
Abstract
Background:
Transfemoral amputees have decreased ability to descend ramps and hills. The Hill Assessment Index quantifies transfemoral amputee ramp performance, but interrater reliability has not been assessed.
Objectives:
To determine whether C-Leg use improves hill descent gait and evaluate the Hill Assessment Index’s interrater reliability.
Methods:
Twenty-one transfemoral amputees descended a ramp while timed and video recorded, using their nonmicroprocessor prosthetic knee. Subjects were fitted and accommodated with a C-Leg and retested. Test times were compared, and ramp performances were independently reviewed using the Hill Assessment Index by two raters. Hill Assessment Index scores were compared between knee conditions within raters for performance and between raters to assess the Hill Assessment Index’s interrater reliability.
Results:
Mean Hill Assessment Index scores were greater for C-Leg compared to nonmicroprocessor prosthetic knee for both raters. C-Leg resulted in faster ramp descent. Strong correlations resulted between raters on Hill Assessment Index scores for nonmicroprocessor prosthetic knee (intraclass correlation coefficient = 0.97) and C-Leg (intraclass correlation coefficient = 0.99).
Conclusions:
C-Leg improves Hill Assessment Index ramp descent performance and time. In descent quality, C-Leg offers the possibility of eliminating assistive device use and/or improving step length in the absence of an assistive device. C-Leg resulted in 23% gait speed increase during ramp descent. The Hill Assessment Index had very good interrater reliability but should be assessed for intrarater reliability, minimal detectable change, and validity.
Clinical relevance
Transfemoral amputees have difficulty ambulating on ramps. While the C-Leg has been shown to improve ramp descent, this has not been confirmed, and the Hill Assessment Index has not been studied for reliability. This study confirms that the C-Leg improves ramp descent performance and the Hill Assessment Index’s interrater reliability.
Background
Ambulation on sloped terrain such as ramps and hills is associated with increased potential for slipping, loss of balance, and falling. Among the many causes for this is the fact that ramp and slope walking requires kinematic changes to traditional stepping patterns used to traverse flat ground. 1 Individuals with decreased ability to make these changes will likely have poorer ramp gait performance. Transfemoral amputees (TFAs) comprise a group that will likely have difficulty ambulating on sloped terrain. 1
TFAs’ use of artificial knee and ankle joints, predominantly designed for flat ground gait, will require different gait strategies and deviations from those used by nonamputees in order to walk on sloped surfaces. For instance, in downhill walking, knee flexion is increased through much of stance phase and into early swing to facilitate a gentle lowering of the body to decrease contact force from subsequent steps. The TFA’s ability to increase and modulate these and other motions at the knee and ankle, as typically done by nonamputees, will be limited based on multiple factors such as loss of anatomy, component function, and more. 1
Because ambulatory TFAs will likely encounter sloped terrain in daily activity, contemporary prosthetic components are including ramp gait functions. The C-Leg (Otto Bock, Duderstadt, Germany) is a microprocessor knee that controls the rate of flexion 2 and has recently been shown to improve the quality of hill descent. 3 Buell et al. 4 developed an instrument called the Hill Assessment Index (HAI), which was used to quantify ramp gait quality in the aforementioned study. 3 The HAI is an 11-item instrument (Figure 1) that scores the quality of TFA gait on sloped terrain based on the following factors or combinations of them:
Willingness to perform the task;
Use of assistance;
Direction of gait relative to the slope;
Step length.
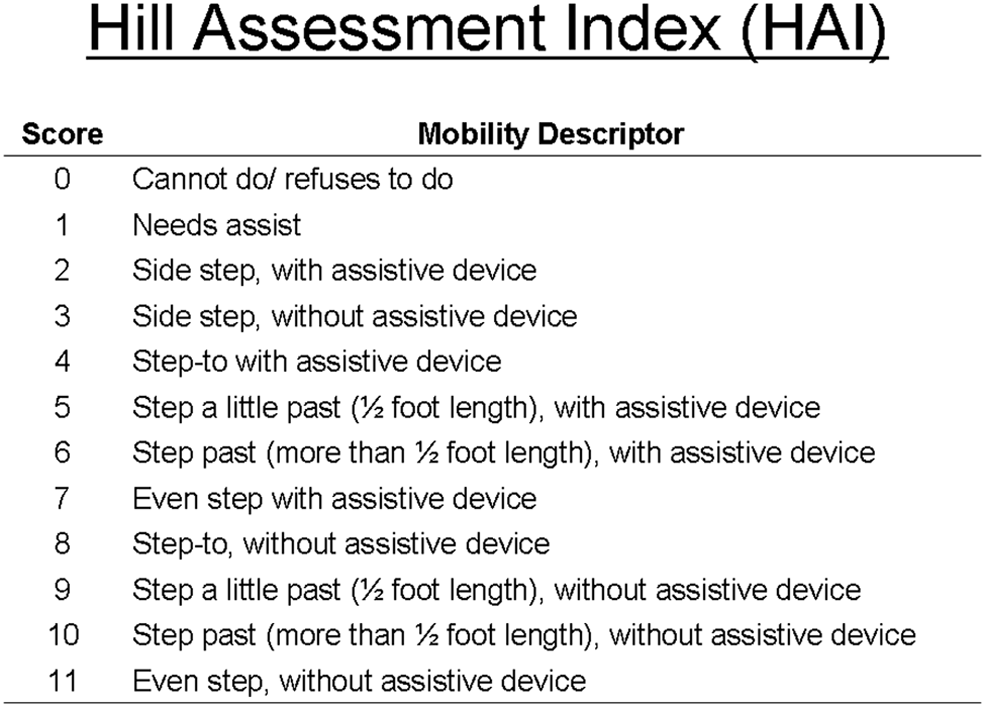
HAI rating system. The HAI represents ordinal scale data.
While the HAI has previously been used to evaluate the quality of sloped terrain gait in TFAs, 3 it has not been formally evaluated for reliability. Furthermore, there has been sparse evidence corroborating the improved gait quality in ramp descent observed by using the C-Leg. Therefore, this study had two purposes: the primary purpose was to determine whether the improved gait quality on ramp descent could be replicated with the use of the C-Leg microprocessor knee (MPK) and the secondary purpose was to evaluate the interrater reliability of the HAI.
Methods
All subjects gave informed consent to participate, and this study was approved by the University of South Florida’s Institutional Review Board. Subject inclusion criteria included
Unilateral transfemoral or knee disarticulation amputation;
Self-reported or known use of a nonmicroprocessor prosthetic knee (NMPK) for 90 days or more prior to enrollment;
Independent level of community ambulation without an assistive aid (e.g. cane, walker);
Ability to descend a ramp without human support;
Willingness to utilize a C-Leg for 90 days.
Knee accommodation and ramp task performance
All subjects entered this study using their previously accommodated and physician-prescribed NMPK. Subjects were enrolled in this study and asked to continue wearing their NMPK for two additional weeks before testing their ramp performance to minimize the acute influence associated with being enrolled in a study. Subjects were then asked to descend a ramp 0.9 m in width and 4.9 m in length that was sloped at an Americans with Disabilities Act compliant angle of 5°. 5 Subjects were asked to walk down the length of the ramp at a comfortable, self-selected pace and to use the handrails as they deemed necessary. Each subject’s trial was timed and videotaped for HAI scoring independently by two separate raters. Raters independently scored the ramp walking performances by reviewing the video recordings and determining which HAI value applied based on the criteria outlined in Figure 1.
Following the initial ramp descent task, subjects were fitted with a C-Leg (Otto Bock) and given 90 days in which to accommodate with the knee. “Subjects’ original sockets and feet were retained” such that only the knee mechanisms were changed. Prostheses were fit and aligned by an American Board for Certification in Orthotics, Prosthetics and Pedorthics credentialed and state licensed prosthetist. The prosthetist was also trained and certified to fit the C-Leg system by the manufacturer. Observational gait analysis was used to align prostheses.6,7 Alignments and adjustments were set to maximize safety and all functions (e.g. gait, stair, ramp, etc.) as opposed to exclusive optimization specific to ramp performance. Unless additional visits were deemed necessary, subjects were asked to follow up once per week for 2 weeks at a minimum and then invited to visit with the study prosthetist as needed up to the 90-day accommodation point. Following the 90-day accommodation period, subjects were asked to walk down the experimental ramp a second time. Both raters independently scored the ramp performances using the HAI from the video recordings.
Statistical analysis to determine ramp descent performance and reliability of the HAI
Because the HAI represents ordinal data, the following comparisons were made using the Wilcoxon Signed-Rank test:
Rater 1: sample mean HAI score NMPK versus C-Leg
Rater 2: sample mean HAI score NMPK versus C-Leg
Sample mean HAI score NMPK: Rater 1 versus Rater 2
Sample mean HAI score C-Leg: Rater 1 versus Rater 2.
Comparison numbers 1 and 2 above indicate ramp performance between the two knee conditions. As an additional ramp performance indicator, mean ramp descent duration (ratio scale data) was compared using a paired sample t test between the two knee conditions. Comparisons 3 and 4 were used as indicators of interrater reliability for the HAI as each rater provided a single HAI score for each subject in the NMPK condition and then a single score each for the C-Leg condition. In addition to comparisons 3 and 4 above, interrater reliability for individual HAI scores was further evaluated by calculating the intraclass correlation coefficient (ICC) using Spearman’s Rho for ordinal data (HAI scores). Statistical significance was determined at the p ≤ 0.05 level. Statistical analyses were performed by an investigator blinded to the data collection with SPSS software v.19 (IBM, Armonk, NY, USA).
Results
Sample demographics
Twenty-one (n = 21) individuals with unilateral TFA comprised the sample. The sample included 11 males and 10 females with a mean (SD) age of 52.1 years (±18.6 years) and mean (SD) body mass index of 23.6 kg/m2 (±4.2 kg/m2). Amputation etiology was as follows: eight peripheral vascular disease, eight traumatic, four congenital, and one malignancy. All subjects were independent community ambulators. Ten subjects had a self-reported history of NMPK use between 6 and 12 months prior to this study. The remaining 11 subjects had a self-reported history of NMPK use of >1 year. The initial NMPKs used were as follows: polycentric (11), weight activated stance braking (5), Mauch swing and stance (SNS) (4), and single axis (1). A variety of feet were used with the NMPKs: energy storing feet (13), flexible keel (4), multiaxial (3), and solid ankle cushioned heel (SACH) (1). All subjects utilized manufacturer approved energy storing feet (Otto Bock) with the C-Leg.
Statistically significant differences (p ≤ 0.05) in mean HAI scores were found for both raters’ NMPK and C-Leg scores. Significant differences were also found in the duration to complete the ramp task with the C-Leg requiring less time to descend the ramp (Table 1).
Ramp descent performance for both raters in HAI and time.
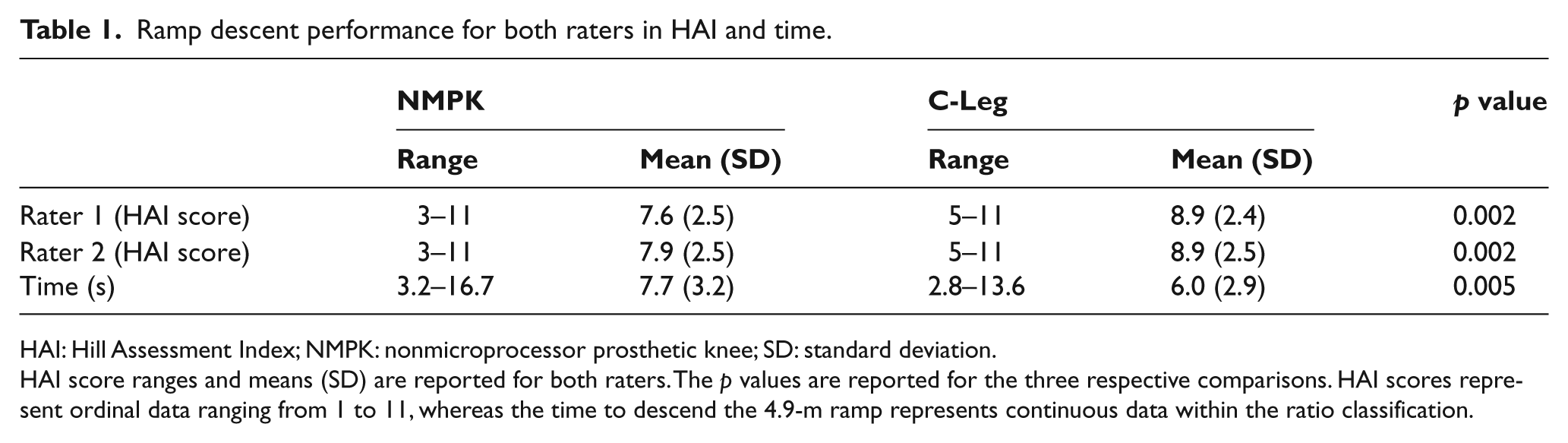
HAI: Hill Assessment Index; NMPK: nonmicroprocessor prosthetic knee; SD: standard deviation.
HAI score ranges and means (SD) are reported for both raters. The p values are reported for the three respective comparisons. HAI scores represent ordinal data ranging from 1 to 11, whereas the time to descend the 4.9-m ramp represents continuous data within the ratio classification.
Significant differences were not observed between HAI scores of Rater 1 and Rater 2 for the NMPK condition (Table 2). Similarly, no significant differences were observed between the two raters’ independent mean HAI scores for the C-Leg condition. Instead, strong correlations were found between the two raters on HAI scores for both the NMPK (ICC = 0.97; p = 0.01) and the C-Leg (ICC = 0.99; p = 0.01) (Figure 2).
Hill Assessment Index scores for Raters 1 and 2 per subject in each knee condition.
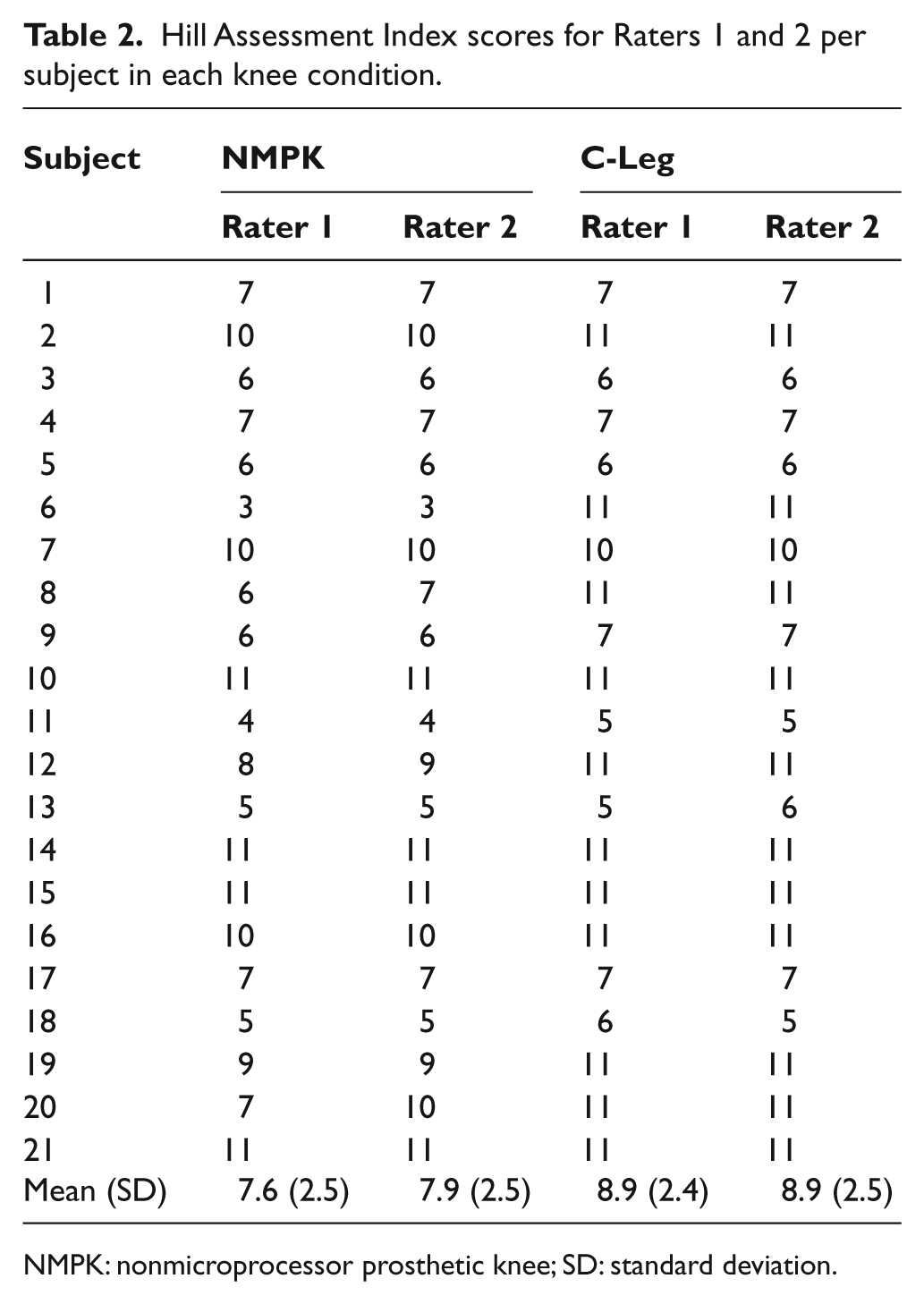
NMPK: nonmicroprocessor prosthetic knee; SD: standard deviation.
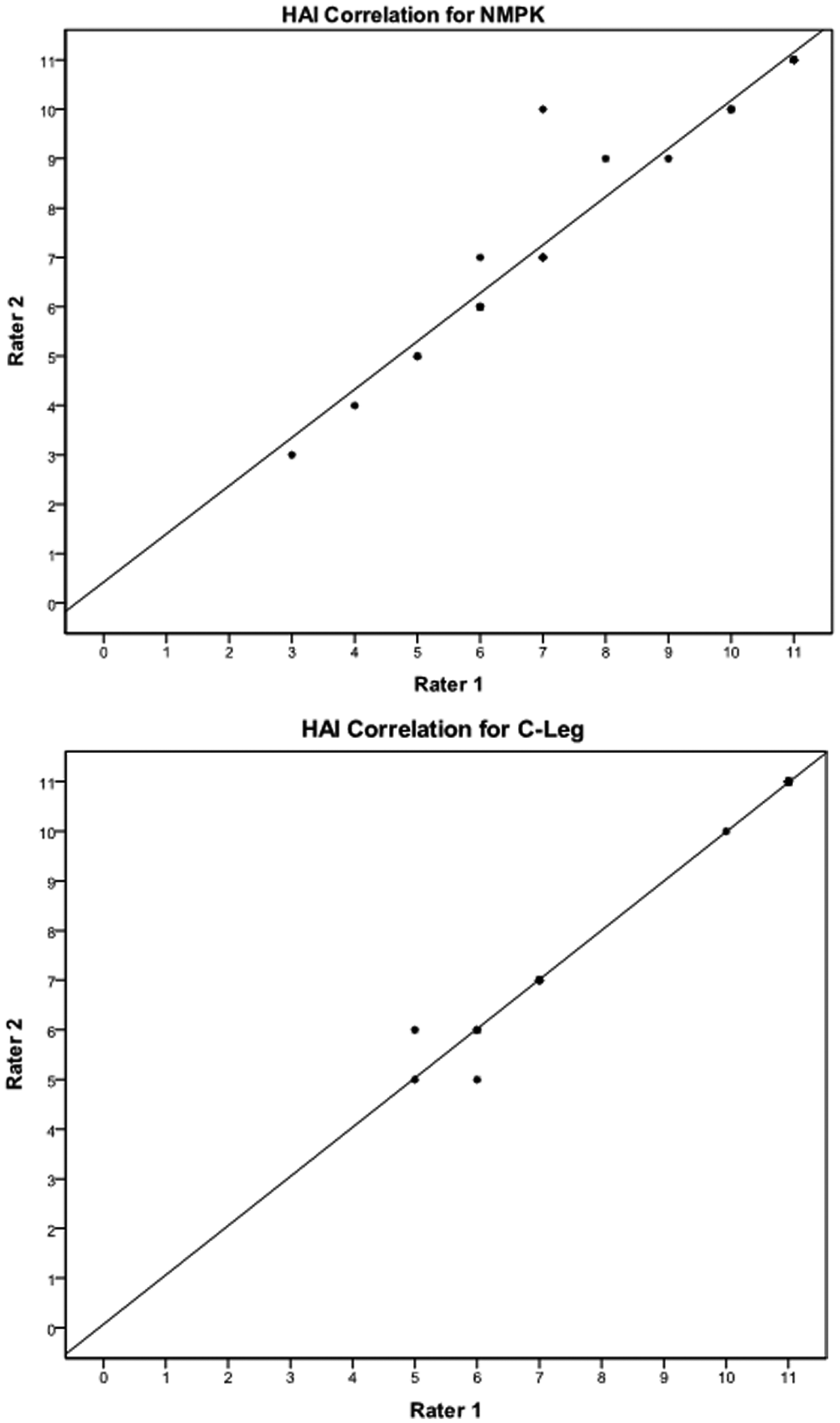
Correlations for interrater reliability. Spearman’s Rho correlation for NMPK was ICC = 0.97 (p = 0.01) and for C-Leg was ICC = 0.99 (p = 0.01).
Discussion
Ramp descent performance with HAI
In accordance with Hafner et al.’s 3 previous findings, we hypothesized that accommodation and use of the C-Leg would improve ramp descent performance in terms of both HAI scores and time to complete the task. Hafner et al. observed ramp descent over a slope of 28.2 m length in 19 TFAs. In their study, subjects achieved higher HAI scores with the C-Leg (approximately 7.7/11) compared to the comparator NMPK (approximately 6.3/11). 3 Relative to the performance of this sample in which NMPK ramp descent resulted in mean HAI scores of 7.6 and 7.9 (Raters 1 and 2, respectively) and the C-Leg yielded a score of 8.9, the magnitude of HAI score difference is highly comparable. That is, the use of the C-Leg appears to increase the HAI score, or the ability to descend an Americans with Disabilities Act (ADA) grade ramp, by approximately 1.1 to 1.4 points. In Hafner et al.’s case, this was the difference between descending the ramp by having a slight asymmetric step length while using an assistive device (possibly the ramp railing) with the NMPK and using a step to gait pattern without an assistive device. In the case of this sample, the difference on average was approximately use of a step to gait without railing in the NMPK compared to utilization of an asymmetric step through gait without railing as noted observationally. Ten subjects realized no change in HAI score between knees. Impressively however, one subject utilized a side step strategy (HAI of 3/11) when using his or her NMPK and improved to a normal forward stepping approach with even steps without an assistive device (HAI of 11/11). Given that HAI scores from both raters in this study were significantly different when comparing mean (SD) scores and that the scores are comparable and in such favorable agreement with those reported previously, it is clear that the C-Leg can improve ramp descent performance at an ADA grade as measured by this instrument. One issue that remains unclear is whether a step to or step through gait is a more realistic goal in a comparable group of TFAs.
A few issues do however become apparent through the former discussion relative to HAI scoring. First, it is critical in scoring the HAI that raters be clear that assistive devices are to include hand railing (or not) as determined uniformly by the clinical or research team such as not to introduce a measurement error. Therefore, instructing new raters on the particular protocol in place locally is critical. Second, the orientation of the rater relative to the ramp is important. That is, viewing the ramp from a vantage point such that a sagittal view is apparent is vital in order to determine the two criteria that comprise a sizable portion of HAI scoring. Those are the direction of travel down the length of the ramp as well as the step length as viewed one foot relative to the other when scoring observationally. These two elements are involved in 10 of the 11 points on the HAI (Figure 1). For this reason, we found that recording the performance and reviewing the video after the fact was helpful in determining whether step lengths were equal or greater or less than the length of the contralateral foot length. On this issue, future studies may consider looking at precision and therefore validity of HAI scoring against instrumented measures of step length.
A limitation of the instrument is the scoring relative to the mere presence or absence of an assistive device. Again, the use of railing constitutes use of an assistive device regardless of whether the use is at an incidental, haptic, or considerable weight-bearing level. Differentiating between these levels can be observationally difficult without the use of kinetic instrumentation but again would further distinguish true ability to descend a ramp considering the level of dependency on an assistive device. The use of an assistive device was an exclusion criteria for our study, which offers partial explanation for the higher scores in this study; however, a number of amputees may utilize an assistive device such as a cane for some terrain situations and not others or some ramp grades but again, not others. As the instrument is presently designed, assuming a comparable step length at two different slopes, loosely carrying a cane for one slope and relying on it heavily on another would be scored equally despite the true use of the device.
Ramp descent performance with time
Subjects descended the ramp approximately 12% faster while using the C-Leg compared to the NMPK. We previously demonstrated that using the C-Leg increases gait speed on flat ground whether the surface is flat (i.e. concrete sidewalk) or uneven (i.e. rocks, dirt, grass). 2 Similarly, we demonstrated that the C-Leg increases stair descent velocity. 2 In both cases, it should be noted that increasing gait speed must be controlled for safety purposes. The C-Leg has been well studied for its ability to dampen flexion and control stumbles and falls and thus improves safety while simultaneously increasing gait speed in TFAs. 8 This is functionally significant as TFAs are known to ambulate slower than transtibial amputees and nonamputees. 9
Hafner et al.’s sample descended the ramp at a velocity of approximately 0.52 m/s with the NMPK and 0.72 m/s with the C-Leg. 3 This represents an approximate 28% increase in velocity with the C-Leg use on the ramp. This sample increased their ramp descent velocity from an average of 0.63 m/s with the NMPK to 0.82 m/s with the C-Leg, which is also a highly comparable gait speed increase (approximately 23%) relative to that reported by Hafner et al. Given that gait speed is known to increase by using the C-Leg on flat ground and the fact that two studies corroborate a gait speed increase on ramp descent at an ADA grade, it is also clear that the C-Leg increases the speed of ramp descent gait in this population.
Interrater reliability of the HAI
It is important to know whether an instrument is providing consistent information and scoring on repeated administrations so that raters can be confident that changes in performance may be associated with actual performance differences as opposed to instability of the instrument. Given that the custom-designed HAI was created ad hoc, it has not been evaluated to date for reliability. We evaluated interrater reliability first by determining whether HAI scores for the NMPK condition were significantly different between Raters 1 and 2. This was repeated for the C-Leg condition, and no significant differences were observed. The difference in means between Rater 1 and Rater 2 for the NMPK condition was approximately 4%, and there was no difference in mean HAI scores between raters in the C-Leg condition. The next step was to determine agreement in HAI scores, per knee condition between the two raters. Through two measures, strong correlations, that is, strong agreement, were found in both knee conditions between raters. This indicates two different raters would be able to utilize the instrument independently and arrive at a highly comparable score. So long as the differences between scoring parameters are agreed upon prior to scoring, separate raters can be confident that comparable scores on the HAI will be reached.
Limitations
Limitations of this study include that subjects were not blinded to the intervention. This has been the subject of debate in prosthetic literature wherein safety and ethical considerations at times limit or preclude the ability to blind components such as prosthetic knees. 8 Subjects were not randomized to the intervention sequence, and therefore, an order of effect bias could adversely impact the effect size of the results. However, the sequence used was chosen to be consistent with two factors: (1) the most common ecologically valid clinical sequence of C-Leg transition from NMPK and (2) the sequence in which third-party reimbursement groups will experience the transition and make funding decisions. Finally, this study represents a first step in evaluating the HAI. In this case, the interrater reliability was evaluated. Comprehensive evaluation would include other such assessments as intrarater reliability, minimal detectable change, and comparison to other hill/ramp metrics to assess validity of the HAI.
Conclusions
This study confirms that accommodation with and use of a C-Leg can improve ramp descent performance at an ADA grade in terms of HAI scores and time to descend the ramp. Relative to ramp descent quality, use of the C-Leg appears to offer the possibility of removing the use of an assistive device when present and/or improving step length from a step to gait pattern to an asymmetric step through pattern in the absence of an assistive device. The use of the C-Leg also resulted in a 23% increase in gait speed during ramp descent. Finally, the HAI was found to have very good interrater reliability but should be further assessed for intrarater reliability, minimal detectable change, and validity.
Footnotes
Conflicts of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding in the public, commercial, or not-for-profit sectors.