
Abstract
This study addresses the dilemma of initial clinical and social acceptance of a newly fabricated silicone prosthesis in relation to its colour match to the natural skin. This was achieved by derivation of specific colour difference thresholds defining perceptible and acceptable levels of colour sensitivity. Two separate sets of 10 fair and dark shade digit prosthesis samples were each fabricated with a stepped increase in colour difference (ΔE) against the baseline hand prosthesis. Ninety individuals with normal colour vision scores were selected as colour assessors. The colour difference of each prosthesis in the two series was evaluated visually against the baseline by the assessors, using defined scores. The thresholds for perceptible and acceptable colour difference determined in this study were ΔE = 0.8 and ΔE = 1.8 for the fair series and ΔE = 1.3 and ΔE = 2.6 for the dark series, respectively. The acceptable threshold values differed from the perceptible threshold values by ΔE = 1.0 for the fair-shade samples and ΔE = 1.3 for the dark-shade samples. This study demonstrated that subjective visual assessment is positively correlated with ΔE values computed from colorimetric measurements for both fair and dark-shade silicone samples (p<0.001). This results shows that human subjects with normal colour vision are capable of accurately assessing colour differences. These observations emphasize the importance of subjective feedback on colour by the patient, provided the latter has perfect colour-tested vision. The study also showed that human subjects were less sensitive to perceived colour differences in darker-shade than fairer-shade samples (p<0.001). This finding seems relevant in a clinical setting involving a multi-ethnic patient population.
Introduction
Aesthetic silicone prostheses have been shown to play a useful role in restoring normal appearance and assist in the rehabilitation of patients with amputations involving the upper limbs (Pillet 1983; Alison and Mackinnon 1992; Beasley 1987; Campbell et al. 1992; Pereira et al. 1996; Leow et al. 2001).
Initial acceptance of these prostheses may rely on colour assessment by the clinician-prosthetist, the patient and his/her peers. Available thresholds for acceptable colour differences were limited to translucent rigid dental materials, fabrics, paints and dyes, but not for application in hand prosthetics (Ruyter et al. 1987; Seghi et al. 1989; Guan and Luo, 1999). In the absence of an established clinical colour benchmark for silicone prostheses, accurate colour simulation of the natural skin presents a constant dilemma to the clinical prosthetist.
Information as to whether human subjects vary in the visual perception of colour difference within either fair-shade or dark-shade prostheses has not been fully investigated. This may be of value in a multi-ethnic patient population.
The aims of this study were to determine: i) the thresholds for perceptible and acceptable colour differences for silicone hand and digit prostheses; and ii) if there were variations in subjective assessments of colour difference in dark and fair shade prostheses.
Materials and methods
Colour measurement using the CIE (L∗a∗b∗) colour system
The colour attributes of all the prosthesis samples in this study were measured in terms of Commission Internationale de l'Eclairage CIE (L∗a∗b∗) values using a colorimeter (Chroma Meter CR-300, Minolta, Tokyo, Japan). The “L∗” measurement gives the value (lightness) of the colour with L∗ = 100 representing purest white and L∗ = 0 representing deepest black. A colour measurement in the “+a∗” direction indicates a shift towards red, a “–a∗” measurement gives a colour towards green, a “+b∗” measurement gives a colour towards the yellow end and a measurement in the “–b∗” end gives a colour towards blue.
Fabrication of fair-shade baseline hand prosthesis
A baseline hand prosthesis colour-matched to a fair-skin shade (with high basic yellow pigment content) and designated as fair-shade hand prosthesis was fabricated using a negative mould made from an epoxy model (Figure 1). Oil-based colour pigments (Cosmesil™, Principality Medical Ltd., South Wales, UK) were used with a medical grade silicone rubber (Cosmesil™, Principality Medical Ltd., South Wales, UK) to produce the prosthesis. The prosthesis was moulded in double layers of silicone rubber—a translucent outer layer and an opaque inner layer—and incorporating an intermediate layer of detailed touch-up colouration, such that its final colouration was the resultant colour of 3 laminated layers. The methodology for moulding multilayered prostheses has previously been reported (Leow et al. 1997; Pereira et al. 2001). The thickness of the inner and outer layer of the prosthesis was maintained at 0.45 ± 0.01 by controlling the silicone-solvent ratio.

Picture showing the 2 series of digit prosthesis samples. The first series consisted of a set of 10 fair-shade digit prostheses with increasing ΔE values against the baseline hand prosthesis. The second series also consisted of 10 dark-shade digit prostheses matched against a dark-shade baseline and with respectively comparable ΔE values to the first series.
A defect was created in the completed hand prosthesis cutting off the “middle digit” near the web space. The digit so “severed” was designated as Prosthesis-Fair-0 and served as a control. The hollow prosthesis was fitted with an inner core of clear silicone with a 2 cm stump-shape protrusion through the residual cut digit to act as digital stump, onto which prosthesis samples are donned for visual assessment.
Fabrication of fair-shade digit prosthesis samples with incremental stepped colour difference
A set of 10 fair-shade digit prosthesis samples, designated Prosthesis-Fair-1 to -10 (Figure 1), with identical layered design, was fabricated using identical negative moulds of the severed middle digit of the baseline hand prosthesis. These digit prostheses acted as replacement for the “severed” digit on the fair-shade hand prosthesis and were later donned and visually assessed for colour difference against the baseline. They were colour-matched to a graduated increase in colour difference against the baseline prosthesis by 0.5 increments in ΔE values (Table I).
L∗, a∗, b∗ values of the inner layers, and of the fair-shade & dark-shade digit prosthesis samples and their ΔE values against the baseline hand prosthesis.
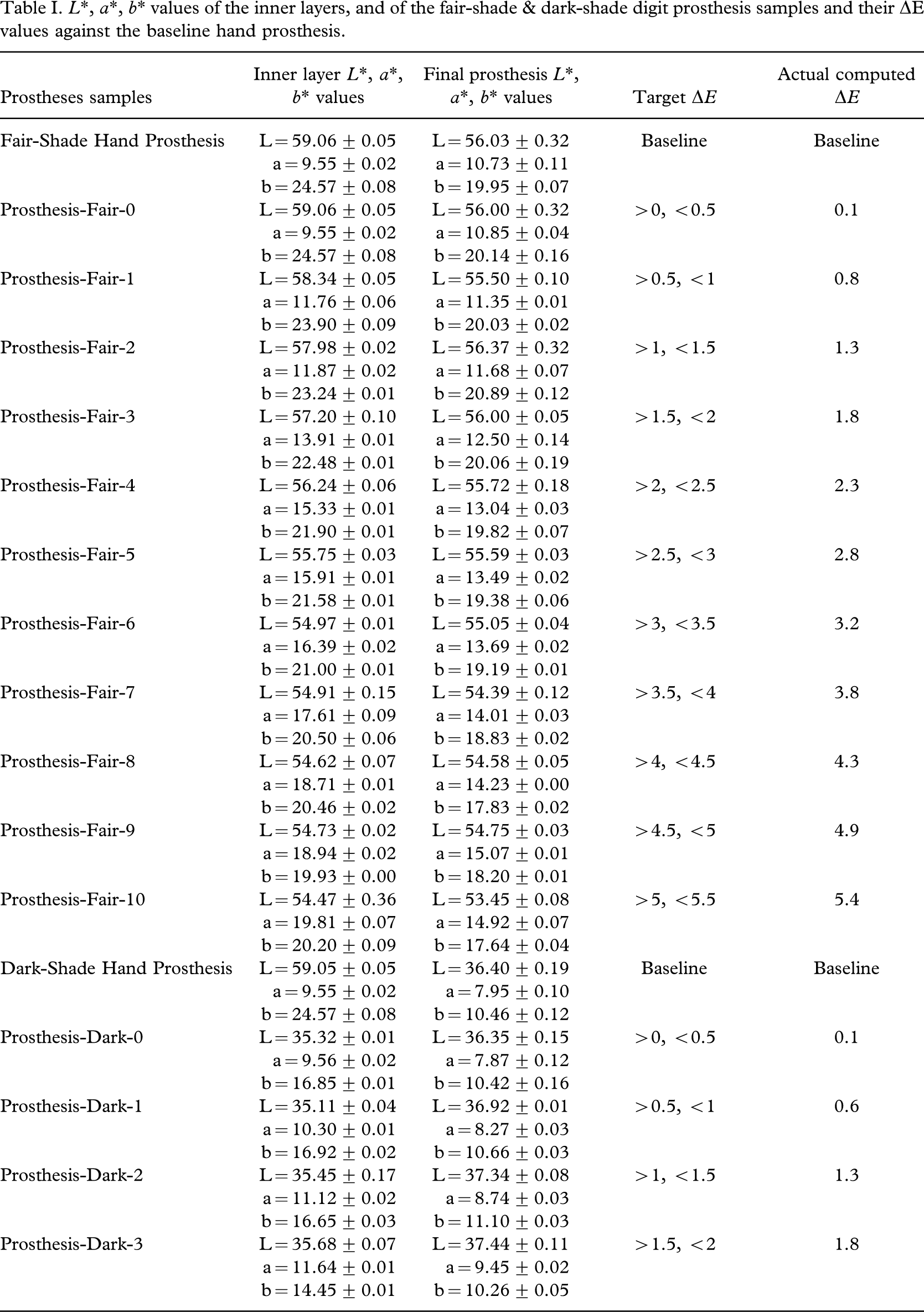
The same pigment formulation for the translucent outer layer (L∗ = 63.19 ± 0.04, a∗ = 15.63 ± 0.01, b∗ = 26.17 ± 0.02) used for the Fair-Shade Hand Prosthesis was used to produce the fair-shade digit prosthesis samples.
The same pigment formulation for the translucent outer layer (L = 52.24 ± 0.16, a = 13.21 ± 0.05, b = 20.67 ± 0.02) used for the Dark-Shade Hand Prosthesis was used to produce the dark-shade digit prosthesis samples.
The same translucent outer layer (L∗ = 63.19 ± 0.04, a∗ = 15.6 ± 0.01, b∗ = 26.17 ± 0.02) for colour-matching the baseline prosthesis was used to produce the digit samples. Only the opaque inner layer was varied in pigment formulation for these samples to achieve a colour difference from the baseline shade. Trial and error was used to achieve the target range of ΔE (colour difference) as shown in Table I. The actual computed ΔE values achieved were close to the targeted values. The main author's (MLEL) clinical experience with colour-matching prostheses, coupled with the method of stepped increase in the number of drops of specific pigments from the baseline formulation, reduced the number of trials needed to achieve the target ΔE values.
Fabrication of dark-shade baseline hand prosthesis and replacement dark-shade digit prosthesis samples
Similarly, a dark-shade hand prosthesis (with high master brown pigment content), designated as dark-shade hand prosthesis, and a set of 10 dark-shade digit prosthesis samples designated as Prosthesis-Dark-1 to -10 ( Figure 1), and each having closely comparable colour difference (ΔE) to corresponding digit samples in the fair series was fabricated using the same described procedures (Table I).The same translucent outer layer (L = 52.24 ± 0.16, a = 13.21 ± 0.05, b = 20.67±0.02) for colour-matching the dark-shade baseline was used to produce the digit samples.
Computation of colour difference
A colour difference (ΔE) between a given digit prosthesis sample and its respective baseline hand prosthesis was calculated using the following colour difference equation (Wypych, 1995;
Beatty et al. 1995; Leow et al. 1997, 1999):

where ΔL∗, Δa∗, and Δb∗ are the differences in the L∗, a∗, and b∗ values between the digit prosthesis and the baseline shade.
L∗, a∗, and b∗, and ΔE (colour difference) values of completed prosthesis samples
The L∗, a∗, and b∗ values of all the completed prosthesis samples, and of their inner and outer layer (measured separately) are as shown in Table I. The actual computed ΔE (colour difference) for each sample in the fair series (Prosthesis-Fair-1 to -10) and the dark series (Prosthesis-Dark-1 to -10) against their respective baseline is also shown therein.
Colour vision deficiency screening of assessors
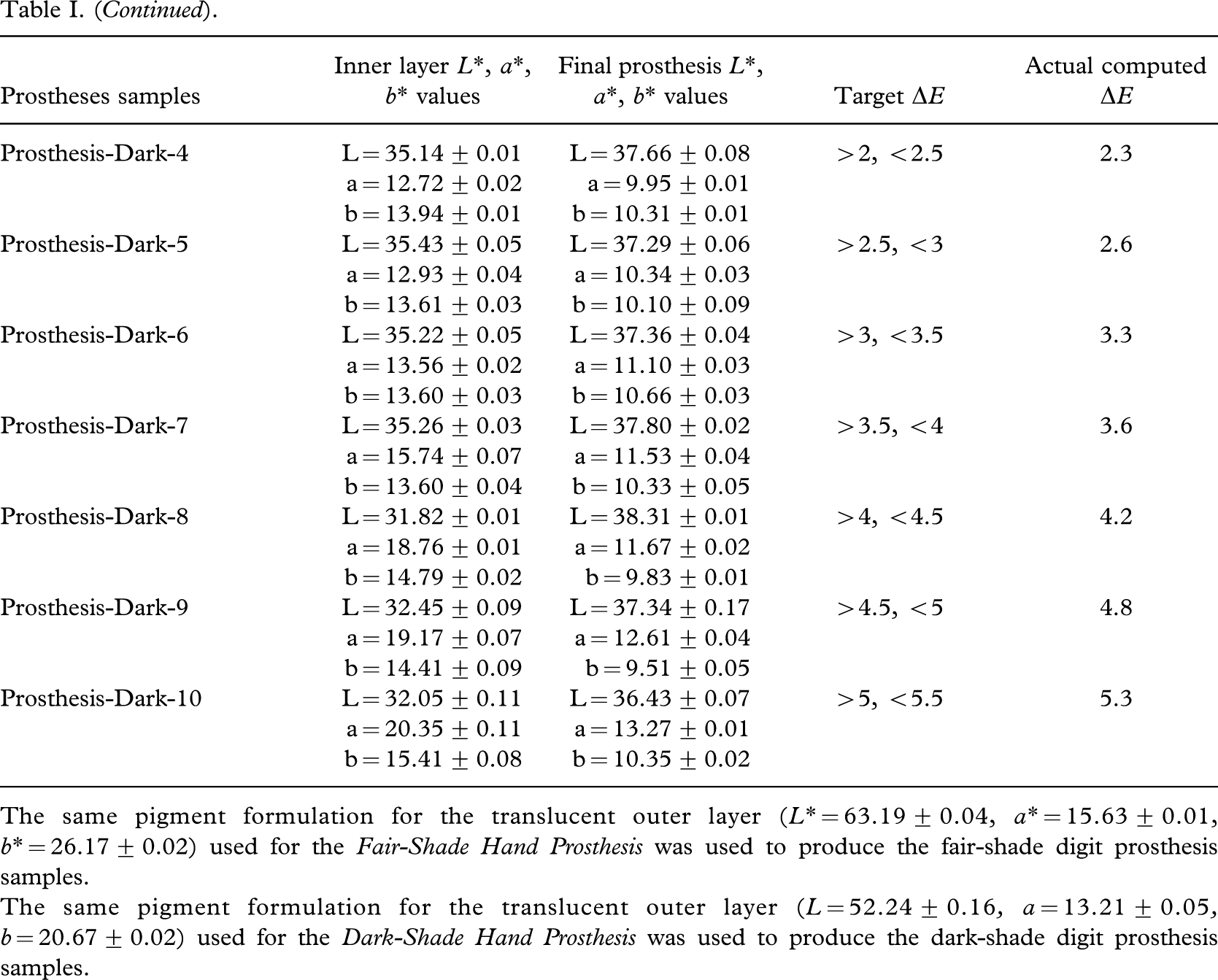
The Farnsworth-Lanthony's Desaturated 15 Hues Test was administered to screen all prospective assessors for any colour vision deficiency. The test consists of 15 colour chips with subtle differences in shades and an additional fixed standard reference chip (Figure 2). The chips are to be randomized and rearranged by a prospective assessor in the correct sequence that conforms to a blue-to-green, yellow-to-orange and pink-to-purple colour scheme. Only those who accomplished the test with a full score were included in the visual assessment of the prosthesis samples. The eye-screening test was conducted under standard D65 light source, within a commercial colour assessment cabinet (Verivide, Leslie Hubbell Ltd., UK) (Figure 2).
The Farnsworth-Lanthony's Desaturated 15 Hues Test set, comprising of 15 colour chips. The screening test was carried out under standard D65 light source within a commercial colour assessment cabinet (Verivide, Leslie Hubbell Ltd., UK).
A total of 93 subjects were administered the Farnsworth-Lanthony's Desaturated 15 Hues Test. All but 3 subjects attained a full score and proceeded on to the visual assessment segment of the study. The 90 assessors consisted of 48 males (53.3%) and 42 females (46.7%). In terms of ethnic proportions, there were 77 Chinese (85.6%), 4 Malays (4.4%) and 9 Indians (10%). The assessors were grouped according to 4 age groups as follows: 15 – 25 years (31.1%); 26 – 35 years (37.8%); 36 – 45 years (24.4%); and 46 – 55 years (6.7%).
Visual and colour difference assessment
Each of the 10 fair-shade digit prosthesis samples was randomly taken and donned on the respective fair-shade baseline for visual assessment of colour difference. A score sheet using a scoring system defined as follows was used to score colour difference (Appendix):
3—same colour;
2—different but acceptable;
1—different and unacceptable.
Each assessor was assigned a score sheet. The assessor assigned a score for each digit prosthesis sample, corresponding to how he thought its colour differed from the baseline. The control digit sample, Prosthesis-Fair-0, was also randomized and assessed. The visual assessment of the prosthesis samples was also conducted under standard D65 light source within the same colour assessment cabinet. Visual assessment was repeated for each prosthesis sample in the dark series.
Data analysis
Statistical analyses were performed using SPSS 12.0 with statistical significance set at p<0.05. Descriptive statistics for the responses were presented using bar charts supplemented with frequency counts and percentages. To establish the threshold for “perceptible colour difference” within each colour shade, McNemar test for paired samples were performed comparing each prosthesis with the respective baseline using the full range of the scoring system (1 to 3). For the threshold of “acceptable colour difference”, the favourable score of “2” (acceptable) and “3” (same colour) were combined.
To determine whether there was a significant difference in how subjects view colour difference between dark and fair shade prosthesis samples, McNemar tests were performed on prosthesis-sample-wise for both perceptible and acceptable colour difference. Chi-square Goodness-of-fit test was performed to assess the distribution of frequencies against the assumption of equal probability for subjects' sensitivity to colour differences between the two shades. The association between gender, age group and ethnicity and their bearing on the visual thresholds for colour difference was assessed using Chi-square/Fisher's exact test.
Results
Visual assessment of colour difference within each colour shade
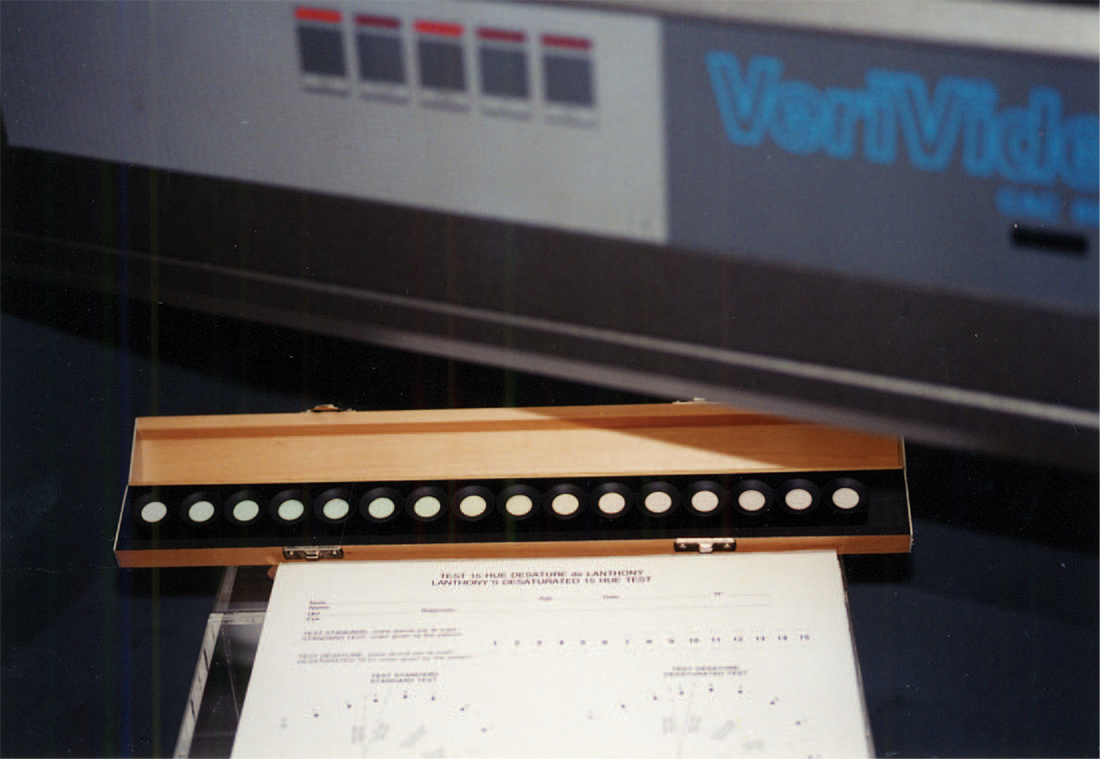
The results of the visual assessment are represented in Figure 3, which shows the percentage of assessors with the different scores against the prosthesis samples. The prosthesis sample beyond which an incipient colour difference began to be perceived was Prosthesis-Fair-1 (for the fair series) and Prosthesis-Dark-2 (for the dark series) (Figure 3). The corresponding threshold for perceptible colour difference was (Table I):
ΔE = 0.8 (for the fair series)
ΔE = 1.3 (for the dark series)
0.8 (for the fair series) ΔE:
1.3 (for the dark series)
The sample prosthesis beyond which colour difference was unacceptable was Prosthesis-Fair-3 (for the fair series) and Prosthesis-Dark-5 (for the dark series). The corresponding threshold for acceptable colour difference was determined as follows (Table I):
ΔE:
1.8 (for fair-shade prosthesis) ΔE: 2.6 (for dark-shade prosthesis)
Summary of visual assessment: percentage of assessors with the different scores against the prosthesis samples, fair versus dark series.
Fair- and dark-shade prosthesis samples
Perceptible and acceptable colour difference
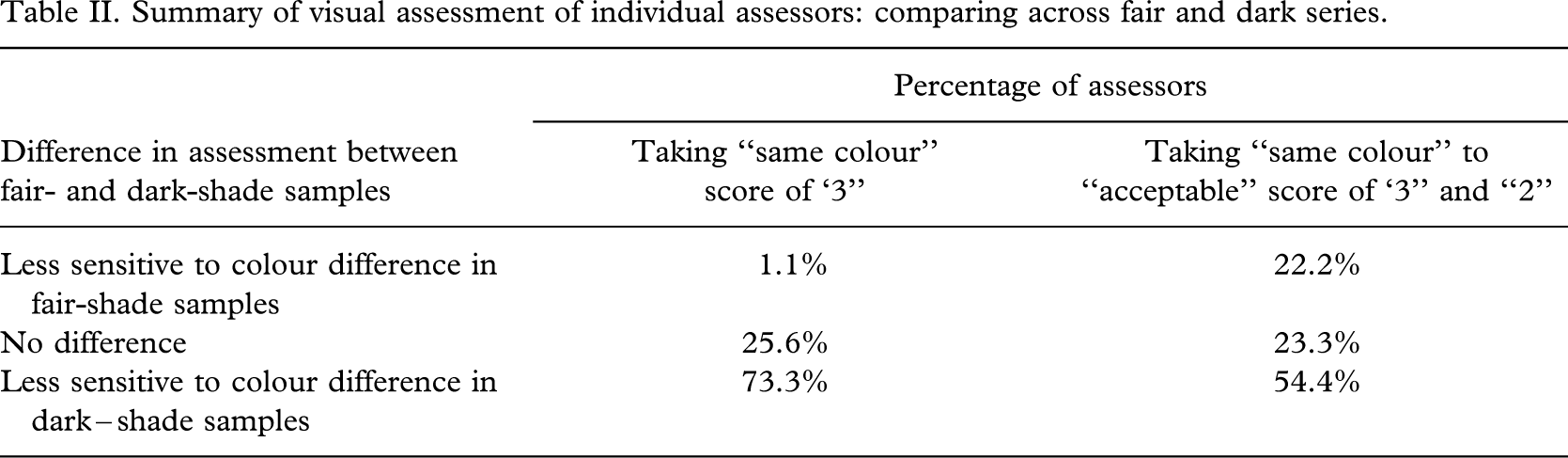
The results of this study demonstrated that the assessors were less sensitive to incipient colour difference (ΔE) in darker-shade than fairer-shade samples (Table II). Comparing across the fair and dark series for each individual, it was found that a significantly higher number of assessors assigned the “perceptible” and “acceptable” to darker-shade samples (73.3% and 54.4%) having larger ΔE values than fairer-shade samples (1.1% and 22.2%) (Goodness of fit test with equal proportions, p<0.001). When the factors of gender, age and ethnicity were considered, there were no significant differences (p > 0.05) in how the assessors perceived colour differences in the prostheses. This preliminary data on gender, age and ethnicity of the assessors have not indicated that these factors had significantly influenced their sensitivity to prosthetic colour assessment. The Farnsworth-Lanthony's Desaturated 15 Hues Test has also confirmed that the selected assessors all had perfect colour vision.
Summary of visual assessment of individual assessors: comparing across fair and dark series.
Discussion
One of the objectives of this study was to address the need to define a colour difference threshold, which depicts initial acceptance of newly fabricated silicone prosthesis. The thresholds of perceptibility or acceptability defined relate to this initial phase of assessment. The defined thresholds were derived from assessments of newly fabricated digit and hand prostheses, which were not subject to weathering agents. The basic pigment composition of the prosthesis samples had attempted to simulate the vascular appearance of the skin of the hand and digits in a neutral posture, that is, neither in a raised nor lowered position, relative to the horizontally placed forearm. The study was designed to exclude extraneous factors such as sun-tanning effects on the natural skin and colour deterioration in the prosthetic samples from exposure to ultra-violet (UV) light and stump perspiration (Leow et al. 2002). Viewing conditions was also standardised to the colorimetric light source of D65 to exclude the influence of metameric colour differences on the results (Leow et al. 1999).
Method error
A small ΔE error of 0.1 against the respective baseline prosthesis was recorded for both the control samples Prosthesis-Fair-0 and Prosthesis-Dark-0. This minor colour difference is attributed to fine differences in pigment homogeneity within each sample that were recorded by the highly sensitive colorimeter (Leow et al. 2002). The minute colour difference was not perceived in the visual assessment, with all the assessors consistently assigning the “same colour” score of “3” for both control samples (Figure 3).
Based on current literature, the human eye is able to detect or perceive a colour difference between two juxtaposed objects only when the ΔE value between them is greater than 1 unit (Wypych 1995; Beatty et al. 1995; Leow et al. 2002). This is referred to as visually perceptible colour difference. The perceptible thresholds of ΔE = 0.8 for fair series and ΔE = 1.3 for dark series (Figure 3, Table I) derived in this study were largely in agreement with the established perceptible threshold of ΔE = 1 unit. The results seem to corroborate the validity of the methods used in this study.
Acceptable colour difference
The perceptible threshold marks the beginning of an incipient colour difference (ΔE values), which increases to a point referred to as the acceptable threshold, beyond which the perceived colour difference becomes unacceptable to the assessor. In clinical situations, a prosthesis having a perceived colour difference when compared with adjoining skin may be still be regarded as satisfactory by the patient, provided the difference is within his “acceptable” threshold. In this study involving soft silicone materials, the acceptable threshold was determined to be ΔE = 1.8 for the fair-shade prosthesis samples and ΔE = 2.6 for the dark-shade prosthesis samples (Figure 3, Table I).
The acceptable threshold values determined in this study differed from the perceptible values by ΔE = 1.0 for the fair-shade samples and ΔE = 1.3 for the dark-shade samples.
Fair- and dark-shade prosthesis samples
The essential difference between the fair- and dark-shade prosthesis samples lies in their pigment composition. A higher concentration of brown pigments was used in the darker-shade prostheses to mimic the increase in melanin pigment density with the change from a fair to dark skin (Williams and Warwick, 1980). The increase in brown pigments translated into large negative shift in the L∗ values, which measures the “lightness” of shade, with the darker prosthesis samples recording lower L∗ values than fair-shade samples.
A significantly higher number of assessors assigned the “same colour” score to darker-shade samples (54.4%) having larger ΔE values than the fairer-shade samples (22.2%), suggesting that human subjects were less sensitive to incipient colour differences in the darker-shade samples (Table II). When a colour difference was perceived, a significantly higher number of assessors continued assigning the “same colour” to “acceptable” scores to darker-shade samples (54.4%) having larger ΔE values than the fairer-shade samples (22.2%), suggesting that the assessors were less sensitive to colour differences in darker-shade.
The more forgiving assessment by the human subjects of colour difference in darker shade samples may be due to the fact that under identical illuminating conditions, darker surfaces reflect less light than lighter surfaces, which in turn, may modify both visual stimuli and responses (Schwartz 1994; Falk et al. 1986). This finding may be of clinical relevance to practitioners involved in producing aesthetic silicone prostheses as well as to fair and dark skin individuals for whom prostheses have been prescribed.
Correlation between subjective assessment and colorimetric measurement
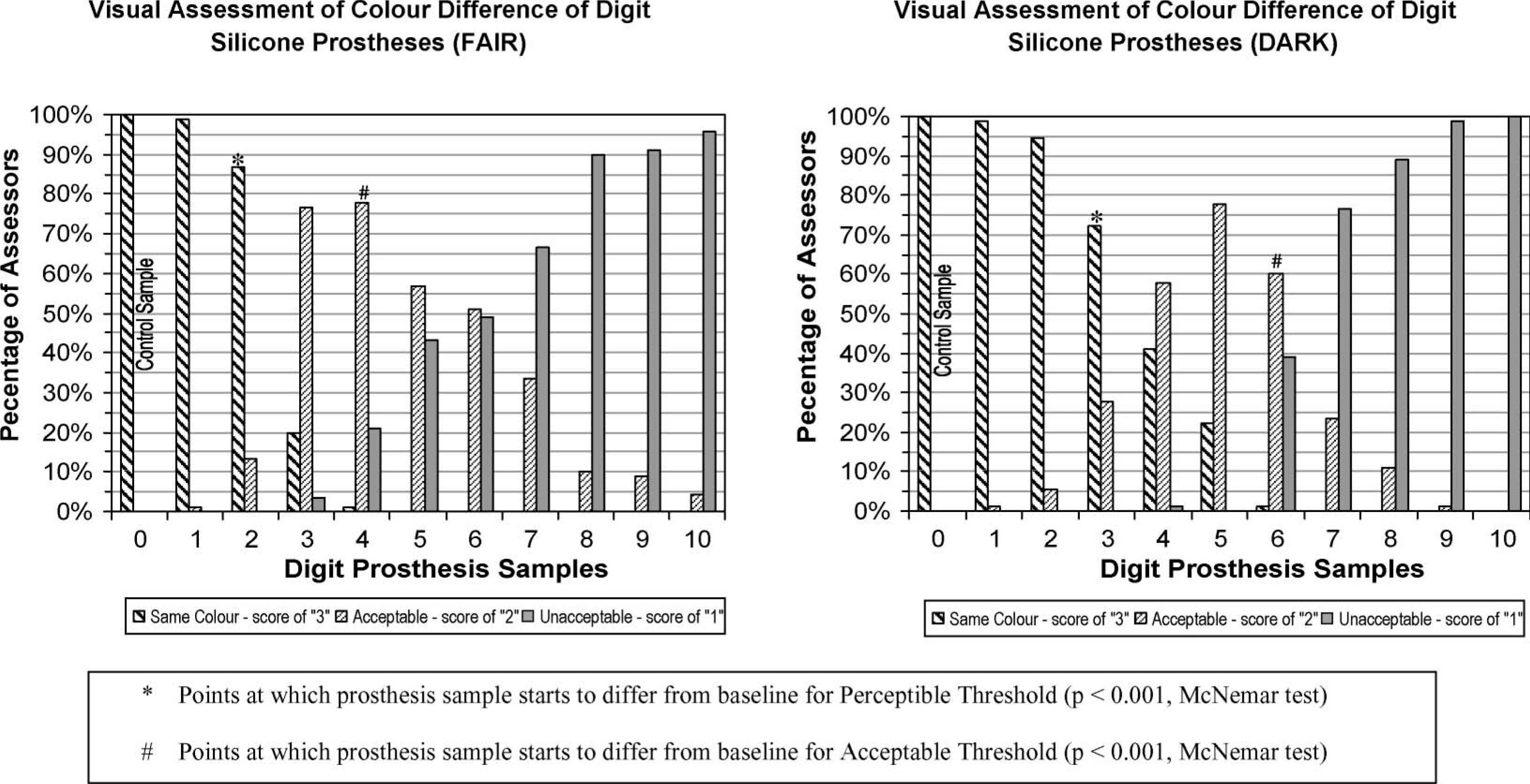
A frequent concern among patients wearing a silicone prosthesis is social acceptance of their prosthesis among their peers. Hence, the prosthetic assessment by the patient for whom the prosthesis has been fabricated is of importance. This study demonstrated that subjective visual assessment is positively correlated with ΔE values computed from colorimetric measurements for both fair and dark-shade samples (p<0.001) (Figure 4). This results show that human subjects with normal colour vision are capable of accurately assessing colour differences. The ΔE values and visual scores relationship add significance to the importance of assessment and feedback on prosthetic colour changes by the patient.
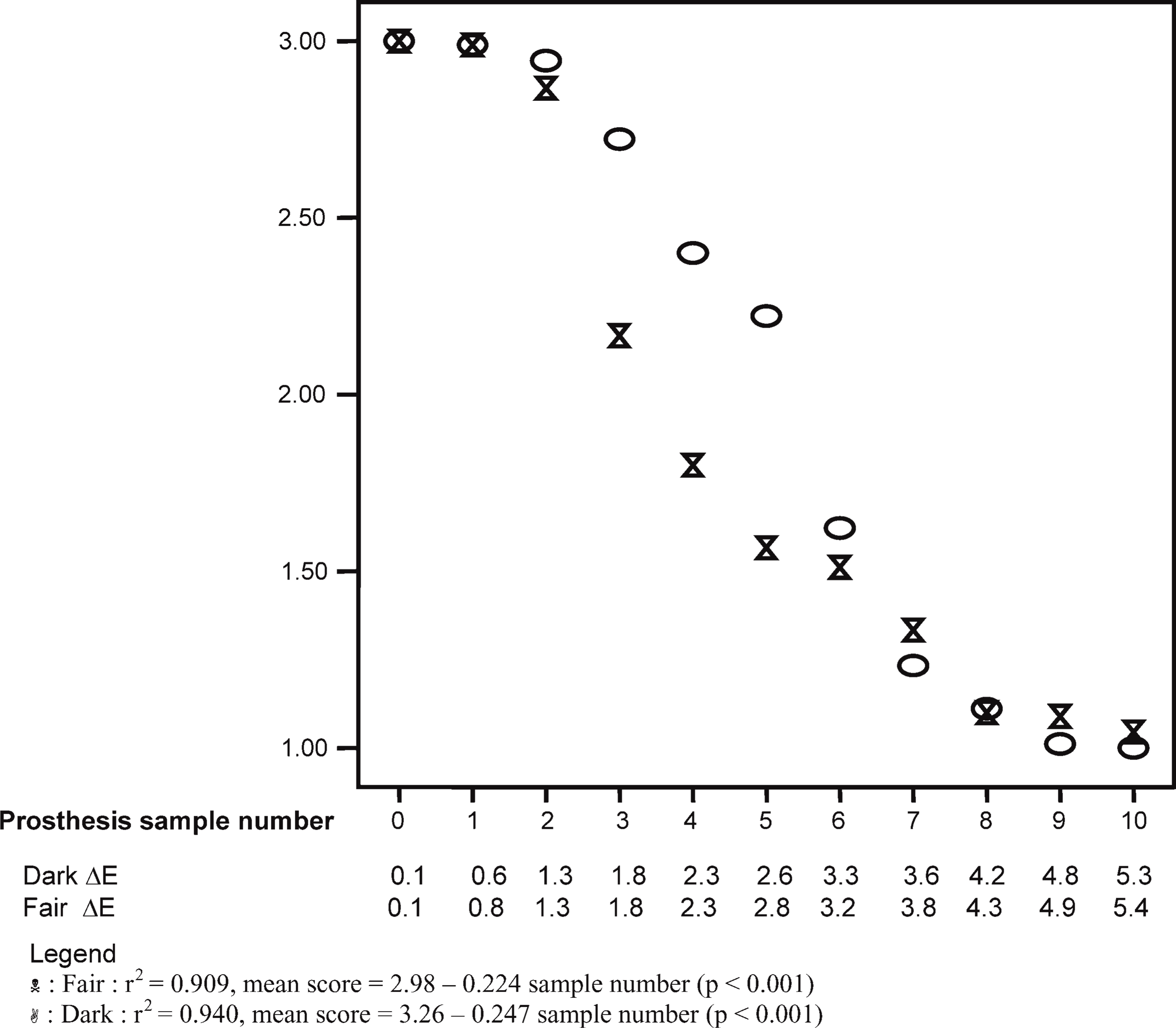
Relationship between assessors' mean score and ΔE values.
The method of systematic stepwise increments in the sample prosthetic colouration with precise quantification of pigment concentration described in this study allowed for the quantitative derivation of a threshold value for evaluating colour difference. The threshold values could also be used for evaluating colour of silicone cosmetic covers for lower limb prostheses and silicone maxillofacial prostheses and other silicone-based materials for which quality control in colour consistency is of critical importance.
In summary, the thresholds for perceptible and acceptable colour difference were determined in this study to be ΔE = 0.8 and ΔE = 1.8 for fair-shade prosthesis and ΔE = 1.3 and ΔE = 2.6 for dark-shade prosthesis respectively.