
Abstract
Background:
This case report describes the revision of a trans-tibial amputation complicated by a proximal malunited fracture. It demonstrates the complexity of decisions involved in revisions of this nature.
Case description and methods:
The patient presented has a painful stump due to breakdown of soft tissues. She had been suffering for over a year with pressure sores and inability to use a prosthesis resulting from this, decreasing her quality of life. Malunion of a tibial fracture proximal to the amputation complicated her condition.
Findings and outcomes:
Initially it was feared that the amputation level would be converted to a through-knee amputation, but wedge osteotomy of the tibia allowed coverage of the stump, increasing functionality for the patient, while still maintaining a below-knee stump.
Conclusion:
This report highlights the importance of addressing the cause of soft tissue problems in an amputation revision, which must be addressed on a case-by-case basis.
Clinical relevance
This case offers an insight into the decision-making process in limb reconstruction and suggests a solution for similar cases. It is important that all surgical options are considered before amputation length is sacrificed.
Background
The rate of lower limb amputation in the United Kingdom has been decreasing since the 1980s, though it has remained stable more recently, currently standing at around 5.1 per 100,000 population. 1 Soft tissue complications following amputation with resulting poor function unfortunately remain relatively frequent.2,3 This may be able to be managed using conservative methods such as reshaping of the prosthesis, or may require further operations. Revision rates following trans-tibial amputation are high (20%–26%),4,5 occasionally this can solely entail revision of soft tissues or shaving of growths on the bone end but loss of stump length frequently results. Patients with more distal amputations have been shown to have lower energy expenditure and those with trans-tibial amputation are more likely to achieve full mobility than those with above-knee or through-knee amputation.4, 6 Considering below-knee amputations alone, an osseous length of 2.5 cm for every 30 cm of patient height (usually 12–17 cm) is considered optimal in terms of balance between energy expenditure and optimal muscular padding. Similarly, in those requiring stump revision, it appears that functional outcome is improved where length is preserved; a longer stump length correlates with better maintenance of balance during standing.7,8 Therefore, a revision that spares as much of the stump length as possible is preferable. However, complex trauma situations lead to difficult decision-making, as factors such as patient comorbidities, complications arising from the stump and the patient’s willingness to go through further operations need to be taken into consideration.
In the herein study, a case of a traumatic trans-tibial amputation which required revision to correct a malunited fracture proximal to the amputation site is described, which was necessary in order to optimise prosthetic fit while preserving the knee joint and retaining length. No previous case reports detailing management of a malunited fracture of the tibia following trans-tibial amputation have been found by the authors.
Case description and methods
In 2005, a 24-year-old woman was involved in a high-energy road traffic collision (RTC), sustaining a segmental right tibial injury with traumatic amputation at the mid diaphysis and an open fracture at the metaphyso-diaphyseal junction. In the same incident, she also suffered multiple other fractures, including a pelvic ring, and ipsilateral femoral and contralateral tibial injury. Previously, the patient was fit and well and was a full-time mother looking after two small children. Initial management included pelvic external fixation, intramedullary nailing of the ipsilateral femoral fracture, soft tissue management and formalisation of the tibial amputation to a 17-cm residuum. Internal fixation of the more proximal fracture was not carried out as the risk of infection was felt to be too high; the metaphyseal injury was treated non-operatively (Figure 1). A skin graft was required to close the soft tissues; this was carried out secondarily. The patient was referred to the prosthetic department and received physiotherapy including gait training.
Post-operative (a) AP and (b) lateral radiographs after initial treatment.
After 2 years, the patient was unable to use her prosthesis due to problems with the skin graft and prominence of the underlying bone end. She therefore underwent initial stump revision with shortening and soft tissue reconstruction, but management at this time did not address the malunited fracture of her tibia and therefore did not address the angulation of the tibia likely leading to the soft tissue breakdown. After she had recovered and could use her prosthesis satisfactorily, responsibility for her care was transferred to a rehabilitation clinic.
The patient represented during May 2010 with repeated stump infection. Unfortunately, presentation was delayed, and when initially consulted, she had established pressure sores over the medial and lateral aspects of her knee. She had been unable to use her prosthesis for several months despite prosthesis adjustment and gait training.
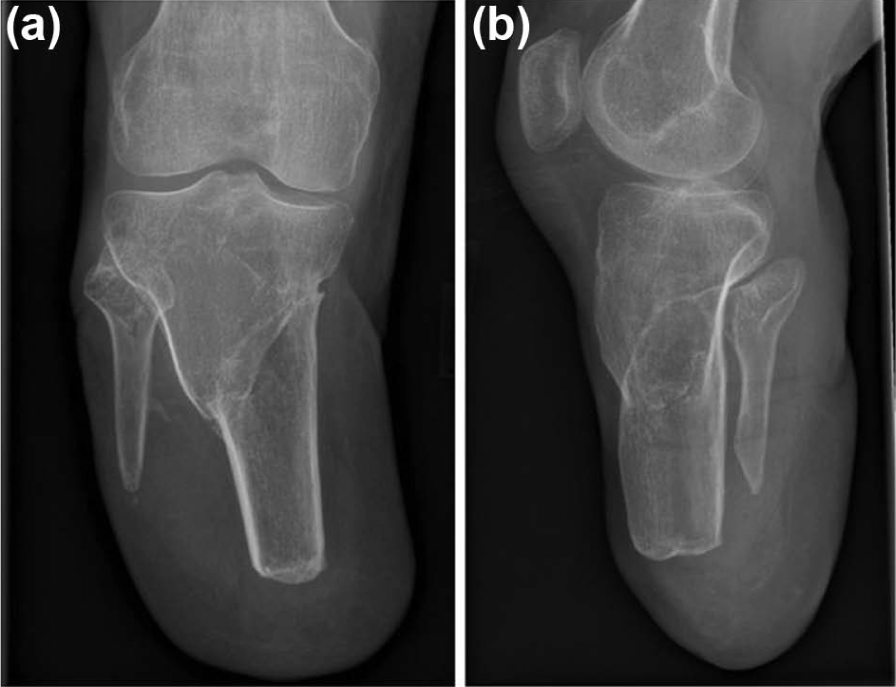
Plain radiology showed a varus malunion of the metaphyseal tibial fracture she sustained in the original RTC proximal to the amputation site (Figure 2). A magnetic resonance imaging (MRI) scan was carried out revealing no evidence of osteomyelitis.

(a) AP and (b) lateral radiographs immediately following corrective osteotomy and internal fixation of residual tibia to correct alignment and optimise prosthetic fit.
At this point, the treatment options included converting to an above-knee or through-knee amputation or stump revision (in the form of an osteotomy) to maintain length. The risks and rewards of these options were discussed with the patient particularly highlighting the fact that:
An above-knee amputation would result in lower risk of complication or further revision at the expense of reduced function capacity.
Further stump revision would carry a higher risk of complication and a potentially longer recovery time but increased quality of life if successful, once a prosthesis could be used. After this discussion, the patient agreed to further revision of her stump to attempt to enable her to use a below-knee prosthesis again.
Findings and outcomes
In February 2011, a 20° closing wedge osteotomy of the proximal tibia just below the tibial tuberosity was carried out. Osteosynthesis was performed using bilateral reconstruction plates. This left a soft tissue deficit which was accepted in order to maintain adequate length. In all, 4 days later, the patient underwent split skin grafting to the stump, bone grafting to her tibia and refashioning of the fibular head. The bone graft was harvested from the right anterior iliac crest. This revision corrected the alignment of the tibia while maintaining the length of the stump (Figure 3). The post-operative course was complicated by a superficial infection of the bone graft harvest site, which was managed with a course of oral antibiotics.

AP and (b) lateral radiographs at 6 months follow-up demonstrating union of the osteotomy.
In May 2011, imaging showed complete healing of the tibia; at this time, the patient was still using a wheelchair (Figure 4). Prosthetic fitting and gait training was then possible, and the patient was full weight bearing with a new prosthesis by July 2011.
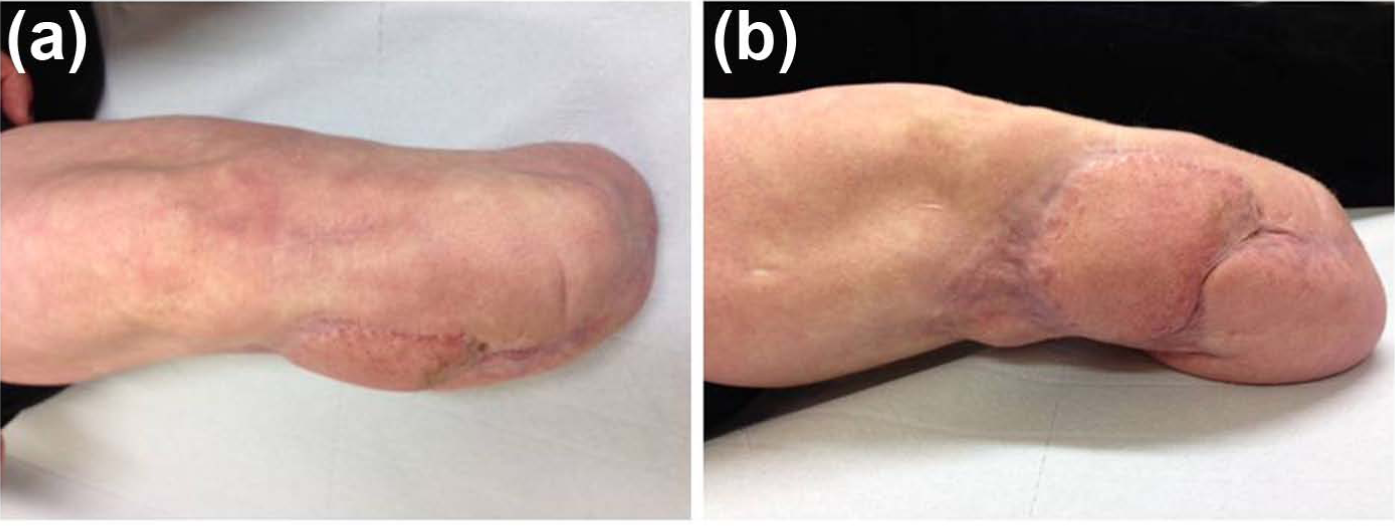
(a) AP and (b) lateral photograph illustrating the state of the soft tissues.
Discussion
With significant numbers of patients requiring amputation for various indications every year, stump complications impairing function remain an important clinical problem. A proportion of such patients may benefit from revision surgery.
This case is unusual due to the added issue of a fracture and subsequent malunion proximal to the amputation. To our knowledge, such a situation is previously unreported. The malunion of the fracture led to a varus deformity of the stump which caused soft tissue breakdown and prevented the wearing of a prosthesis. Osteotomy of the tibia improved alignment allowing better soft tissue balancing and coverage of the stump and better prosthetic fitting. The revision in this way increased function without significant loss of stump length thereby avoiding the increased morbidity associated with a higher amputation. Since the accident, this patient has been unemployed and suffered from depression. Recurrent painful problems with her stump resulting in inability to use her prosthesis and loss of mobility are likely to be significant contributors to this. The revision of her stump allowed the patient to again wear the prosthesis for the first time in over a year.
Our objective was first to correct the bone deformity by performing a tibial osteotomy. This would lead to better soft tissue balancing and better distribution of loading forces during limb fitting and walking. For reconstruction of the osteotomy, two low-profile plates were selected to minimise subsequent irritation to the underlying soft tissues. Bone graft was used to provide an osteogenic stimulus facilitating early bone repair. This is critical in situations where the soft tissue envelope has been compromised and healing delay is anticipated. We used an autogenous bone graft harvested from the iliac crest. Autogenous bone is ideal as it has complete histocompatibility leading to minimal rejection and contains all the important properties for bone regeneration (osteoinductivity, osteoconductivity and osteogenecity). Limitations of autogenous bone grafting are need for additional surgery and resulting donor site morbidity; 9 in this case, a donor site infection required admission to hospital but was managed medically with no long-term complications. The bone excised in the osteotomy can also be considered for grafting purposes, but care must be taken to ensure viability, and this should never be performed if there are concerns about infection.
Bone grafting is commonly necessary in fracture non-unions and ideal in patients who have had previous failed attempts at non-union repair or who have mechanical issues leading to non-union. 10 A non-union after the osteotomy would have been a serious complication as it would have led to further surgery, more scarring and further insult to the surrounding soft tissues. We recommend that when such procedures are contemplated, bone grafting should be performed routinely to reduce the risk of non-union and to accelerate the healing process.
Skin grafting was necessitated to complete the soft tissue reconstruction. Skin grafts enable keeping of length of the stump, therefore allowing preservation of joints. Problems may occur due to ulceration and breakdown of the graft, but these are usually minor and can be healed by resting of the stump without a prosthesis for a few days or by prosthetic adjustments. 11
A possible technique in patients with a high physical demand is to use a bone bridge between the tibia and fibula. The bridge grafting of the fibula can increase strength and stability in the resulting residuum, especially if the bone length is short. This technique remains controversial and was not used in this case as it was felt that adequate stability was produced by the osteotomy and bone grafting for the patient to have a good quality of life.
In such complex revision cases, early referral to specialist limb reconstruction service should be considered to allow all treatment options to be discussed with the patient. These decisions may impact the patient’s quality of life and expectations for the future greatly.
An above-knee amputation may be the easier choice, with lower complication and subsequent revision rates. However, if the patient may not be satisfied with the resultant quality of life, it is important to consider more complex surgery, with the option of transfer to a higher amputation in the future.
Conclusion
This is an unusual and complex case that has required extensive revision over several years. The impact of having a stump unusable with a prosthesis on the patient’s quality of life was profound. It is likely that restoration of her ability to use a prosthesis will greatly improve her personal and family situation. The case highlights the need for careful consideration of the causes of soft tissue problems. The initial revision surgery, which did not address the malunion, failed to resolve these issues. However, such interventions are demanding for both the surgeon and the patient, and need to be carefully considered on a case-by-case basis. A multidisciplinary approach is necessary to achieve the optimum outcome.
Footnotes
Conflict of interest
The authors declare that there are no conflict of interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.