
Abstract
Background:
Patterns and ease of stair ambulation influence amputees’ level of satisfaction with their rehabilitation, confidence level, and motivation for continued rehabilitation, demonstrating the importance of stair-ascent data for rehabilitation. However, little is known about the determinants of stair-ascent patterns in unilateral transfemoral amputees.
Objectives:
To investigate the factors affecting stair-ascent patterns in transfemoral amputees.
Study Design:
Cross-sectional survey.
Methods:
Stair-ascent patterns were evaluated using the Stair Assessment Index. We collected Stair Assessment Index data as well as demographic and clinical data (sex, age, height, mass, amputation side, reason for amputation, time since amputation, and residual limb length) from 25 transfemoral amputees.
Results:
Statistical analyses revealed that age was negatively correlated and time since amputation was positively correlated with Stair Assessment Index. In contrast, height, body mass, and residual limb lengths were not correlated with Stair Assessment Index.
Conclusion:
The results of this study suggest that in unilateral transfemoral amputee, (1) both age and time since amputation could affect stair-climbing patterns and (2) residual limb length should not be a limiting factor for stair climbing if the transfemoral amputee has a certain minimum residual limb length.
Clinical relevance
Rehabilitation teams should carefully consider nonmodifiable predisposing factors such as age and time since amputation. However, they may be able to carry on stair-ascent rehabilitation for transfemoral amputees disregarding residual limb length (depending on the length).
Background
Stairs are a common obstacle encountered by amputees in daily life. Although several studies demonstrated that able-bodied people and people with transtibial amputation can climb stairs in step-over-step manner,1 –6 this movement is a very demanding task for transfemoral amputees (TFAs).6 –8 Indeed, Narang et al. 9 reported that more than 90% of TFAs needed handrails or other assistance in stair climbing. In other words, the majority of TFAs used a step-to-step or skipping pattern to climb stairs, using a handrail or special assistive device.7,8,10,11 However, some TFAs could climb stairs using a step-over-step gait pattern without handrail use or any assistive device. 12 Although patterns of stair ambulation can influence physiological cost, efficiency, and speed,13,14 little is known about the determinants of the stair-ascent pattern in TFAs.
Several rating scales exist to evaluate ambulatory ability in amputees. The Functional Independence Measure (FIM) is currently the most widely used and accepted functional assessment in rehabilitation.15,16 However, Buell et al. 10 clearly showed that the FIM could not be utilized to discriminate stair-climbing patterns in amputees owing to the apparent ceiling effect. Another clinical scale including items related to stair climbing is the Climbing Stairs Questionnaire (CSQ).17,18 The CSQ is a patient-reported 15-item questionnaire that measures activity limitations in climbing stairs.17,18 The sum score is standardized (range = 0–100), with higher scores indicating less limitation (more mobility) in climbing stairs. Similarly, the Locomotor Capabilities Index (LCI) is a 14-item questionnaire specifically designed to measure walking ability in lower limb amputees.19,20 However, like FIM, neither CSQ nor LCI is sufficient to evaluate stair-climbing patterns, because both ratings have no items that specify stair-climbing patterns in detail.
In this regard, the Stair Assessment Index (SAI) is a unique and useful tool to evaluate stair gait patterns in TFAs.10,11,21 The SAI was originally utilized to assess subjects’ ability to descend a 12-step, Americans with Disabilities Act–compliant stairwell and to score them for functional independence and technique by using the 14-level SAI scale. 11 Buell et al. 10 and Hafner et al. 11 demonstrated that the mean SAI score in TFAs was approximately 5 (“Without rail or assistive device, step-to-step pattern”) when TFAs used both mechanical (nonmicroprocessor) and microprocessor knee joints. However, the factors affecting SAI score in TFAs are still unknown.
The purpose of this study was to investigate the factors affecting stair-climbing patterns in TFAs. Past findings suggest that ambulation ability in amputees was positively influenced by a greater number of years since amputation, but negatively influenced by age. 22 Furthermore, Arwert et al. 23 reported that residual limb length is of significant influence in ambulatory activity in amputees. Thus, in this study, we hypothesize that (1) SAI during stair ascent in TFAs will be correlated with both age (negatively) and time since amputation (positively) and (2) SAI will be positively correlated with residual limb length.
Methods
Participants
Eligible participants were identified using the following criteria: (1) unilateral transfemoral amputation, (2) age greater than 20 years, (3) not residing in a care–support situation, (4) using their prosthesis for primary ambulation (with or without the use of gait aids), and (5) cognitively capable of answering interview questions. Our TFA volunteers did not have skin problems or any other balance limitations. Participants with multiple limbs amputated were excluded. The protocol was approved by the local ethics committee and is in accordance with the guidelines set out in the Declaration of Helsinki (1983).
Demographic data and SAI
We collected demographic and clinical data (sex, age, height, body mass, reason for amputation, time since amputation, and residual limb length) from each participant. Stair-ascent pattern was evaluated using the SAI, which was administered by telephone interview in discharged patients or self-report at an ambulatory rehabilitation facility. First, a prosthetist asked the participant about their stair-ascent pattern in climbing up the stairs (“How do you climb up stairs in daily life?”). Then the participant’s answers were scored using the SAI scale.
Statistics
A Shapiro–Wilk normality test was performed to ascertain whether SAI in this study was normally distributed. 24 Pearson’s correlation coefficients were used to examine the relationship between the demographic data (age, height, body mass, time since amputation, and residual limb length) and SAI. In addition, we calculated partial correlation coefficients, which indicate the contribution of a predictor after the contributions of the other four predictors have been taken out of both that predictor and the dependent variable. Statistical significance was set at p < 0.05. SPSS for Windows (IBM SPSS Statistics Version 19; SPSS Inc., Chicago, IL, USA) was used for all statistical analysis. All data are presented as the mean (M) ± standard deviation (SD).
Results
Demographic data and SAI
Demographic data and SAI are shown in Table 1. Twenty-five subjects (2 females and 23 males), aged 20–74 years (45.7 ± 14.9 years), were recruited for participation in the survey. The average height and body mass were 1.68 ± 0.06 m (1.53–1.83 m) and 63.8 ± 10.1 kg (46.0–80.0 kg), respectively. The mean ± SD time since amputation was 20.93 ± 23.53 years (1–55 years). The mean ± SD residual limb length was 21.3 ± 4.4 cm (11.0–30.5 cm). Arithmetic mean ± SD and median of SAI were 6.2 ± 3.4 and 5, respectively. The Shapiro–Wilk normality test revealed that the SAI in this study was normally distributed. Furthermore, the reasons for amputation included traumatic (84%), oncologic (12%), and vascular factors (4%).
Subject demographic data.
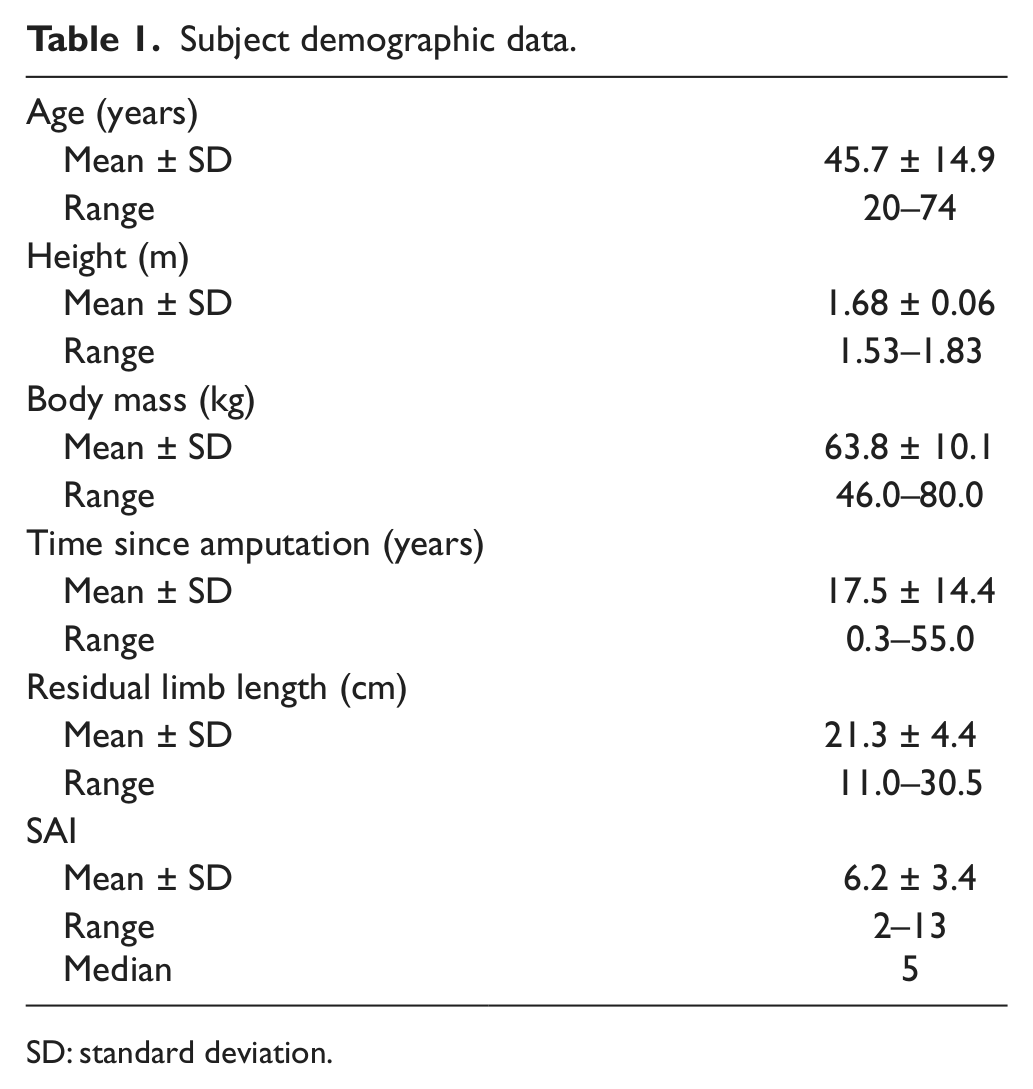
SD: standard deviation.
Correlation between demographic data and SAI
As shown in Table 2, Pearson’s correlation coefficient of age (−0.264) and time since amputation (0.368) was slightly greater than those of height (−0.197), mass (−0.215), and residual limb length (0.077). However, there were no significant relationships between demographic data (age, height, body mass, time since amputation, and residual limb length) and SAI.
Pearson’s correlation and partial correlation coefficients of age, height, body mass, time since amputation, and residual limb length.
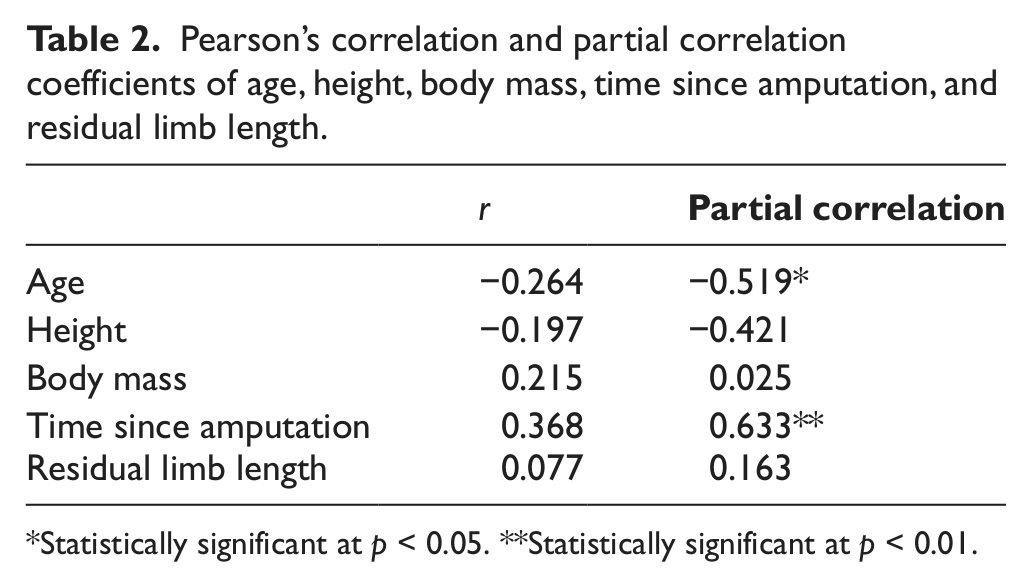
Statistically significant at p < 0.05. **Statistically significant at p < 0.01.
Table 2 also shows that the partial correlation coefficient of age (−0.519, p < 0.05) and time since amputation (0.633, p < 0.01) were significantly correlated with SAI. However, there were no significant correlations between height (−0.421), mass (0.025), or residual limb length (0.163) and the SAI.
Discussion
The purpose of this study was to investigate the factors affecting stair-ascent patterns in TFAs. We evaluated the stair-ascent pattern by assessing SAI, which was originally used to assess stair-descent pattern in TFAs by observing TFA’s gait pattern. In this study, we applied the SAI to stair ascent using telephone interview. To our knowledge, this is the first study that demonstrates the factors affecting stair-ascent patterns in TFAs. Although it did not reach statistical significance, Pearson’s correlation coefficients in age and time since amputation were slightly greater than other demographic data (Table 2). Specifically, the results of partial correlation revealed that age and time since amputation were significantly correlated with the SAI, respectively (Table 2). Thus, the present results support our initial hypothesis, which stated that SAI in TFAs would be correlated with both age and time since amputation.
The current results are in accordance with our previous study, 12 which reported that some TFAs could ascend stairs in a step-over-step pattern, the typical gait in normal subjects, without using a rail or other assistive device utilizing a unique form of compensatory intra- and interlimb coordination with a single-axis prosthetic knee joint. That study considered two TFAs who had had their leg amputated at quite a young age (time since amputation was 43 and 25 years in TFAs 1 and 2, respectively). Similarly, Puhalski et al. 22 reported that locomotor function is positively influenced by prosthetic wear time and the number of years since amputation, but is negatively influenced by age. Hence, this study as well as past findings suggests that both age and time since amputation are factors affecting stair-climbing patterns in unilateral TFAs.
It is somewhat surprising that there was no correlation between residual limb length and SAI (Table 2). This finding is contrary to our second hypothesis, which stated that SAI would be positively correlated with residual limb length. As mentioned above, our previous study reported that some TFAs could ascend stairs in a step-over-step pattern utilizing unique compensatory intra- and interlimb coordination. 12 In that study, residual limb length, which was thought to affect ambulatory ability in amputees, was different between the two subjects (Table 1 in that study). Furthermore, a previous finding has demonstrated that residual limb length does not significantly correlate with any spatiotemporal, kinematic, or kinetic gait parameters if the femur is at least 57% of the length of the contralateral femur. 25 So far, no study has yet investigated the relationship between residual limb length and stair ambulation in TFAs. However, our result shows that residual limb length does not affect SAI if the residual limb is at least 11 cm long (28% of contralateral thigh length, calculated from Plagenhoef et al. 26 ). Thus, this study suggests that residual limb length is not a limiting factor for stair climbing if the TFA has a certain level of residual limb length. Future studies should examine the relationships in this population between residual limb length and detailed gait parameters, such as kinematics, kinetics, and energetic efficiency.
In this study, stair-climbing patterns in unilateral TFAs were assessed by SAI. The arithmetic mean ± SD and median of SAI were 6.2 ± 3.4 and 5, respectively. These scores correspond with those of a previous study, where the mean score of SAI was approximately 5 (“Without rail or assistive device, step-to-pattern”) in TFAs.10,11 Indeed, Bae et al.7,8 reported that TFAs in their study have a gait pattern in which the foot of the prosthetic limb is pulled up only after the foot of the sound limb climbing the step is placed firmly on the step. Hence, this study and past findings suggest that our study population was representative, and the typical gait pattern during stair ascent in TFAs is the step-to-step pattern.
In this study, we investigated relationships between demographic data (age, height, body mass, time since amputation, and residual limb length) and SAI; however, additional independent variables may also relate to the SAI. One possible variable is the prosthetic knee unit and other prosthetic components (i.e. socket fitting, suspension, prosthetic foot, etc.). Past findings suggest that a nonmicroprocessor single-axis prosthetic knee joint could be a reasonable tool for TFAs during stair climbing, because it could give the patient more voluntary knee control.12,27 Another possible variable is the strength of the sound limb. Powers et al. 3 suggest that adequate force is necessary in both residual and sound limbs to improve functional gait ability in below-the-knee amputees. Although we did not determine functional level of the TFAs in this study, this level might influence the SAI. Furthermore, as suggested by Zidarov et al., 28 stair-climbing patterns may be more related to pain sensation and psychosocial well-being (adaptation to amputation and body image) than to clinical or demographic variables such as age, sex, and level or cause of amputation. Using these factors, deeper explanations of the determinants of stair-climbing patterns in TFAs might be possible.
Limitations
There are several limitations to consider when interpreting these findings. First, as previous studies described, SAI is an outcome measure for stair-descent pattern by asking the participants to walk a 12-step, Americans with Disabilities Act–compliant stairwell.10,11,21 In this study, we applied the SAI to stair ascent by the telephone interview. The method involves subjectivity in subject responses; however, several studies reported that the use of telephone interviews with individual lower extremity amputations is a valid method of obtaining functional outcome measurements.22,29 –32 Second, stair-climbing training was not controlled and the rehabilitation training could affect the SAI outcome. Further research is needed to identify the effects of training on stair-ascent pattern in TFAs. Finally, we investigated the relationship between SAI in stair ascent and demographic data in TFAs. However, the SAI is generally used for assessing stair-descent pattern.10,11,21 Therefore, factors affecting stair-descent patterns in this population should be examined in future research.
Conclusion
The results of this study suggest that both age and time since amputation are predictors of SAI in TFAs. On the other hand, residual limb length did not correlate with SAI, indicating that residual limb length is not a limiting factor for stair climbing, assuming a certain level of residual limb length. Clearly, additional work is necessary to fully determine the mechanisms responsible for the step-over-step stair-ascent pattern in TFAs.
Footnotes
Conflict of interest
None of the authors have any conflict of interest associated with this study.
Funding
This study was supported by Grant-in-Aid for JSPS Fellows.