) guideline and reports the required information accordingly.
Participants
Using G-power software 3.0.1 (Franz Faul, University of Kiel, Kiel, Germany) and considering Timed Up and Go (TUG) score as the primary outcome, the sample size was estimated at 32 (16 subjects per group) with α = 0.05, power = 0.8 and effect size = 0.41 (based on mean scores and standard deviations of our pilot study); however, to take account of potential withdrawals, 44 patients (n = 22 per group) were ultimately recruited for the study. Participants were recruited through public announcements and advertisements. People above the age of 60 years with a TKA of more than 50° were included if they could stand and walk without assistance. Exclusion criteria were as follows: a rigid fixed kyphotic deformity; history of fracture, surgery, or trauma in the spine and lower extremities; inflammatory diseases, such as ankylosing spondylitis, rheumatoid arthritis, central nervous system (CNS) disorders, neuromuscular disorders and diabetic neuropathy; untreated hearing or vision disorders; dizziness and vestibular disorders; cardiovascular diseases; severe osteoporosis; joint diseases or deformities of the lower extremities; any spinal deformities other than hyperkyphosis; use of drugs that affect the CNS or balance; and skin problems that made participants unable to wear the orthosis. Participants were withdrawn if they did not adhere to the investigator’s instructions for wearing the Spinomed orthosis or if they were in discomfort or unbearable pain from wearing the orthosis.
Randomization
Participants provided written informed consent and were allocated to experimental or control groups through permuted block randomization in blocks of four at an assignment ratio of 1:1. To ensure allocation concealment, randomization codes were kept in opaque, sealed, sequentially numbered envelopes. The obvious nature of orthoses obstructed the blinding of participants to their group, but the outcome assessor was blinded to group allocation, as participants removed their orthosis before entering the examination room.
Intervention
The experimental group wore a Spinomed® IV AP orthosis (Medi-Bayreuth, Bayreuth, Germany). The Spinomed is a semi-rigid thoracolumbar support consisting of a hand-moldable metallic back pad and a system of belts with Velcro. The posteriorly directed forces provided by shoulder straps and the total contact of the back pad can help kyphotic posture correction. Donning and doffing is easy and has an acceptable weight of about 450 gr. A single certified orthotist fit the orthoses based on the manufacturer’s instructions and in accordance with individuals’ anatomy and also taught participants how to don and doff their orthoses. Participants were asked to wear their orthoses for 13 weeks. For the first 2 weeks, orthoses were worn for 30 min a day to prevent muscle cramps. After that, they were worn for 2 h a day for the next 5 weeks, with application duration varying from 2 to 4 h a day on the basis of individuals’ physical activities until the 13th week. During the intervention period, the amount of correction force applied by the orthosis was adjusted monthly by an experienced orthotist who tightened the shoulder straps and reformed the back metal pad to fit the thoracic spine curvature. To control participants’ adherence to the intervention, subjects were asked to record their hours of donning and doffing the Spinomed orthosis in a daily log. The control group was advised to maintain their daily physical activity and did not receive any external support or exercise therapy.
Outcomes
In this study, balance performance was considered the primary outcome and TKA, CVA, BME and JPS were reported as secondary outcomes. Position sense was assessed first to prevent the effect of fatigue on the results of this test. However, other assessments were administered in random order. Assessments were performed at baseline and weeks 5, 9 and 13. The same experienced physical therapist, who was blinded to group allocation, administered the outcomes measures to all participants and all dependent variables were measured without the orthosis. Weight was measured in kilograms using a calibrated scale and participants’ height was measured using a standard measuring tape.
In this study, balance performance was rated using the Berg Balance Scale (BBS) and TUG Test. These balance measures have been extensively used in research and clinical practice. BBS simulates a number of tasks a person uses during daily activities and can predict the onset of difficulty with activities of daily living in community-dwelling older adults. 36 This test takes 10–15 min to administer and scores less than 45 indicate an increased risk of falls in community-dwelling older adults. 37 Excellent inter-rater (Intra-class Correlation Coefficient (ICC) = 0.98) and intra-rater reliability (ICC = 0.98) have been reported for BBS in an elderly population. 38 The TUG Test is the shortest and most reliable clinical balance test that predicts the risk of falls in elderly people. 39 A cut-off score of 13.5 s is predictive of falls in community-dwelling elderly people. 40 Previous studies have reported excellent inter-rater (ICC = 0.99) and intra-rater (ICC = 0.99) reliability for the TUG test in community-dwelling older adults.40,41
Balance was measured using the BBS and TUG Test. The BBS includes 14 tasks scored on a scale of 0 (unable to perform) to 4 (normal performance), with a maximum score of 56.37,38 The TUG Test measures the time it takes participants, in seconds, to rise from a 41-cm high armchair, walk 3 m, turn and return to a full-seated position in the chair.39,49
The degree of kyphosis was measured using a dual digital inclinometer (JTech Medical, Salt Lake City, UT, USA) with a reported reliability of 0.92–0.97. 42 The participant wore an open back gown and the spinous processes of the 1st and 12th thoracic vertebrae (T1 and T12) were marked on the skin by the examiner. Next, the participant was asked to stand in a relaxed natural posture. As the dual digital inclinometer uses a gravity-realized reference point for calibration of this tool, both sensors within the inclinometer were set at zero on a vertical wall before assessment. Then, the primary sensor and the secondary sensor were located on the T1 and T12 spinous processes, respectively and the thoracic kyphosis angle was recorded.
CVA was measured to evaluate forward head posture and refers to the intersection between a horizontal line and a line that connects the ear targus and the seventh cervical (C7) spinous process. CVA assessment, in this study, was based on a photogrammetry technique described by Salahzadeh et al. 43 A Nikon D3300 24 megapixel camera with a maximum resolution of 6016 × 4000 pixels was used for taking digital lateral view photographs and the CVA calculated using Digimizer image analysis software 5.3.4 (MedCalc Software bvba, Ostend, Belgium).
The JPS test measured participants’ ability to reproduce a predetermined target position. First, the participants were asked to sit down and stand up twice. Then, they were asked to sit for the third time and stay in that position, which was considered the natural sitting posture. 44 The hips and knees were at 90° angles, the hands were crossed over the chest and the distance between the legs was 20 cm. 44 Two inclinometer sensors were placed on the seventh cervical (C7) vertebra and 12th thoracic (T12) vertebra. All tests were performed while the participant was in a normal sitting position with his or her eyes closed. The chair used for this test had a 25 cm back to isolate or minimize posterior pelvic tilt and lumbar flexion movements while the participant was sitting.45,46 Each participant was asked to extend his or her thoracic spine, to stop moving upon hearing the “STOP” command given by the examiner, to stay in the same position for 3 s and then to return to the initial position. After that, the participant was asked to reproduce the previous position without the examiner’s guidance, stay there for 3 s and then return to the initial position. The angle each participant was asked to reproduce was half the extension range that the individual could reach using his or her maximum effort in a neutral state.
The JPS test was repeated 6 times. Then, maximum and minimum values were deleted and the remaining four values averaged to obtain the repositioning error. The repositioning error was calculated as the difference between the target and the patient’s reproduced positions. There are three quantitative definitions for position sense: the absolute error (AE), which is the difference in positions without respect to direction; the constant error (CE), which is the difference in positions with respect to direction; and the variable error (VE), which is the standard deviation of the constant error. The following equations were used

where n is the frequency of testing and REi is the raw magnitude of the repositioning error. 47
BME was measured using the Ito test, which has excellent reliability in office workers with low back pain. 48 However, the reliability of this test in community-dwelling older adults has not been reported. Each subject was placed in the prone position on a bed with a pillow under their belly with their hands positioned alongside the body. Upon hearing the “START” command, the subject raised their upper trunk. Each subject was asked to keep their neck down and flexed as much as possible during testing and to contract the gluteus maximus muscles to maintain pelvic stability. This test continued until the participant was unable to breathe naturally and/or maintain the position but did not exceed 5 min.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences (Version 16; SPSS Inc., Chicago, IL, USA). Statistical significance was set at P = 0.05 for all statistical tests. All data were encoded to prevent bias and to blind the statistician. The Kolmogorov–Smirnov test was used to determine the normality of the distribution and showed that BME, TKA and TUG Test had a skewed distribution. These were log transformed to stabilize variance. A series of independent t tests were used for baseline intergroup comparisons. To avoid overestimating treatment efficacy on the basis of attrition, all participants were analyzed based on the intention-to-treat principle. The last measures of any dropouts were carried forward in the analysis.
BBS scores, TUG Test times, TKA, CVA, BME and JPS were analyzed using separate 2 (group: experimental vs. control group) × 4 (time: baseline, week 5, week 9 and week 13) mixed-model analyses of variance (ANOVAs). Where the group’s interaction with time was significant, a one-way repeated measures ANOVA was used to determine the simple main effect. Bonferroni corrections were used for multiple comparisons.
Pearson product moment correlation coefficient was used to determine the strength of bivariate correlation of changes in BME, TKA, JPS and CVA, with changes in BBS score and TUG Test time. Among these variables, TKA, BME and JPS that exhibited a significant correlation with the TUG Test time and or BBS score were included in a multiple stepwise regression model as candidate predictor variables for TUG Test time and BBS score.
Results
Between September 2017 and January 2018, 317 individuals (198 females and 119 males) were screened. Of these, 273 were excluded because they had one or more of the following conditions: diabetic neuropathy, cardiovascular diseases, lower extremity deformities, dizziness and use of drugs that affect the CNS or balance, or they were unwilling to participate. Ultimately, 44 were eligible and willing to participate in the study. During the study, four participants withdrew from the experimental group (four females) and four participants withdrew from the control group (three males and one female) due to bed rest in hospital (n = 2), inability to wear the orthosis as required (n = 2), trauma in the lower extremities (n = 1), unwillingness to participate in follow-up assessment (n = 2) and death (n = 1), as shown in Figure 1. Comparison of demographic and clinical characteristics between the two groups showed no significant difference at baseline (Table 1).
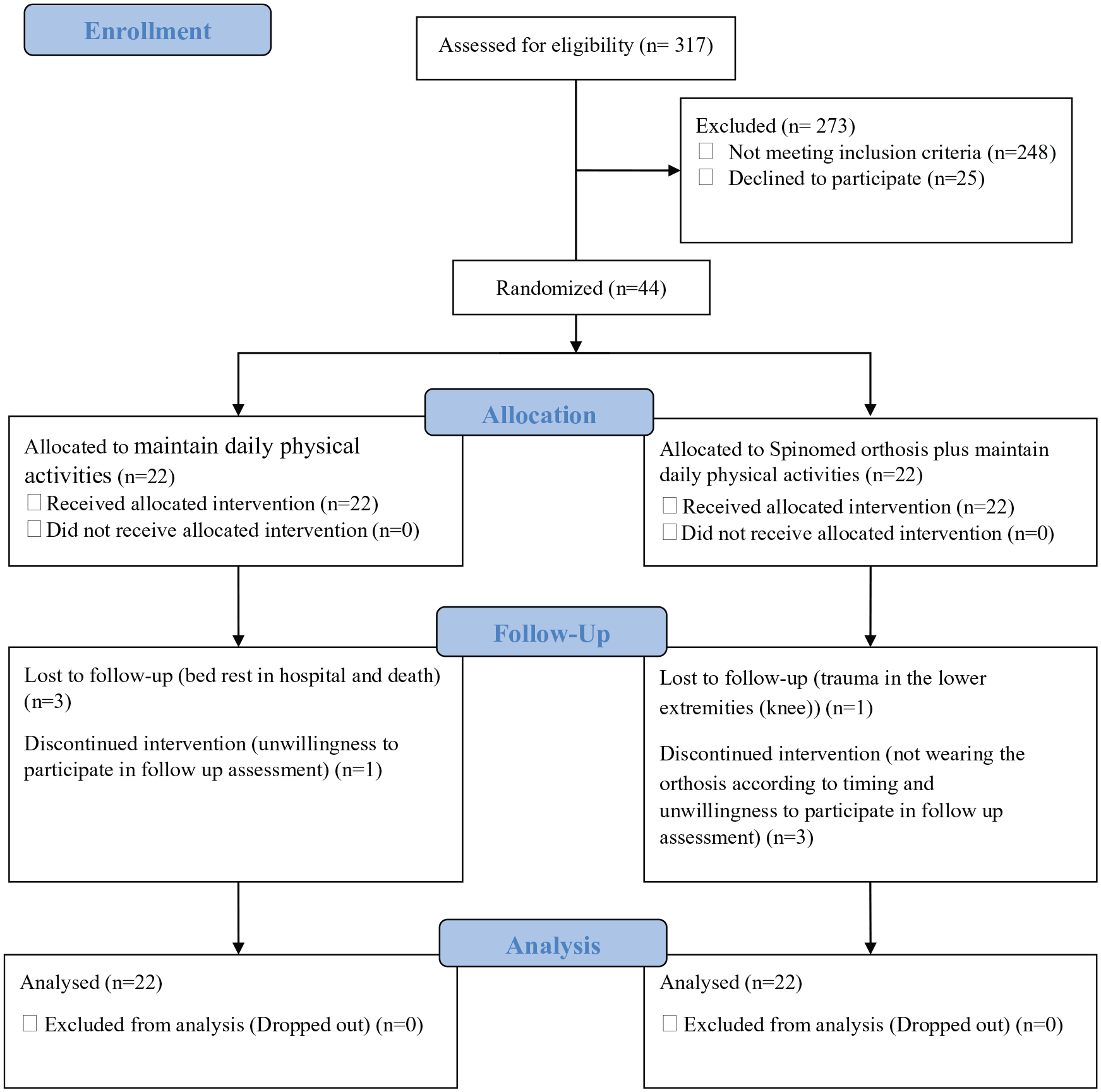
Consolidated Standard of Reporting Trials (CONSORT) flow chart.
Baseline characteristics and outcome measures before and after (i.e. 13 weeks) intervention in both groups.
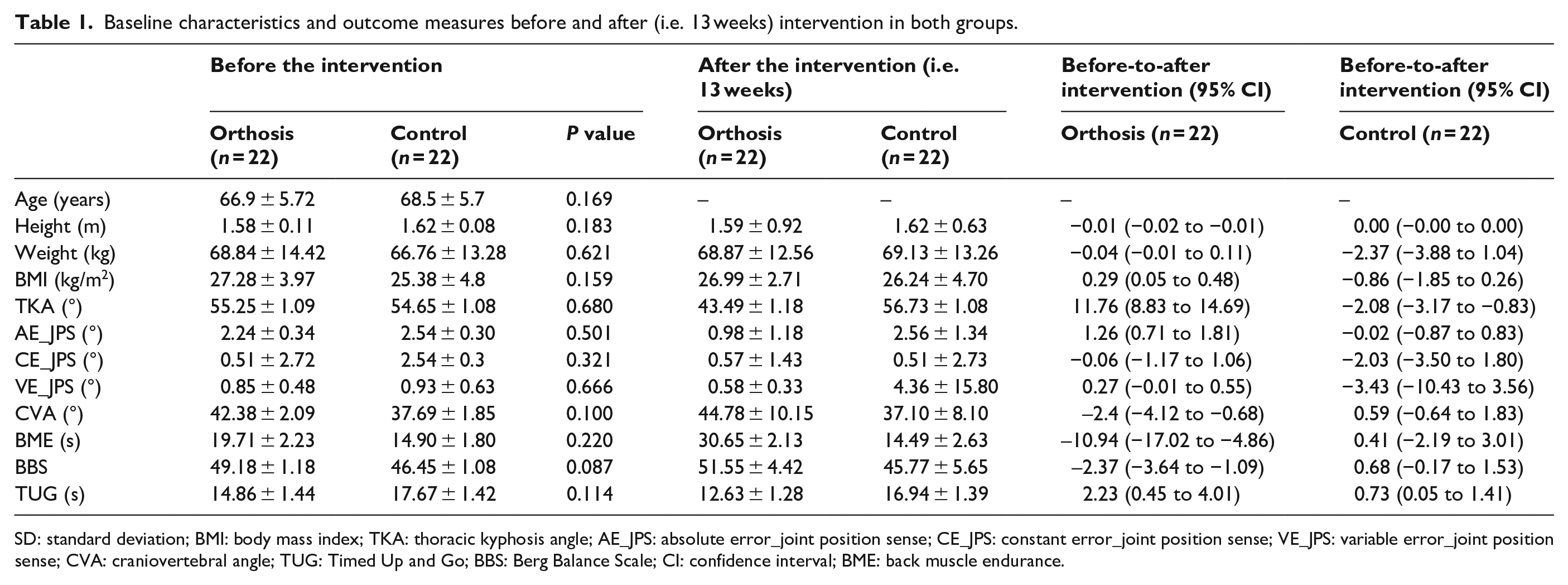
SD: standard deviation; BMI: body mass index; TKA: thoracic kyphosis angle; AE_JPS: absolute error_joint position sense; CE_JPS: constant error_joint position sense; VE_JPS: variable error_joint position sense; CVA: craniovertebral angle; TUG: Timed Up and Go; BBS: Berg Balance Scale; CI: confidence interval; BME: back muscle endurance.
The two-way (group × time) interactions were significant in terms of BBS (F = 11.6, P ⩽ 0.001,
Summary of the analysis of variance for clinical variables.
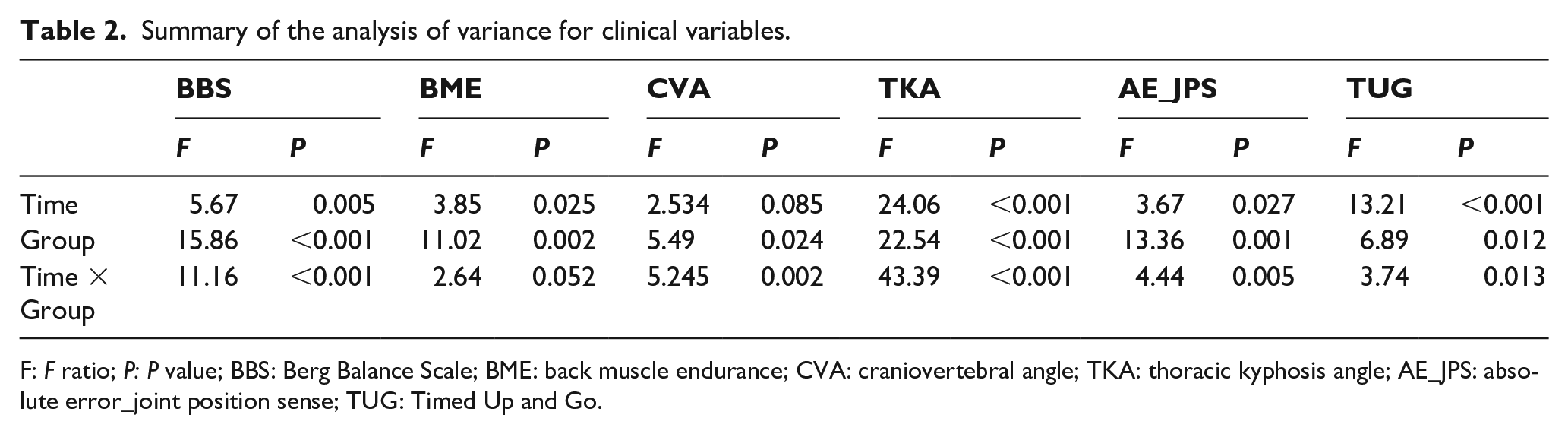
F: F ratio; P: P value; BBS: Berg Balance Scale; BME: back muscle endurance; CVA: craniovertebral angle; TKA: thoracic kyphosis angle; AE_JPS: absolute error_joint position sense; TUG: Timed Up and Go.
BME was the only variable that significantly correlated with BBS score (r = 0.463, P = 0.035). Hence, BME was included as an independent variable in a regression model for BBS score. However, no significant association was found between BME and BBS score (R2 = 0.074, P = 0.0234; Table 3). Regarding TUG Test time, significant correlations with TKA (r = −0.432, P = 0.029), BME (r = −0.521, P = 0.015) and absolute value of repositioning error (r = 0.457, P = 0.037) were observed. Based on these findings, BME, absolute value of repositioning error and TKA were used as independent variables in a stepwise multiple regression model for the TUG Test time. TKA and absolute value of repositioning error were found to be significantly associated with TUG Test time (R2 = 0.155, P = 0.037; R2 = 0.292, P = 0.012, respectively; Table 3).
Multiple regression analysis of the association between BBS and BME and between TUG test and AE_JPS, TKA and BME.
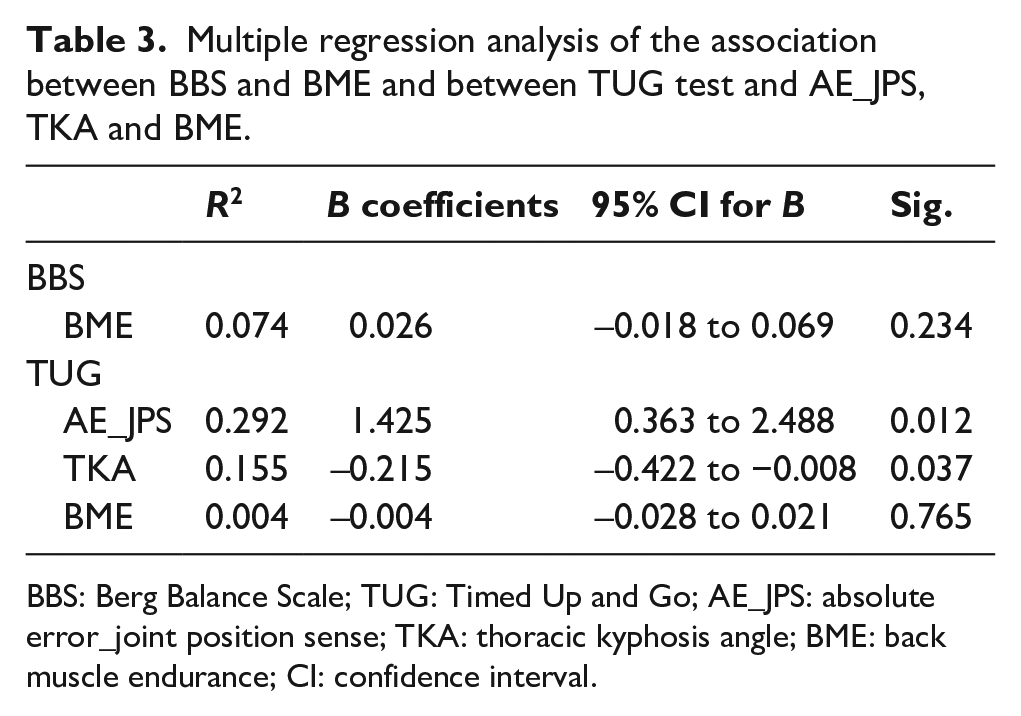
BBS: Berg Balance Scale; TUG: Timed Up and Go; AE_JPS: absolute error_joint position sense; TKA: thoracic kyphosis angle; BME: back muscle endurance; CI: confidence interval.
Discussion
The present randomized controlled trial primarily aimed to evaluate the effect of a Spinomed orthosis on balance performance and modifiable physical impairments linked to balance including TKA, CVA, JPS and BME. Furthermore, we aimed to determine whether changes in the aforementioned parameters predict balance performance improvement in elderly people with hyperkyphosis. The results of this study showed that wearing a Spinomed orthosis for 3 months improved the posture, position sense and muscle performance of hyperkyphotic elderly people. Spinal orthoses may improve balance performance by correcting spinal alignment and increasing proprioceptive information.
Spinal alignment
The significant reduction in TKA as a result of orthotic treatment supported previous findings.8,22 However, kyphosis angle correction in this study was 1.94 times higher than that reported by Pfeifer et al. 22 for the same orthosis. This may be due to the periodic adjustment of orthoses in this study by an experienced orthotist, which may have maintained corrective force at an ideal level. Spinomed orthoses are semi-rigid and may correct spinal alignment by applying three-point pressure, creating a trunk extension moment. This orthosis, like other spinal orthoses, may also provide a psychological reminder to maintain an upright posture by providing feedback on body position. 8
Previous literature has reported that forward head posture is associated with greater thoracic kyphosis.50,51 This study was the first to measure TKA and CVA to determine the effectiveness of a Spinomed orthosis in correcting spinal alignment. Although the applied orthosis lacked a cervical component, it corrected forward head posture (FHP). FHP is one of the most common postural abnormalities, appearing as increased lordosis in the upper cervical spine and decreased lordosis in the lower cervical spine. 52 Since, the association of FHP with thoracic hyperkyphosis has been reported in previous studies,50,53 correction of thoracic curvature possibly contributes to the restoration of normal cervical alignment. In the experimental group, the highest change in CVA occurred at the end of the first month.
The mean reduction in TKA of the experimental group was 11°. A minimal detectable change (MDC) of 8° in TKA has been reported in a previous study. 54 Therefore, it seems that changes in TKA in the current study may be considered a true change. On the contrary, changes in CVA did not reach the previously reported MDC of 4°, 53 so, changes in CVA do not exceed the measurement error.
Back extensor muscle endurance
BME increased in the experimental group. The average increase in the holding time of the test position in the experimental group was 11 s, which is higher than the standard error of measurement (SEM) reported in a previous study (7 s). 55 Although it seems that BME enhancement is above the potential errors accompanied by measurement, changes in BME did not reach the estimated MDC of 19.4 seconds. So, changes in BME are not clinically valuable. It must be noted that the reliability of the Ito test has been evaluated only for office workers with back pain and no SEM and MDC value for this test has yet been reported for community-dwelling older people. So, the clinical relevance of these findings must be interpreted cautiously.
Maintaining the erect posture of the spine depends on the function of back extensor muscles, which are the main supporters of the spine. 27 A kyphotic posture may cause stretch weakness of extensor muscles through changes in the length–tension relationship. 56 Some researchers have reported decreased back muscle activity in kyphotic posture, which may decondition the extensor muscles and cause muscle performance impairments. 27 Orthotic treatment may correct spinal alignment by facilitating back muscle activity and increasing the ability of these muscles to sustain isometric contraction. Previous studies have not investigated the effectiveness of a Spinomed orthosis in terms of BME but have reported increased muscle strength (maximal voluntary contraction force) after wearing a Spinomed orthosis for 6 months.8,22 However, participants in these studies suffered from painful vertebral fractures and the muscle strength test may have been affected by confounding factors, such as pain. Pain and even pain catastrophizing are considered important confounding factors in the assessment of muscle performance. 57 Therefore, patients with acute vertebral fractures may avoid their maximum effort in muscle strength test because of pain anticipation in pre-treatment assessments. But, after a course of orthopedic treatment and pain relief, the test might be done at an optimal level. Considering the exclusion of participants with back pain in present study, our findings cannot be affected by pain. Results of the present and previous studies do not support the widely held belief that muscle deconditioning occurs as a result of using spinal orthoses. 58 However, muscle weakness due to orthosis wear may occur when the orthosis is rigid and completely limits spinal movements. 58 Additionally, full-time wear of a Spinomed orthosis may obstruct muscle activity.
JPS
Improved proprioception is considered a mechanism of spinal orthoses, but the validity of this hypothesis has not been tested. Results of this study indicated reduced repositioning error in the second and third months of intervention in the experimental group (refer to Supplementary Material). This improvement in proprioception cannot be attributed to increased tactile sensation, because cutaneous receptors are fast adaptive. 17 If improved position sense was achieved by increasing cutaneous input, results opposite to those found would be expected and the highest changes in position sense would have occured during the first month of intervention. However, changes were insignificant in the first month (refer to Supplementary Material). Proprioception improvement in this study may be attributed to muscle spindles, because these mechanoreceptors are very sensitive to muscle length changes.27,59 It is possible that the orthosis positions muscles in a more optimal length through correcting spinal alignment, improving the ability of muscle spindles to provide sensory information. Regarding JPS, this measure lacked published standard error of measurement or MDC to help determine the clinical relevance. Hence, interpretation of clinical relevance of these findings must be done with caution.
Balance performance and spinal alignment, muscle endurance and position sense
A reduction of 2.23 s was found in TUG test times in the experimental group, which is larger than the smallest real difference of 1.1 s reported in a previous study. 60 Accordingly, changes in TUG test time in the experimental group may be considered a true change. Although a two point increase in BBS score in the experimental group was statistically significant, its clinical relevance is questionable given the average baseline score of participants in this study was above 45 points and a 4-point change in score is required to consider it a true change. 61
Improvement in balance performance in the experimental group was consistent with the results of previous studies.13,62 Orthoses may affect postural balance by correcting spinal alignment and improving muscle performance and proprioception; however, these hypotheses have not been tested previously. This study investigated each factor thought to be influential in improving balance performance. A significant but low to moderate association was found between changes in TKA, BME and JPS with changes in TUG test times. However, the coefficient of determination in the stepwise multiple regression model for all variables was 0.44, indicating that 44% of variability in TUG test times was explained by TKA and JPS. These results show that 56% of the variation in TUG test times cannot be explained by TKA or JPS. Therefore, there must be other factors contributing to TUG test performance. A significant but low correlation was found between BME and BBS score, which was consistent with the result of Suri et al. 28 In our regression model, a change in BME was not a significant contributor for BBS score. It seems that balance performance is multifactorial and it is likely that factors other than TKA, JPS and BME play roles in postural balance. Balance confidence and fear of falling are examples of contributing factors that should be investigated further.33,63
Limitations
It is possible that the participants have not followed the wearing schedule which was instructed by the orthotist despite the fact that their compliance was monitored using a self-reported diary. Like other rehabilitation interventions, the participants were not blinded to group allocation. However, to reduce contribution of participants’ expectations and placebo effects to outcomes, all variables were evaluated without orthoses. Nevertheless, we cannot be sure that participants’ beliefs about orthopedic treatment did not influence the more upright posture they adopted in the experimental group. Participants in the current study were elderly people with asymptomatic hyperkyphosis; those suffering from thoracic or low back pain were excluded. So, caution should be taken in generalizing the results of this study to elderly people with painful osteoporotic vertebral fracture. Pain and even pain catastrophizing are considered important confounding factors in the assessment of muscle performance because of pain anticipation wherein the patient is likely to abstain from maximum effort during muscle endurance testing so as not to aggravate pain. 57 Furthermore, pain can influence proprioception adversely 64 and some researchers have attributed postural balance disorder to pain interference. 65 Since in previous studies pain was not controlled as a confounding factor, one cannot know whether the improvement in muscle performance and balance ability reported in the previous studies was influenced by pain.
Spinal flexibility is considered one of the potential contributing factors in success of orthotic treatment. 35 None of the participants in this study had fixed deformity and all were able to reduce their kyphosis angle during attempted hyperextension of the trunk and place their back in a more upright position. It is likely that patients with fixed spinal curves would have different results.
Using a secondary analysis to explore the potential determinants of balance performance improvement following a period of orthotic treatment is the main weakness of this study. Further studies are required to evaluate the association of longitudinal changes in various physical impairments with balance performance improvement in larger patient populations. As our sample size was not large enough to provide a robust regression model, potential confounders like age and sex were not included in the regression model.
Furthermore, we conducted an internal pilot study for sample size calculation but the data collected from the pilot study were also included in the final efficacy analysis, which should be considered another limitation of the current study.
The mean TKA in this study was 55.16, so generalizing the results of this study to a population with more severe deformities must be done carefully, although the effectiveness of Spinomed orthosis for people with more severe kyphotic posture has been reported by Pfeifer et al.8,22
Conclusion
Findings of this study indicated that orthotic treatment of hyperkyphosis in elderly people could decrease TKA and improve JPS. Also, our findings did not support the common assumption about the adverse effects of wearing spinal orthosis for trunk muscle performance. Proprioceptive information may be increased and balance performance improved by correcting spinal alignment in this population.
Supplemental Material
10.1177_0309364620923816_Supplementary_material – Supplemental material for Effect of a Spinomed orthosis on balance performance, spinal alignment, joint position sense and back muscle endurance in elderly people with hyperkyphotic posture: A randomized controlled trial
Supplemental material, 10.1177_0309364620923816_Supplementary_material for Effect of a Spinomed orthosis on balance performance, spinal alignment, joint position sense and back muscle endurance in elderly people with hyperkyphotic posture: A randomized controlled trial by Mostafa Hosseinabadi, Mojtaba Kamyab, Fatemeh Azadinia and Javad Sarrafzadeh in Prosthetics and Orthotics International
Footnotes
Acknowledgements
Medi Inc. donated Spinomed orthoses to this study. The funder had no role in the interpretation and reporting of results or the decision to approve or submit the manuscript for publication.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by Iran University of Medical Sciences with grant number: 970203233170.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.