
Abstract
Background: The osseointegration programme for upper extremity amputation started in Sweden in 1990, when a titanium fixture was first implanted into a thumb. This method has since been used for transhumeral and below-elbow amputation. The treatment involves two surgical procedures. During the first a titanium fixture is surgically attached to the skeleton, and a second procedure six months later involves a skin penetrating abutment to which the prosthesis is attached.
Objectives: To describe the osseointegration procedure for surgery, prosthetics and rehabilitation.
Methods: Patients with short stumps and previous problems with prosthetic fitting were selected. From 1990 to April 2010, 37 upper limb cases were treated and fitted with prosthesis: 10 thumbs, 1 partial hand, 10 transradial and 16 transhumeral amputations. Of these, 7 patients are currently not prosthetic users.
Results: Patients indicated that function and quality of life had improved since osseointegration.
Conclusion: Osseointegration is an important platform for present and future prosthetic technology. The prosthetic situation is improved due to the stable fixation, freedom of motion and functionality.
Keywords
Introduction
Amputees using upper extremity prostheses experience problems with conventional prostheses. Sockets often restrict range of motion and the prostheses do not always fulfil demands relating to stability, comfort and functionality. 1 – 7 Problems with excessive sweating and irritation from the harness or socket have been reported. 2,6,8 – 12 Other areas in need of improvement include range of movement of the hand/arm, 7 socket suspension, and the ability to rely on the prosthesis being properly secured. This is especially evident after amputation at the transhumeral (TH) level, where a harness is most frequently needed, or at the thumb level, where part of the hand has to be covered to provide prosthetic suspension. Traditional prosthetic socket and suspension technology often fails to meet both cosmetic and functional requirements, which can severely impair quality of life. With direct bone anchorage, the prosthesis is attached to the residual limb without use of a socket. The method is based on the principle of osseointegration, which has been in clinical use for tooth and maxillofacial replacements since 1965. 13 – 15
Starting the osseointegration programme for extremity amputees in Sweden was a major challenge. The first patient, a female with a bilateral transfemoral amputation, was treated in 1990, followed by a thumb amputee and a series of transradial level amputees. A direct attachment for the prosthesis is created by surgically implanting a threaded titanium implant (fixture) into the bone, and an additional titanium implant (abutment) connected to the fixture and penetrating the skin (Figure 1a). The concept of osseointegration entails direct contact between the fixture and the bone tissue, thereby ensuring a stable attachment.
15
From a prosthetic and rehabilitation angle, no methods and components were available. The goal was to design methods and components to enable various amputation levels and residual limb variants to be fitted with prostheses of different types without the need for a socket. Absence of a socket is the main difference between conventional socket prostheses and bone-anchored prostheses. The bone-anchored prosthesis always fits, is correctly attached and is held firmly in place by the titanium implant and prosthetic attachment device. This eliminates all socket-related problems such as heat, sweating, chafing or discomfort. Osseointegration of the upper extremity is used for amputation at the thumb, transradial (TR) and TH level, and a large number of transfemoral patients have been treated.
12,16
–
20
(a) Skin penetrating abutment. (b) The puck. (c) Attachment, alignment and rotation safety device.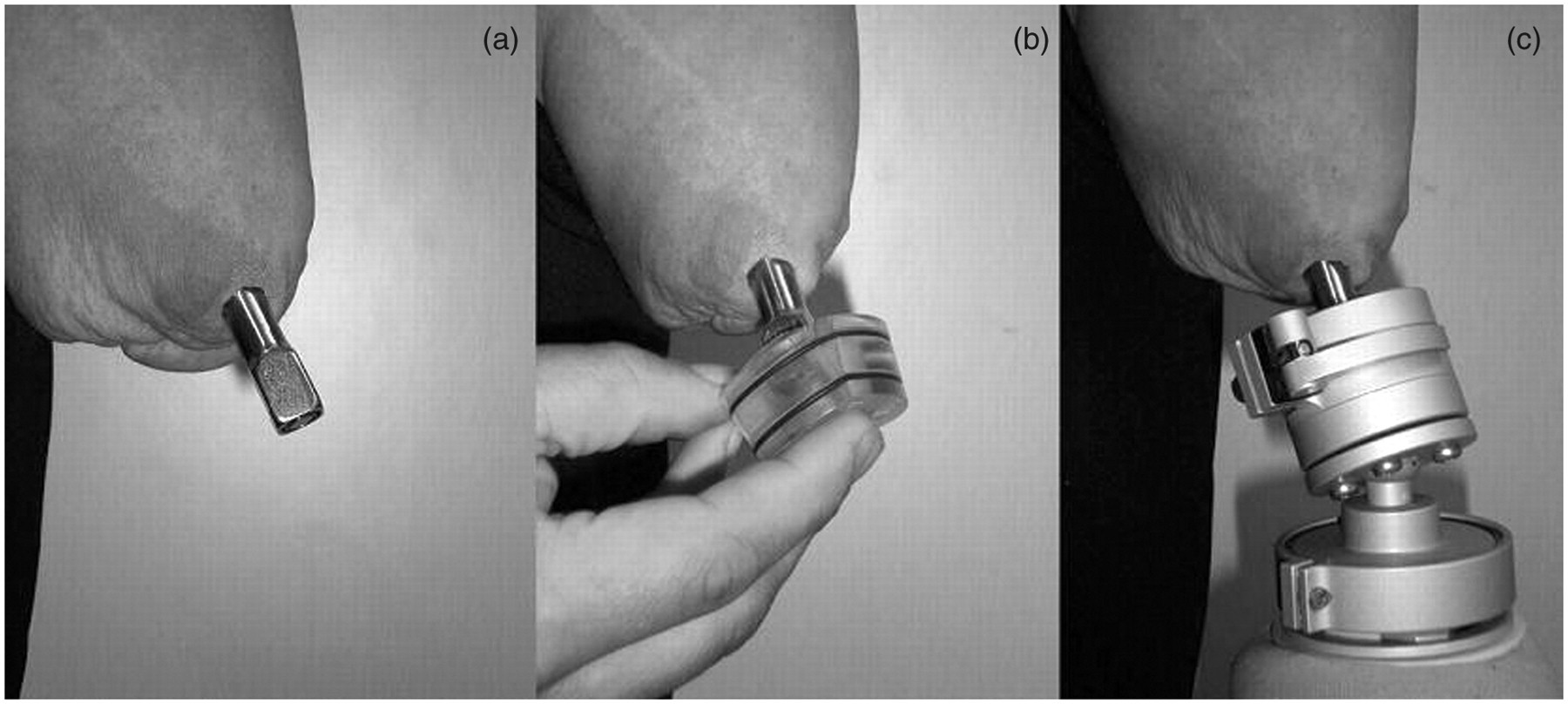
Methods
Assessment and requirements for treatment
Patients referred to the Centre of Orthopaedic Osseointegration (COO) are assessed by a team consisting of orthopaedic surgeons, a prosthetist, an occupational therapist (OT) and a co-ordinator. Prior to the team assessment, patients meet the prosthetist and the OT to be given detailed information about the treatment plan. They are offered the opportunity to meet a patient with the same level of amputation fitted with a bone-anchored prosthesis, and can ask any questions they choose.
The criteria for bone-anchored upper limb prostheses are:
Difficult to fit with a conventional prosthesis, or previous experience of a socket prosthesis with high documented wear and socket- or harness-related problems Adequate bone quality assessed by X-ray No contra-indicated illnesses or disabilities, such as ongoing chemotherapy or corticosteroid treatment Highly motivated patient who can conform to the treatment plan.
All other options/prosthetic solutions must be considered before the decision for treatment is made.
The team analyses the information and the assessment results. The patient has to reconsider the team assessment which can result in several alternatives: osseointegration, recommendation to change the existing socket prosthesis or no further steps at this time. If the patient is regarded as a candidate for osseointegration, the planning and co-ordination process begins.
This study of osseointegration prostheses of the upper limbs has been approved by the Swedish Regional Ethics Committee in Gothenburg, no. 626-10.
Implant system and surgery
The implant system incorporates three main components (Figure 2): a threaded titanium implant (the fixture), a skin-penetrating cylindrical implant (the abutment), and a titanium screw (the abutment screw) which holds the system together. The surgical procedure consists of two operations/stages (S1 and S2). At S1, the skeleton is surgically exposed. The fixture is inserted intramedullary using fluoroscopy and the wound is then closed. The healing period is normally six months, based on clinical experience from dental osseointegration science.
13
The implant is kept unloaded until the bone has grown into the threads. The patient is informed to avoid high external forces to the distal end of the stump. At S2 surgery, the implanted fixture is re-exposed and the abutment is connected to the fixture. The wound is closed with the abutment penetrating the skin.
15,16,21
–
23
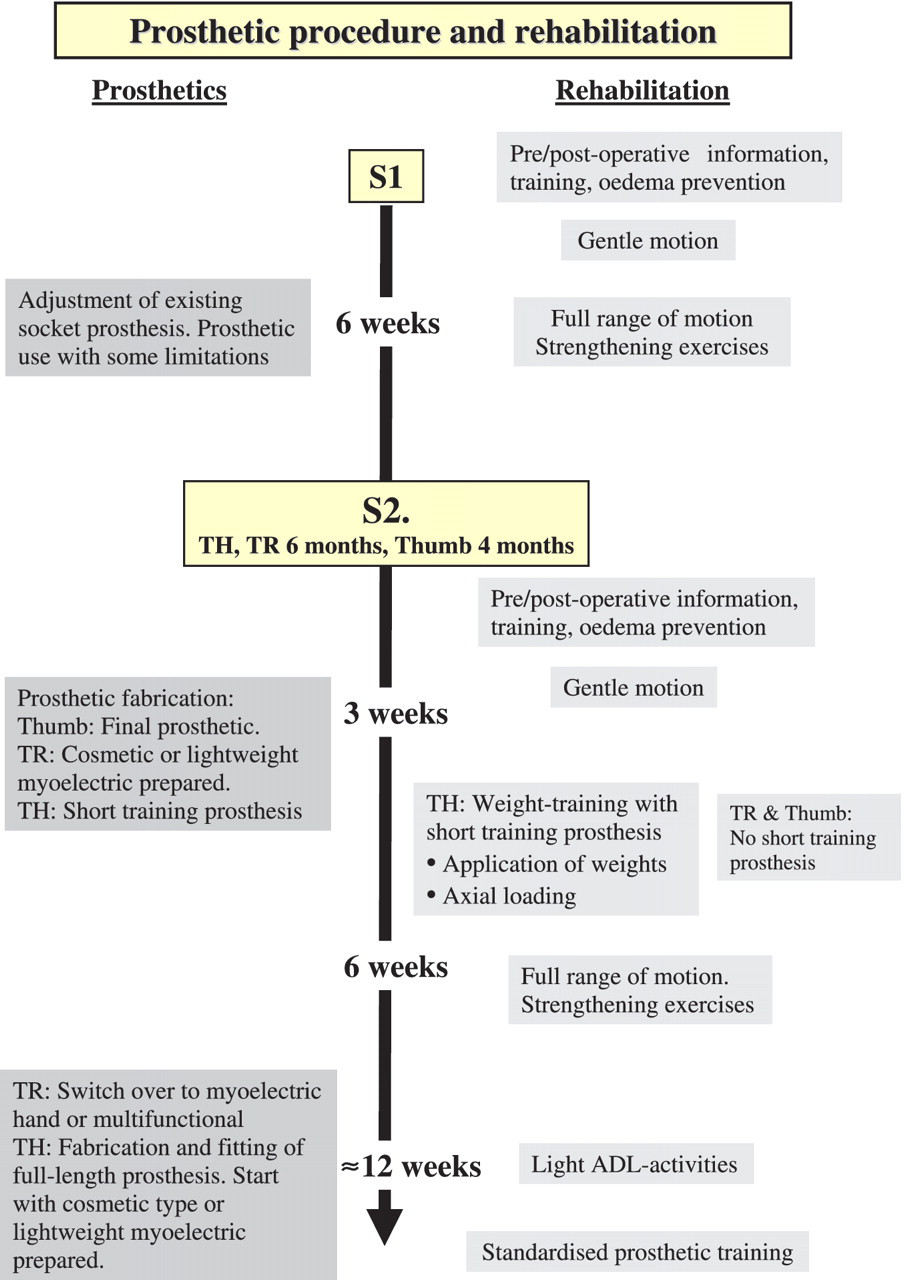
Great care is taken to stabilize soft tissues and trim skin around the abutment with the aim of attaching the skin to the end of the distal bone. After surgery, the patient follows a strict prosthetic and rehabilitation protocol (Figure 3).
Implant system. Prosthetic and rehabilitation procedures.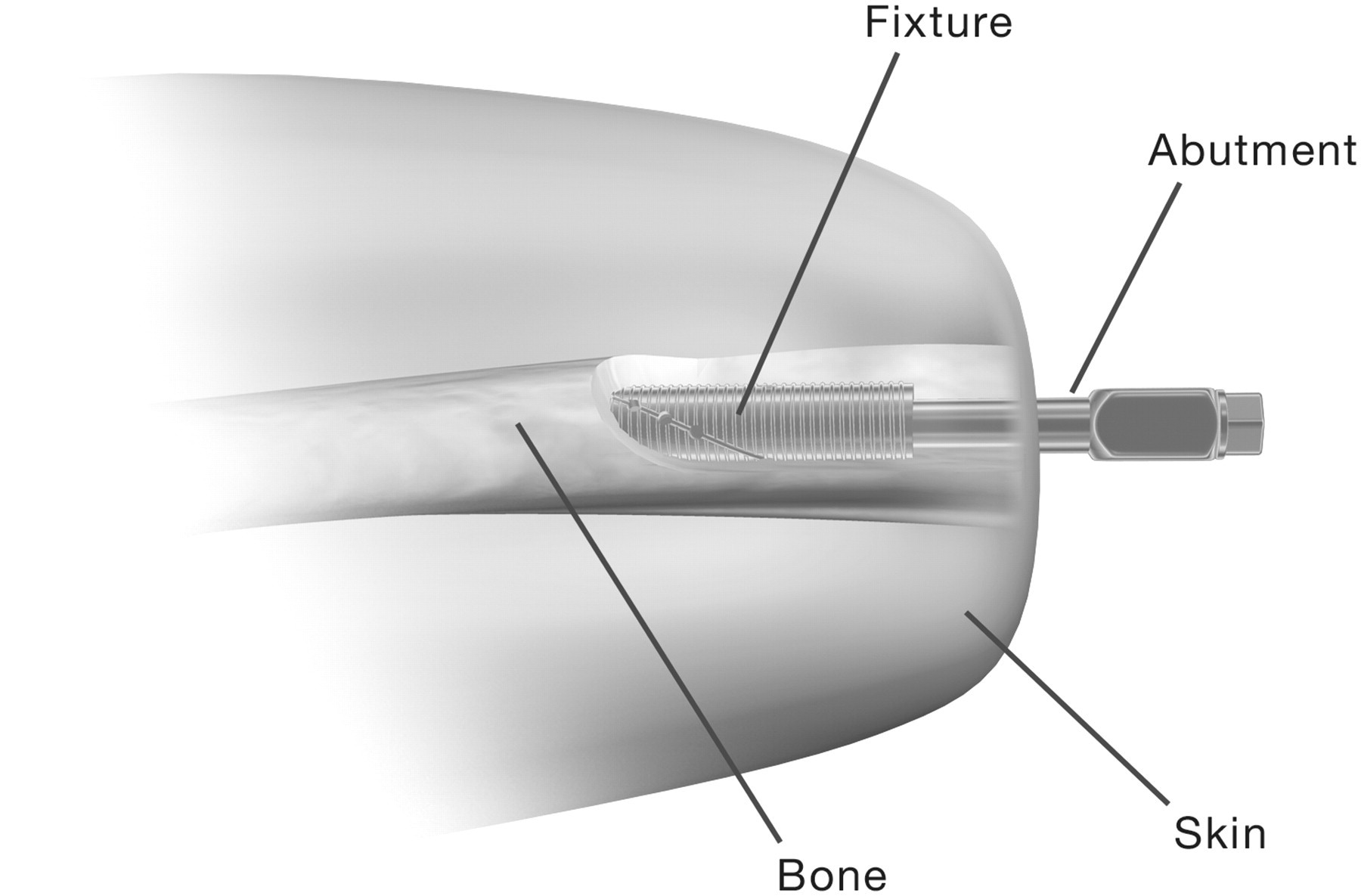
General prosthetic procedures and constructions
The first thumb amputee was treated with osseointegration (S1) in 1990, the first TR amputee in 1992 and the first TH amputee in 1994. During the initial healing period from S1 to S2 (six months), the patient is normally able to use the existing socket prosthesis with some limitations. The prosthesis has to be modified, so the distal part of the bone of the residual limb is kept unloaded. The prosthetic procedure after S2 surgery depends on the amputation level, but the aim is to gradually increase the load on the implant over time.
Specially developed osseointegration attachment devices, including the puck system, help to guarantee stable, reliable fixation of the prosthesis to the abutment (Figure 1b-c). For TH and TR levels, the attachment device is available in two standard sizes, includes a quick-locking mechanism, has low weight and is easy to keep clean. For thumb levels, the attachment device is made in one size and secured to the abutment using an Allen key. The specific components/terms and their characteristics are described in Table 1. Some amputation levels require components to protect the implant from overload in rotation/torsion. A shock absorber to avoid unwanted shock peaks or forces and a temperature insulator can be built in if needed (Table 1). In cases of myoelectric control, the electrodes are held in place with flexible bars (Figure 4). The prosthetic cosmetic cover can meet up in contact with the distal tissue of the residual limb. All constructions that leave a hollow space and closed chamber in the penetration area have to be ventilated. Moisture can cause undesirable skin conditions and increase the risk of infection. A distal cap placed over the exposed abutment can be used for protection when the prosthesis is not worn.
TH level with electrode holders. Technical terms/components and their characteristics. Orthopaedic osseointegration in the field of amputation prosthetics is a relatively new technique. Therefore it is important to define the terms and names of the components in use. Some terms are common to lower limb osseointegration treatment.
Prosthetics at TH level
A stable, reliable socket suspension for the TH amputee generally results in a harness-and-socket design that limits range of motion in the shoulder joint. Socket stability and humerus rotation are normally difficult to achieve via the socket. Suspension alternatives to avoid those problems could include angulation osteotomy or the SISA concept. 24 – 26 Both procedures require surgery and are used in combination with socket suspension.
At TH level, the prosthetic procedure begins three weeks after S2 surgery. The patient is fitted with a training prosthesis with a set of changeable weights (Figures 3, 5). The construction permits a gradual increase in load and moment over time. The training prosthesis should be used temporarily until the patient reaches the weight of the final full-length prosthesis. The final prosthesis is fixed to the abutment by a standard attachment device (Figure 1b-c). At TH level, special components such as spacers, alignment components and rotation safety devices are manufactured (Figure 1c). Some elbow joints on the market already include a reliable rotation/torsion function. In cases of myoelectric control, electrode holders are mounted (Figure 4). The first full-length prosthesis is normally a cosmetic type or a myoelectrically prepared variant. In order to keep the weight down, it is initially equipped with electrodes but with a lightweight hand without grip function and with no batteries mounted (Table 1). The prosthesis can thereafter be upgraded to a more functional type. For this amputation level, cosmetic, body-powered, myoelectric hybrid and multifunctional prostheses have been fitted (Table 2). After the osseointegration process is complete, all patients either continue to wear the initially fitted prosthesis or are upgraded to a more functional prosthetic type (Figure 3).
Training prosthesis TH level. Demographic data. TH: transhumeral, TR: transradial.
Prosthetic rehabilitation at TH level
It is important that the patient has maximum range of motion and good muscle strength before surgery to benefit from the increased motion osseointegration produces. With a bone-anchored prosthesis, the joint closest to the prosthesis is loaded in an almost normal way, a situation the patient has not experienced since becoming an amputee. After S1 surgery, the patient is instructed to perform limited range of motion of the shoulder without pain. Three weeks after surgery the patient can start to practise internal/external rotation of the shoulder to avoid rotational forces of the distal soft tissues. The aim is full range of motion by six weeks after surgery. Strengthening exercises for arms, shoulders, chest and back muscles can also be started. After S2 surgery, the patient performs the same exercises as after S1. To ensure solid attachment between the titanium fixture and the bone, the bone must be carefully subjected to loads. This is performed in a controlled way by using the short training prosthesis from three weeks after S2. First, low weights (50–100 g) are applied to the training prosthesis and these are increased each week (50–100 g) until the patient reaches the weight of the final prosthesis. Loading of the implant system is dependent on bone quality and pain. Secondly, the patient performs axial weight loading twice daily by pressing the short training prosthesis against a bathroom scale according to a special treatment plan. This procedure gives the bone/fixture interface controlled loading over time. No pain above level 4 is allowed, using the visual analogue scale. 27 Approximately 12 weeks after surgery, the patient is fitted with a full-length prosthesis without grip function. Gentle exercises are performed with the prosthesis and these increase in intensity over time. Light bilateral activities can be performed. The patient can be fitted with a heavier functional prosthesis when the surgeon decides this is possible. Functional prosthetic grip training with bilateral activities can be started.
Prosthetics at TR level
Common socket suspension techniques for this level normally work well, even though the socket sometimes produces abrasion, tissue problems, discomfort and most often reduced range of motion in the elbow joint. These problems are normally related to the length of the residual limb. A short residual limb is subjected to a high tissue load, while a long residual limb exposes more tissue to the socket interface.
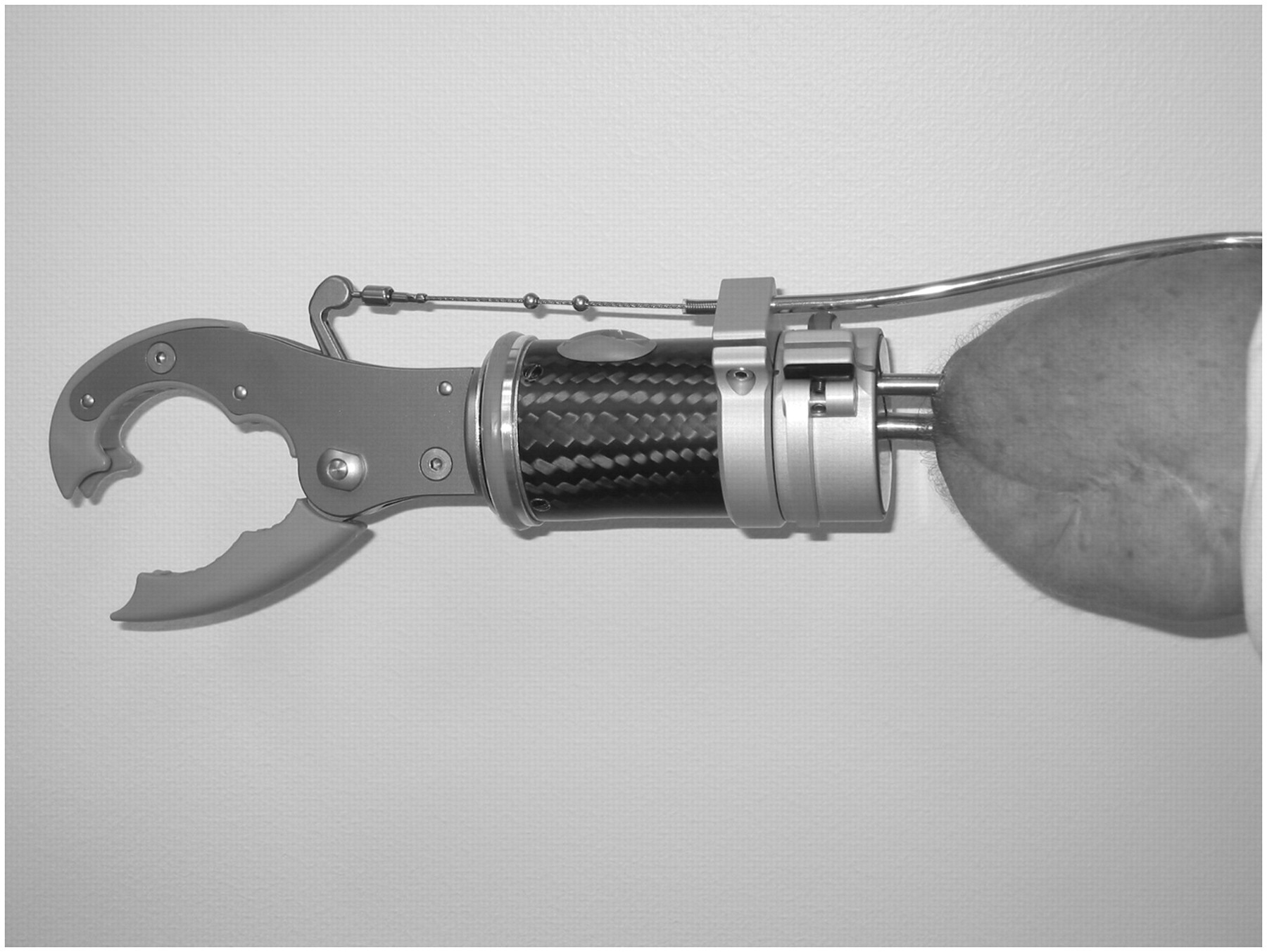
With osseointegration, implants in both the radius and ulna are used to obtain stable, reliable fixation. Two abutments follow the skeletal anatomy and penetrate the skin to form a uniquely individualized geometrical configuration. An individual impression is therefore necessary. The impression can normally be made three weeks after S2 surgery, using a special impression jig in which the abutment situation is captured in an optimal position. The impression jig allows the prosthetist to optimize the prosthetic alignment and check the prosthetic length. If there are plans for myoelectric control, the electrode sites are positioned using the jig as a reference. The geometrical situation of the abutment is copied into the plastic puck (Table 1). The prosthesis can then be produced ready for delivery without any further control or checkpoints. Active pronation and supination can be built in, but this results in much more load on the ulnar implant and is not normally used. If myoelectric electrodes are used, electrode holders are mounted. For this amputation level, cosmetic, myoelectric, body-powered and passive hook/working prostheses have been fitted (Figures 6, 7, Table 2). As at TH level, all patients were able to continue wearing the initiall fitted prosthesis or could be upgraded to a more functional prosthetic type after the osseointegration process was complete (Figure 3).
Myoelectric transradial application. Body powered transradial application.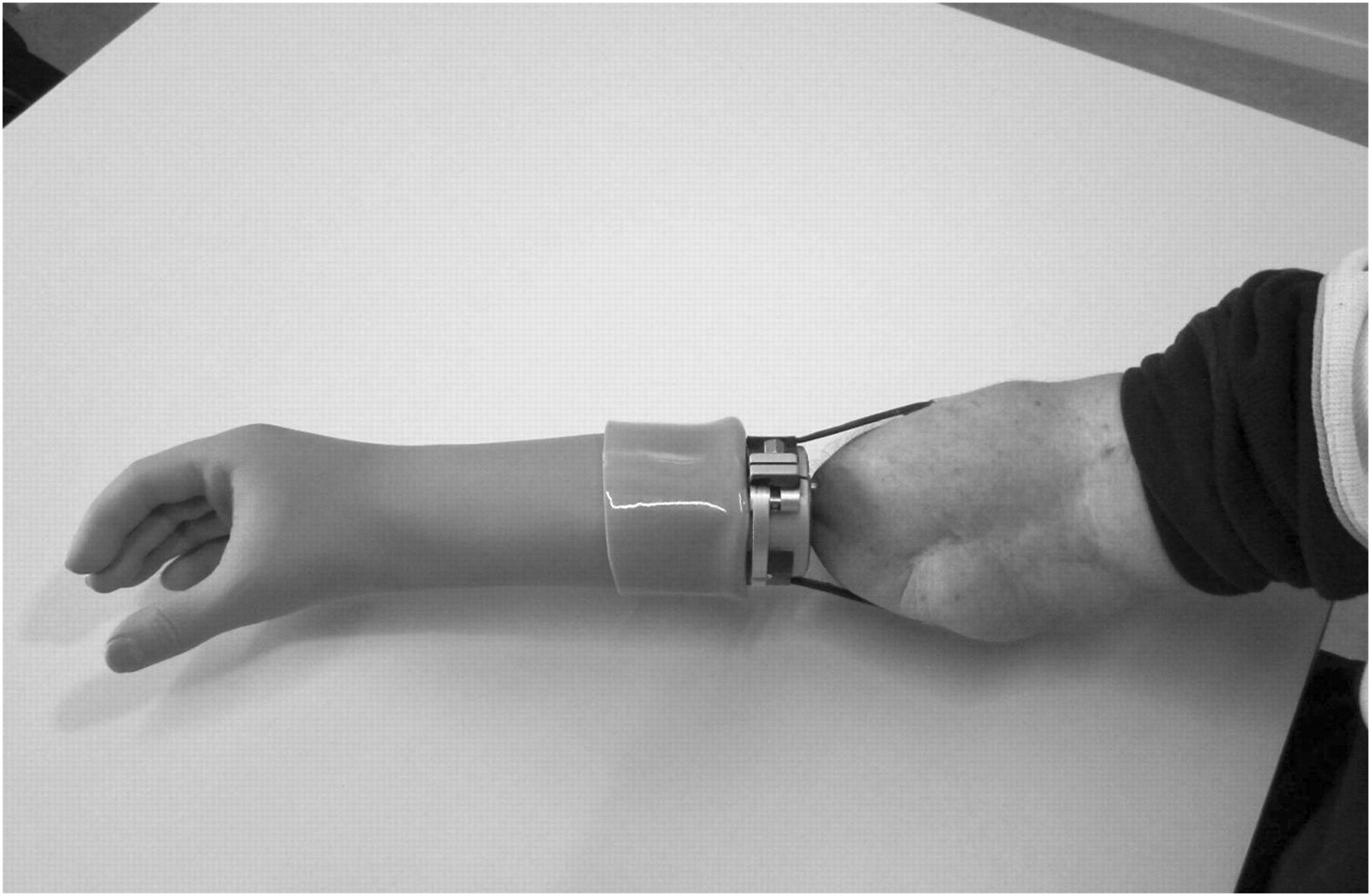
Prosthetic rehabilitation at TR level
Rehabilitation follows the same programme as for the TH level, but no short training prosthesis is used (Figure 3). The patient can wear a cosmetic or a lightweight myoelectrically prepared prosthesis and start to use the prosthesis as a support in daily activities. Based on the skeleton quality (X-ray) and pain assessment, 27 a heavier prosthesis can be used and a general rehabilitation regime followed.
Prosthetics at thumb level
The face and hands are the most visible parts of the body. Finger loss, especially thumb loss, can cause major cosmetic impact and dramatic impairment of hand function.
28
Treatments for this type of amputation can include a toe-to-finger transfer, pollicization or a prosthesis.
29
–
31
The conventional prosthesis for a thumb amputee covers a large part of the remaining hand to achieve suspension, which impairs cosmesis and function. A fixture integrated into the metacarpal bone and a skin-penetrating abutment creates an optimal platform for prosthetic fixation. The prosthetic procedure starts with an impression to capture the shape of the residual limb in relation to the abutment position. This can be done if no oedema exists, using silicone impression compounds. Some silicone prosthesis fabrication methods do not require this impression procedure. A special test prosthesis can be used to find the optimal prosthetic fingertip position. The final prosthesis is built around an attachment device with a hexagonal locking mechanism. A prosthetic inner frame, which gives the prosthesis stability, is connected to the attachment-device. The outer part of the prosthesis is normally made of silicone and gives the prosthesis a high-definition aesthetic appearance. With full freedom of movement in the proximal thumb joint, the patient has very high functionality, including positioning from a key grip to all fingertips (Figure 8a-b). The radical improvement in grip with an osseointegrated thumb prosthesis increases the patient’s hand function. High-frequency active use, however, rapidly wears down the silicone prosthesis. For this reason, patients are sometimes provided with both HD silicone and a special type of high-durability working prosthesis.
(a) Silicone thumb prosthesis. (b) Grip function with prosthesis.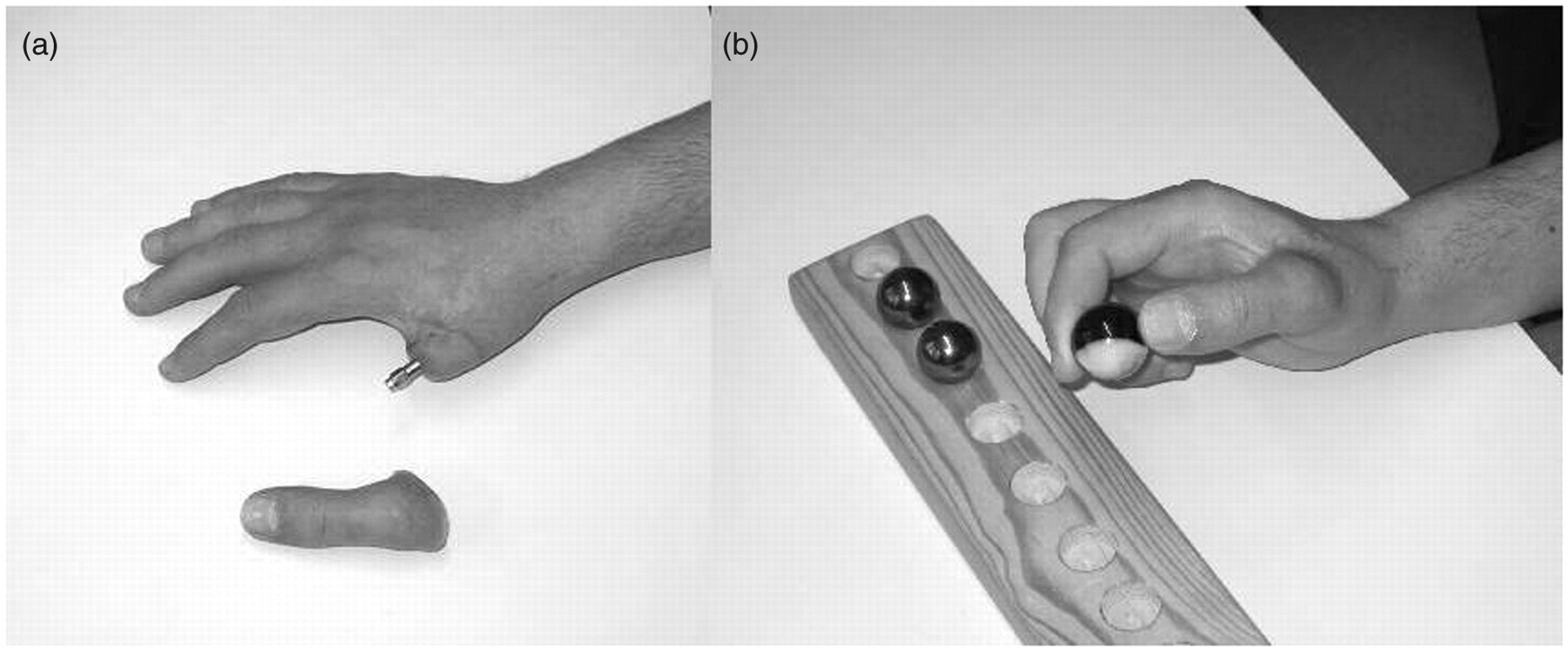
Prosthetic rehabilitation at thumb level
The healing time between the first and second operation at thumb level is reduced to only a four-month interval. Range of motion has to be exercised postoperatively and oedema must be reduced. The patient is fitted with a prosthesis when the oedema has diminished. During the first three months after surgery the thumb prosthesis should only be used for light activities of daily living. Heavy pinch/key grip should be avoided initially and the load increased over time. Pain should not exceed 4.0 on the visual analogue scale. 27
Follow-up
All patients are asked to fill in a questionnaire, consisting of 36 items relating to the residual limb and prosthetic data, ADL, quality of life and pain assessment. The disability of arm, shoulder, hand (DASH) protocol is used before S1 and after S2, 32 – 34 and range of motion is measured with and without the prosthesis. Follow-ups are carried out 1, 2, 3, 5, 7, 10 and 15 years after the S2 operation using the same questionnaires. The Sollerman grip function test, 35 Jamar and B&L pinch gauge are used for thumb and finger prostheses pre- and postoperatively. 36,37
The results of these follow-ups will be reported in a forthcoming publication.
Results
A total of 37 cases were treated with osseointegrated implants on the upper extremities between 1990 and April 2010. The mean number of years since primary amputation was 8.3 years (range 0–25 years) and the mean age at SI surgery was 40.9 years (range 18–64 years). The demographic data are shown in Table 2, and include 16 TH, 10 TR, 10 thumbs and 1 partial hand. One patient was treated bilaterally at TR level and is presented as two cases. The cause of amputation was trauma in 32 patients, congenital deformity in 3 and tumour in 2 cases; 24 were amputated on the right side and 13 on the left. There were 6 females and 31 males.
Prosthetic constructions have made it possible to provide patients with long or short residual limbs at TH and TR level. The patients have been fitted with prostheses of various types, including cosmetic, body-powered, myoelectric including multifunctional, and hybrids. A harness is never used for suspension. The average prosthetic usage time (1990 to April 2010) for TH is 5.6 years (range 0.3–15 years), TR 13.9 years (range 5–17.6 years), partial hand 10 years (range 10 years) and thumbs 8.1 years (range 0–20 years).
Seven patients are non-users today. Their limited usage time is included in the results above. One patient with a thumb amputation, treated in 2001, developed an infection and the fixture was removed five months after S2. Two patients with thumb amputations experienced loosening of fixtures because of incomplete integration shortly after prosthetic fitting in 1992/2000. Another patient with a congenital deformity at TR level was a successful user but had an overload accident that caused a fracture in one implant (usage time 1993–1998). Two transhumeral patients are non-users; one had a severe arthrosis of the shoulder joint. An arthrodesis improved the situation, but after a trauma, the arthrodesis became mobile and painful and the patient was unable to use the implant for suspension, so the abutment was removed and the patient now has a ‘sleeping’ implant. This was not an osseointegration-related problem (partial usage time 1997). The second TH case failed because of incomplete integration after two surgical trials (temporary usage time 2005–2009). In one partial congenital hand amputee, the implant was removed (functional usage time 1995–2005). The patient experienced improved suspension and stability from the osseointegration, but the improvement did not override the long-term disadvantages. The main problem was related to the lack of protection of the distally placed abutment, which caused substantial problems for the patient when the prosthesis was not being used.
Discussion
Over the years, a number of socket designs have been presented. 38 Prosthetic socket suspension generally works well, but socket-related problems develop in association with soft tissue loading. The osseointegration programme in Sweden includes developments in several areas and involves different professions. Techniques and methods have been refined and optimized over time. The puck system has been the attachment design of choice for all transradial and transhumeral amputation levels since 1993. Other components have been customized to adapt to this technical solution. It has been possible to fit cosmetic, body-powered, myoelectric, hybrid and multifunctional prostheses with good results. The training and rehabilitation method was developed along with checks-up for outcome assessment.
Most candidates for the osseointegration procedure had a history of problems with their previous socket prostheses. The majority suffered from skin/tissue problems, had problems with sweating, or had extremely short residual limbs, which in some cases caused low prosthetic use or nonuse. 6,39 Many of these problems have been resolved using the osseointegration technique, which eliminates the need for a socket. Full perception of touch at the residual limb surface is achieved with osseointegration due to full skin exposure (Figure 6). Exceptionally short TH stumps have been treated with good results. The patient achieves full freedom of motion in the proximal joint without the restriction of a socket. EMG detection has been solved using a special electrode holder, but with a very high level of TH amputation there can be EMG interference from the shoulder muscles when moving and positioning the prosthesis. It is to be hoped that new technology, such as nerve coupling, etc., could be a future solution. 40 The harness causes discomfort, 2,8,41 and as no harness is needed for suspension, a higher degree of comfort can be accomplished. Donning and doffing is simple and the prosthetic fixation is reliable. Patients also experience improved sensory feedback because of the phenomenon of osseoperception. 22,28,42 – 45
Without any residual limb volume to consider, direct bone-anchored prostheses always fit and have long durability. The need for prosthetic replacement is not frequent, and worn-out sockets are no longer an issue. This reduces the prosthetic cost over a long time period. No negative effects of osseointegration have been reported in the working situation and patients have a wide spectrum of jobs, ranging from office work to heavy-duty farming. Concerning patients’ family life, a small number of patients mention that the protruding abutment can be disturbing in specific situations when they are not using their prosthesis, for example, when performing baby care. A special baby-care prosthesis was made for one TH with good results. Patients can be provided with a ‘distal cap’ for protection, which can be used when not wearing the prosthesis.
The long prosthetic usage time for the TR level is a result of early surgery in the 1990s and, when it came to the thumb level, 6 patients were treated before 1999. On the other hand, only three patients had undergone surgery at the TH level before 1999 and the majority received treatment from 2003 to 2009.
Conclusion
Osseointegration has the potential to change the rehabilitation strategy for selected upper limb amputees and is a very important platform for introducing new prosthetic technology, due to the stable fixation. Further reports on complications and outcome data, including quality of life assessment, will enhance the clinical relevance of this new treatment concept.
Footnotes
Funding
This research was supported by ALF-grant, Sahlgrenska University Hospital and University of Gothenburg.