
Abstract
Background and Aim:
The fitting of short finger stumps with silicone prosthesis is a challenge because of the suboptimal finger–prosthesis contact due to length and distal tapering of digital stumps. The purpose of this report was to describe and evaluate the Micropore™–polyvinyl chloride tube technique for fitting short finger stumps.
Technique:
For a total of 10 patients, short finger stumps were fitted using the technique. A short length of polyvinyl chloride tube, trimmed and contoured to fit, was secured on the distal stump tip with Micropore tape. The prosthesis was worn over the polyvinyl chloride tube extension. Three different fitting methods were evaluated: fitting with and without the Micropore–polyvinyl chloride tube technique, and with the use of skin adhesive on the stump.
Discussion:
All patients achieved a very secure prosthetic fit with the Micropore–polyvinyl chloride tube technique. No incidences of prosthesis slippage were reported at the longest follow-up of 30 months. The Micropore–polyvinyl chloride tube technique is an effective method for fitting short finger stumps.
Clinical relevance
The Micropore–polyvinyl chloride tube technique presents a nonsurgical method for fitting short finger stumps. It can help avert late outcomes whereby patients, after having undergone surgery to enable fitting, found they no longer need prosthesis.
Background and aim
A traumatic finger amputation is an unfortunate life event not only because of the functional disability it causes but also because of its disfiguring consequences. The sense of stigmatization associated with a missing digit can lead to damaged body image, and this can be detrimental to the psychosocial well-being of the patient.1,2 The fitting of esthetic silicone prostheses can play a useful role in mitigating the adverse impact of digital loss for patients who are concerned about the appearance of their hand.3 –5
Apart from a stump that is well healed and free of edema, an important prerequisite for fitting silicone prosthesis is adequate stump length. A minimum residual length of 15 mm—from the interdigital web to the distal tip—is needed for a secure fit of the prosthesis, which is held on the stump via vacuum “suction-cup” effect. 6 Short stumps that are also tapered add to the difficulty of fitting. In such cases, an interdigital web deepening or for selected cases, digital stump lengthening 5 are options that can be considered for increasing digital length. More radical procedures have included osseointegrated implants. However, it is not uncommon for patients to shun such surgical procedures because of concerns over tissue scarring, long-term complications, longer rehabilitation time, and added associated costs. Long-term prosthesis utilization studies have also shown that a fifth of patients who were fitted may no longer be wearing their prosthesis after the initial years.5 –7 In view of the attrition, a nonsurgical approach to fitting short finger stumps is preferred, keeping in mind that the consequences of surgery are permanent, but prosthesis use may be temporary.
The authors have developed a novel nonsurgical method for fitting short finger stumps, the Micropore™–polyvinyl chloride (PVC) tube fitting technique, for this purpose. In this article, we describe the technique and our evaluation of its effectiveness in achieving a secure prosthetic fit in patients with very short finger stumps.
Methods
Patient profile
Between October 2009 and July 2012, 10 patients presented at our hospital’s prosthetic clinic with very short finger stumps with residual length less than the 15 mm required for fitting silicone prostheses. The profile of each patient and their stump characteristics and length of follow-up postfitting are summarized in Table 1. All cases were the result of trauma, except for a 16-year-old female student with bilateral constriction band syndrome (patient no. 5) who had corrective surgery at the age of 1 year, but whose right middle finger stump (Figure 2(b)) was still too short for prosthetic fitting. All patients had requested finger prostheses to improve the overall appearance of their hand but did not want surgical intervention to enable fitting on their short finger stumps.
Summary of patient profile, stump characteristics, and length of follow-up.
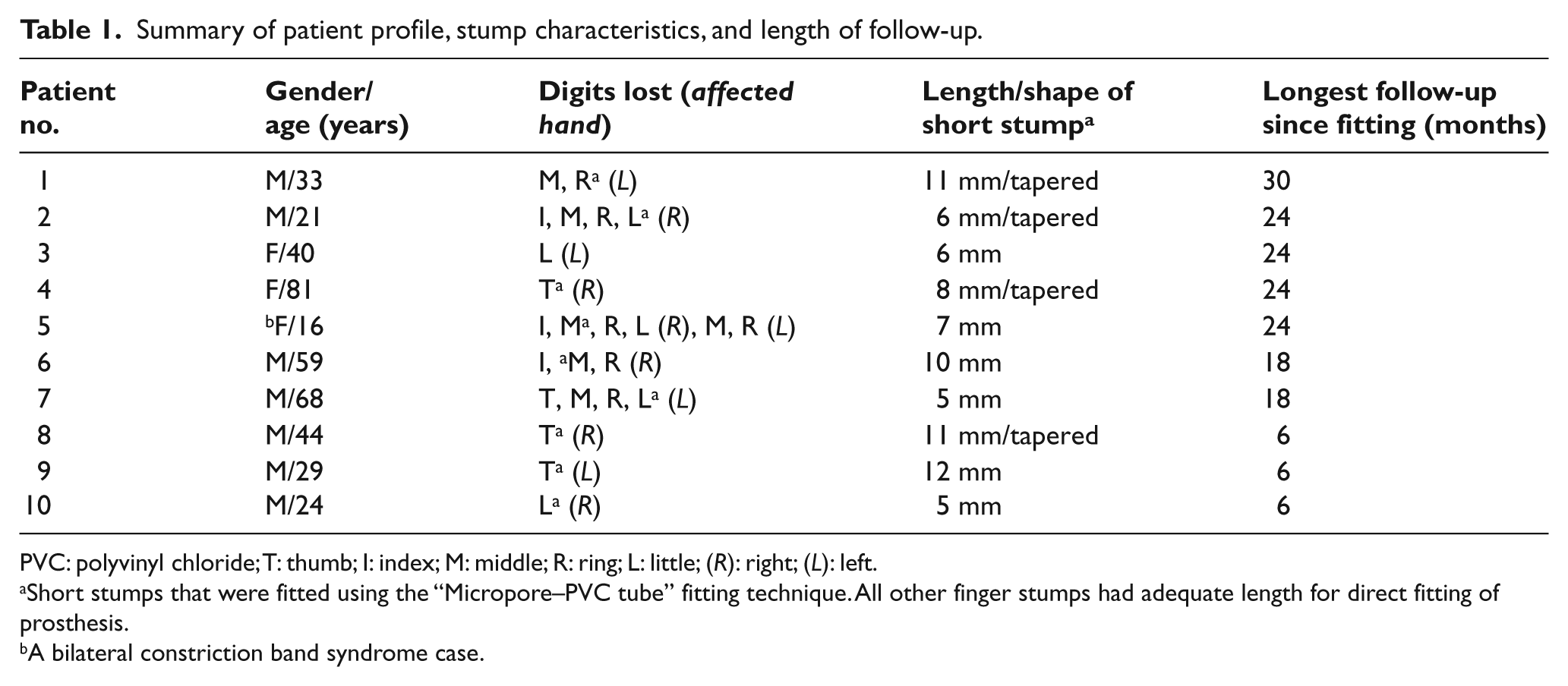
PVC: polyvinyl chloride; T: thumb; I: index; M: middle; R: ring; L: little; (R): right; (L): left.
Short stumps that were fitted using the “Micropore–PVC tube” fitting technique. All other finger stumps had adequate length for direct fitting of prosthesis.
A bilateral constriction band syndrome case.
The Micropore–PVC tube fitting technique
For each short stump that was fitted using the method, a rigid PVC tube (HomeFix Ltd, Singapore) of matching circumferential size was procured. A short length of the tube (2 cm) was cut out for fitting on the stump as a “length extension.” The proximal cut edges were trimmed to a matching contour to fit snugly over the distal stump without causing any impingement. The PVC tube was tapered distally to replicate the shape of the finger. All cut edges were smoothed out using a fine-grade sand paper, and the finished tube was secured firmly on the finger stump using a skin-colored strip of Micropore tape (3M, Minnesota, USA) as shown in Figures 1(a) and 2(b). Two layers of Micropore tape was applied such that enough width of it tapes over and around the stump (skin) and the PVC tube to ensure a secure fixation. The prosthesis was then worn over the PVC tube extension to cover it and any visible Micropore tape completely (Figures 1(b) and 2(c)).
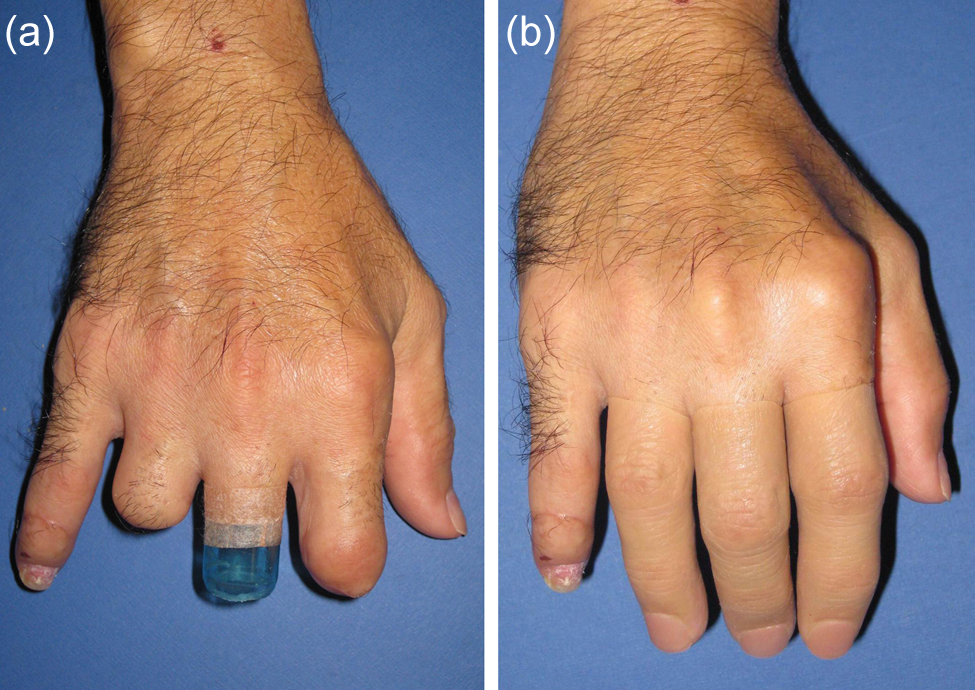
(a) Patient (no. 6, Table 1) with multiple-digit amputation. The Micropore–PVC tube fitting technique was applied on the middle stump, which was too short for fitting a prosthesis. The tube was taped and secured firmly on the stump using 3M Micropore tape. (b) After fitting with prostheses.

(a) Bilateral congenital case (patient no. 5) with malformed right index, middle, ring, and little digits, and left middle finger and ring fingers, (b) application of the Micropore–PVC tube fitting technique on the right middle finger stump, and (c) after fitting with prostheses.
PVC tube, manufactured in varying diameters, is easy to cut and soften with a heat gun for reforming to match different finger shapes and sizes. Micropore tape is hypoallergenic, adheres well to skin and PVC surfaces, yet leaves no sticky residues on the finger stump. Its thin and translucent appearance blends well with the surrounding skin and makes it an excellent tape to be used with this technique.
Evaluation of prosthetic fit
Patient evaluation of the prosthetic fit was conducted during final fitting when the prosthesis was supplied to the patient. Three different methods of fixation as follows were evaluated in succession to determine which gives a more secure fit:
The prosthesis was fitted directly on the bare stump without the use of skin adhesive.
The prosthesis was fitted after a thin coat of Pros-Aide skin adhesive (A.D.M. Tronics Inc, NJ, USA), which is used widely for the fixation of maxillofacial prostheses, was applied on the stump to augment fixation.
The prosthesis was fitted using the Micropore–PVC tube fitting technique.
With the prosthesis properly donned, the patient was instructed to perform a gentle flick of the hand to attempt to dislodge it from the stump. In a nonevent, evaluation was proceeded with a third person (a colleague who is not involved in the study) applying an outward pulling force, referred to as a tug, on the prosthesis in a further attempt to dislodge it. When prosthesis fixation is secure, an incipient slippage would give rise to a vacuum suction effect on the stump (palpable to patient) that checks further movement. A scoring system designed by the authors was used to evaluate prosthetic fit. The patient was asked to evaluate the prosthetic fit by giving a score to indicate how secure he felt the prosthetic fit was. A score of “0” was recorded when the patient felt no suction-cup effect, with the prosthesis easily slipping off the finger stump with a gentle flick of the hand. A score of “1” was recorded when fairly good suction effect was achieved, with the prosthesis remaining on the finger stump when a light tug was applied, but slipping off with a heavier tug. A score of “2” was given when a strong suction effect was achieved, with the prosthesis remaining firmly secure on the finger stump when a heavy tug was applied.
Postfitting stump/prosthesis care and monitoring
Follow-up review was done every 6 months. Patients were instructed to monitor their finger stump for any signs of skin problems from extended hours of application of the PVC tube and Micropore and to return for adjustments should they encounter any pain from the PVC tube impinging on their stump.
To prolong the life span of the prosthesis, all patients were advised to use Vaseline™ as lubricant to ease donning, which minimizes wear and tear forces, and to regularly clean its internal surfaces with 70% alcohol to prevent accumulation of sweat/Vaseline residues that can lead to fungal growth. They were advised not to wear their prostheses when they are at home so as to avoid undue stress to their skin.
Results
All patients had a more secure prosthetic fit using the Micropore–PVC tube technique compared with fitting using skin adhesive, with their prosthetic fit score improving from 0 or 1 to 2 (Table 2). The use of skin adhesive resulted in a better fit in all cases compared with direct fitting on the bare stump except for two patients (Nos. 7 and 10) who had very short stumps of 5 mm. Both patients found no appreciable improvement in prosthetic fit with the use of skin adhesive. Three patients (Nos. 1, 6, and 9; Table 1) who had initial prosthetic fit score of “1” had improved fit with skin adhesive, but fixation was still not secure enough to be accorded the score of “2.” They had the lowest shortfall in stump length from the minimum of 15 mm needed for a secure fit compared to the other patients for whom prosthetic fit with direct fitting had a score of “0.”
Evaluation of prosthetic fit.
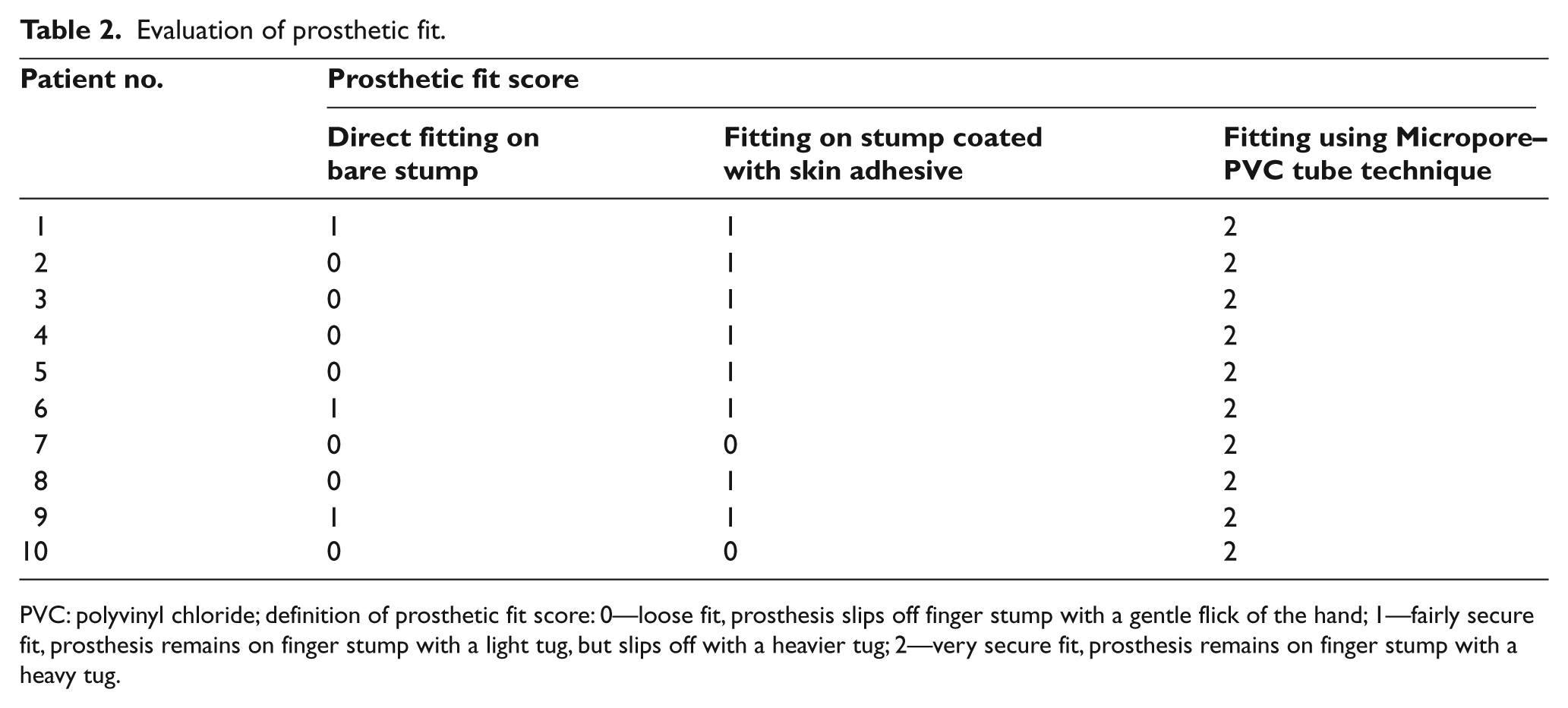
PVC: polyvinyl chloride; definition of prosthetic fit score: 0—loose fit, prosthesis slips off finger stump with a gentle flick of the hand; 1—fairly secure fit, prosthesis remains on finger stump with a light tug, but slips off with a heavier tug; 2—very secure fit, prosthesis remains on finger stump with a heavy tug.
At follow-up time ranging from 6 to 30 months (Table 1), none of the 10 patients reported any incidence of prosthesis slippage, stump discomfort/pain, or skin maceration from using the Micropore–PVC tube technique. The reported frequency of prosthesis utilization among the patients ranged from 4–8 h daily. All patients found the method easy to use and were able to apply the PVC tube and the Micropore tape on their finger stump on their own.
Discussion
A challenge confronting fitting finger short stumps with silicone prosthesis is to achieve a secure fit despite the residual length constraint. This is compounded by the tendency of short stumps to taper in shape from late tissue shrinkage and the fact that a suction-fitted silicone prosthesis acts very much like a pressure garment and, when worn for a protracted period, can shrink the finger stump via soft tissue compression. 8
Proprietary skin adhesive manufactured for maxillofacial prostheses application has been shown in this evaluation to be unsatisfactory in aiding prosthetic fixation when used on very short and tapered finger stumps. The layer of adhesive residues left on the skin was also troublesome to remove and posed a problem for four patients in our series who had sensitive stumps. When secure prosthetic fixation cannot be achieved with vacuum suction effect and skin adhesives, the usual recourse for patients who are still keen to have prosthesis is to have the stump surgically lengthened, with the attendant disadvantages of tissue scarring, prolonged recovery time and added cost. Osseointegration has also been offered at a small number of centers as a stable method of fixation with better prospects for tactile sensation. 9 However, besides cost escalation, lingering concerns about potential late complications, including loosening of the implant, implant fractures and infection at the implant–skin interface needs to be more adequately addressed. Nonsurgical approaches involving the double or buddy ring method of fixation have been used. 10 However, the method is cumbersome to apply because of the rigidity inherent in the soldered rings. A related limitation of the method is compromised stability of prosthetic fit in the face of repeated flexion-extension mobilization of the uninjured anchoring digit. The method also cannot be used when both adjacent fingers are similarly affected.
The Micropore–PVC tube fitting technique has been demonstrated to be a simple and yet effective nonsurgical approach to fitting very short and tapered stumps. A secure prosthetic fit can be achieved without the encumbrances of elaborate buddy rings, skin adhesives, and the need for surgical intervention. It presents a welcome option for patients who want a prosthesis primarily for esthetic reasons but are averse to undergoing further surgical procedures to enable a fitting on their short finger stumps. Patients found the simplicity of the method an advantage. They understood how a secure prosthetic fit is achieved and were able to independently apply it on their own. They also appreciated that because both materials used in the technique—Micropore and PVC tube—are low-cost items that are readily available, the option can be offered to them at no extra cost. Secure fixation of the PVC tube, and therefore, the prosthesis, is via the good adhesion to skin and strength of the Micropore tape. A wider strip taping over more skin and additional layers may be used to augment fixation if required. Candidates suitable for the Micropore–PVC tube fitting technique should have adequate stump protuberance (5 mm from interdigital web) and with healthy skin.
It remains a challenge to accurately assess patients’ expectations, acceptance and utilization of their prostheses over a long term. Some patients may, as time passes, simply come to terms with their physical loss and subsequently do as well without prostheses. The Micropore–PVC tube fitting technique presents a useful option that can help avert late outcomes whereby patients, after having undergone surgical revision of their stump to enable fitting, found they were fine without a prosthesis after all. For patients without prior experience with prosthesis use, a nonsurgical approach to fitting short finger stumps using this technique can be used as a first option. Patients who had demonstrated to be long-term prosthesis users can later make a better “informed” decision on more invasive methods of fixation, should they find it to be necessary.
Key points
Short finger stumps present a challenge in terms of fitting with silicone prosthesis because of the suboptimal finger–prosthesis contact due to length and distal tapering of digital stumps. The usual recourse is surgical intervention to lengthen the finger stump.
Three different fitting methods were evaluated: fitting with and without the Micropore–PVC tube technique, and with use of skin adhesive on the stump.
Fitting with Micropore–PVC tube technique was demonstrated to be able to achieve the most secure of prosthetic fit.
All patients achieved a very secure prosthetic fit with the Micropore–PVC tube technique, with no reported incidences of prosthesis slippage at the longest follow-up of 30 months.
Where possible, a nonsurgical approach such as the Micropore–PVC tube fitting technique should first be attempted when fitting short finger stumps, as it can help avert late outcomes whereby patients, after having undergone surgery to enable fitting, found they no longer need to wear a prosthesis.
Footnotes
Conflict of interest
The authors hereby declare that there is no conflict of interest. Due to the nature of this study, no bioethical approval is required and therefore was not sought.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.