
Abstract
Background:
Literature mostly describes the cosmetic role of prostheses for finger amputation. The impact on hand function has not been systematically explored.
Objectives:
Our aim was to describe the impact of silicone finger prostheses on hand function and gripping ability.
Study design:
Prospective descriptive cross-sectional study.
Methods:
We included 42 adult patients with partial or complete single- or multiple-digit amputation of one hand. We evaluated hand function of the injured hand without and with the prosthesis with the Southampton Hand Assessment Procedure, and grip power and tracking ability with a grip-force tracking system.
Results:
Southampton Hand Assessment Procedure grip index scores were slightly higher when using the prosthesis as compared to not using it (though not reaching the minimum real difference reported in the literature), except for lateral grip. Grip power was not significantly affected by prosthesis use for power grip and lateral grip and slightly diminished for tip grip. Tracking errors only differed with respect to the signal type but not with respect to using the prosthesis.
Conclusion:
A minimum improvement of hand function can be expected at best with silicone prostheses for finger amputation, accompanied by a slight decrease in tip grip power.
Clinical relevance
Based on our results, an evidence-based explanation can be given to patients after finger amputation regarding the functional benefits that can be expected from a silicone prosthesis.
Background
Finger amputations are the most frequent amputations of upper limb. 1 The estimated annual incidence rate of traumatic finger amputations is 1.9 per 100,000 for the age group between 25 and 65 years. 2 In the words of the International Classification of Functioning, Disability and Health, amputations can cause a wide range of activity limitations and participation restrictions. 3 The acute surgical treatment is followed by rehabilitation aimed at restoring the previous functional level, enabling return to work and preventing psychological trauma. Several rehabilitation methods are available: activity modification, use of adaptive equipment that aids in functional skill compensation or use of prostheses. There are different options for finger prostheses: passive silicone prostheses, body-powered prostheses, externally powered prostheses for total finger amputation or task-specific prostheses. 4 Presently, silicone prostheses for finger amputation are the only option for finger restoration in our country.
Silicone prostheses are constructed either using a mould that defines the shape of the prosthesis or with direct modelling of silicone on a model of the stump. 5 There are four different suspension types: vacuum, suspension with medical glue, mechanical attachment on fingers next to the stump or by means of osseointegrated implants. Vacuum suspension is frequently used; medical glue is used if the finger stumps are too short or when the fingers are amputated at the level of metacarpophalangeal joint. 5 Silicone prostheses provide aesthetically pleasing results, but the evidence that they also improve functioning is not firm.
The existing literature mainly describes the cosmetic role with psychological benefits of such prostheses;1,6,7 their impact on hand function has been less explored. Most of the studies have used non-standardised questionnaires as outcome measures in patients with prostheses for finger amputation.6–12 We only found one study that used a validated questionnaire (Disabilities of the Arm, Shoulder, and Hand (DASH)) for assessing activities of daily life (ADL) after finger amputation. 13 That study showed an improved ability to perform ADL with the prosthesis. 13
There is one published report providing a more precise description of the impact of finger prostheses on hand function. 14 The finger prosthesis for an amputated thumb should enable proper opposition to the fingers. 14 It also makes it possible to hold objects too large for the fingers themselves to encircle. 14 When the ring finger is amputated, long fingers deviate ulnarly and by providing prosthesis for the missing ring finger, stability to the fingers should be added during lateral pinch. 14 This should also keep small objects from falling out of the hand when fingers are held together. 14 The prosthesis extends the digit to its normal length, which is supposed to improve precision grip because it enables the pulp of the thumb to oppose the pulp of the prosthetic digit. 14 We found another case study of a patient with osseointegrated prosthesis mentioning that in thumb and index finger amputation, power grip could be improved with the use of the prosthesis. 15 However, all these statements are probably based on clinical experience because no scientific methodology employed to derive them is reported.
Similarly, we found only one study describing the impact of a silicone prosthesis on grip power as assessed by a dynamometer. 13 The results showed improvement of grip power by using the prosthesis, although the number of included patients was very small (n = 10). Another limitation of this study was large variability among the patients, who had different fingers amputated at different levels, different numbers of amputated fingers and different sides of the amputation with respect to hand dominance. Up to now, there have been no studies systematically addressing the impact of finger prostheses on hand function with regard to the side of amputation (left/right and/or dominant/non-dominant) or the number of amputated fingers.
The aim of our study was to evaluate the impact of silicone finger prostheses for finger amputation on hand function, grip power and grip-force regulation by comparing the measurements with and without a finger prosthesis.
Methods
We included all the adult patients with partial or complete single- or multiple-digit amputation of one hand and a intact and uninjured other hand who were examined at the Outpatient Clinic for Prosthetics and Orthotics of the authors’ institution between August 2010 and December 2012 and received a new silicone prosthesis for finger amputation during this time. We included the patients who either received a prosthesis for the first time or were entitled for prescription of a new prosthesis according to the health insurance regulations (which allow replacement every 3 years). The patients who received a prosthesis for the first time had at least 2 months for getting used to the prosthesis before we evaluated their hand function, grip power and grip-force tracking ability. All the patients received silicone prostheses; suspension was ensured either solely by vacuum or in the case of shorter stumps, medical glue or mechanical attachment onto the fingers next to the stump.
We excluded patients who had neurological or rheumatologic diseases or previous hand injuries. The participating patients were a random subset of those involved in a previously published study that explored the differences between the injured hand without the prosthesis and the intact hand. 16 All the participants participated voluntarily, and the study was conducted in accordance with the Declaration of Helsinki on biomedical research on human beings and the Oviedo Convention. The study was approved by the National Medical Ethics Committee.
We evaluated hand function of the injured hand with the Southampton Hand Assessment Procedure (SHAP) test. 17 The SHAP test consists of 26 timed tasks (12 abstract tasks and 14 activities of daily living). The test’s outcome measure is a contextual rating of functionality (relative to that of normal hand function) that evaluates tripod pinch, tip grip, lateral pinch, power grip, spherical grip and extension grip. 17 The results of the test are expressed as Index of Functionality for each grip ranging from 0 to 100; 16 the functionality profile for unimpaired participants lies between 94 and 99. 16 The SHAP has been designed for evaluation of effectiveness of upper limb prostheses.17,18 It has been validated, 17 and normal values have been determined for the healthy population of different ages in our country. 19
We also evaluated grip power and tracking ability with a grip-force tracking system. 20 The system consists of two force-measuring units of different shape (Figure 1). Grip power measurements for power, tip or lateral grip can be made when the patient applies grip force to the measuring unit. The units are connected to a computer, which enables visual feedback and data acquisition. 20 The system measures forces up to 100 N a resolution of about 0.03 N. 21 Force assessment with this system has been shown to be more accurate compared to the commonly used mechanical dynamometers. 21 The measurements were performed three times and the best result was used for further analysis. Grip-force tracking ability was measured for power grip for all patients, and for tip grip for those patients who had index finger amputation – either only the index finger or in combination with other finger amputations. Three types of signals were used in the tracking tasks – sinusoid, rectangular and random. The order of the tasks was randomised between patients by the computer.
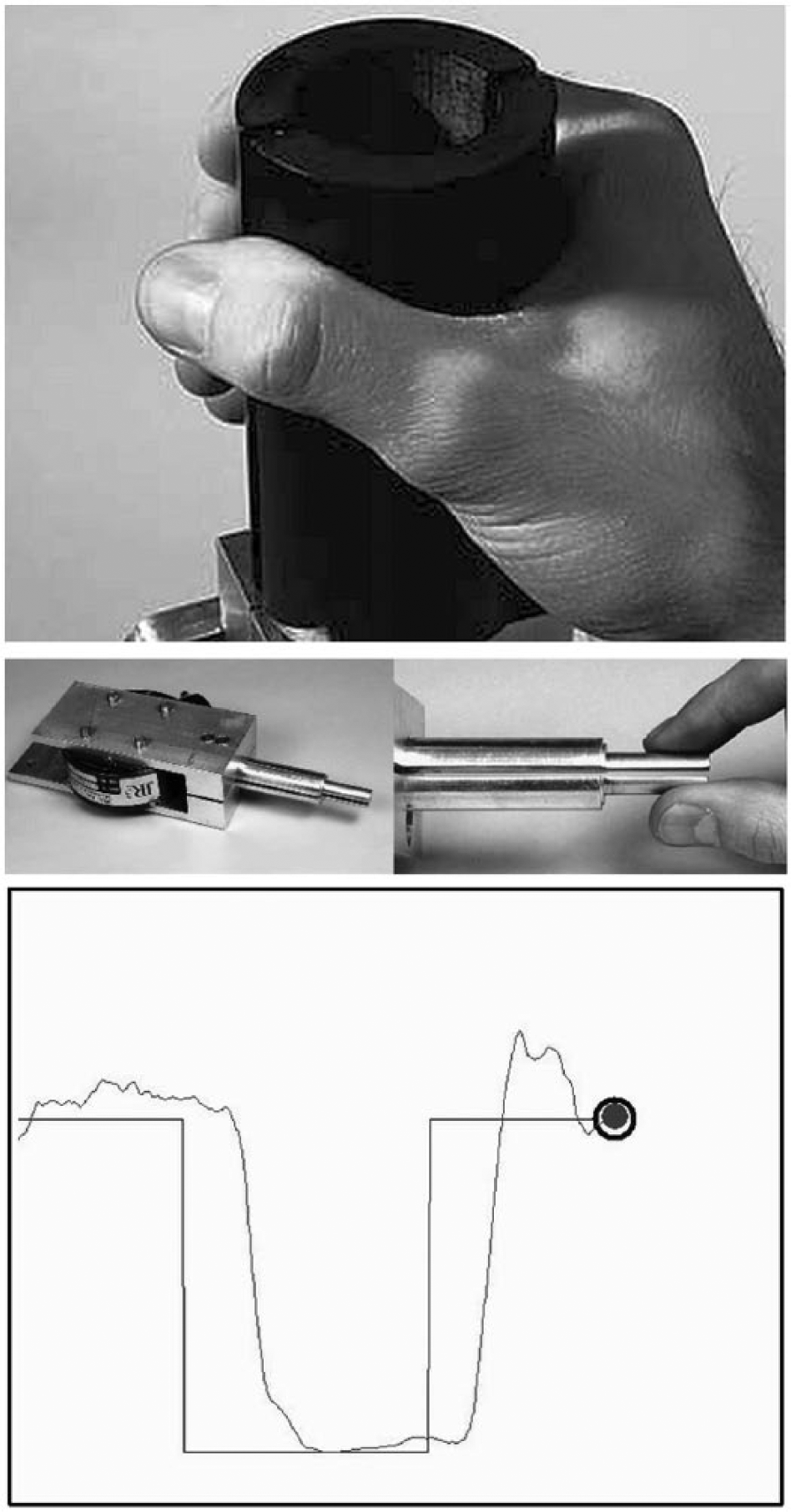
The system for measuring grip power and grip-force tracking ability – the unit for measuring power grip (top panel), the unit for measuring tip grip (middle panel) and a screenshot of a grip-force tracking session with rectangular signal (bottom panel; the grey curve is the user’s response). See section ‘Methods’ and the Kurillo et al.20,21 for references details.
All the patients first performed the SHAP test. Order of prosthesis use (with, without) was randomised. The subsequent grip power and tracking ability measurements were also performed in a random order with respect to prosthesis use.
Paired-samples t-test and Wilcoxon matched-pairs test (exact version) were used to statistically compare the injured hand without and with the prosthesis regarding SHAP index scores and grip strength measurement results. For tracking error evaluation, we applied the square-root transformation to the data before further analysis because the tracking error distributions were right-skewed. This way, mean skewness across assessment conditions was reduced from 1.45 to 0.18 (median from 1.44 to 0.75) and homogeneity of variances was also improved. We performed two-way repeated-measures analysis of variance (ANOVA) stratified by grip type (power, tip) to the transformed data because the number of patients and the type of their amputations differed between the two grips. The within-subject factors were signal shape (sinusoid, rectangular, random) and hand (intact, affected without prosthesis, affected with prosthesis). In addition, we tested whether the effect of prosthesis on SHAP scores and grip power (i.e. difference scores between prosthesis use and no prosthesis) differed according to the amputation type using both a parametric (one-way ANOVA) and a nonparametric test (Kruskal–Wallis test, exact version).
Differences according to amputation type were also tested for tracking errors (see section ‘Results’ for details). Statistical analyses were performed using the IBM SPSS Statistics 20 software (IBM Corp., Armonk, NY, USA, 2011). Statistical significance threshold was set at p = 0.05.
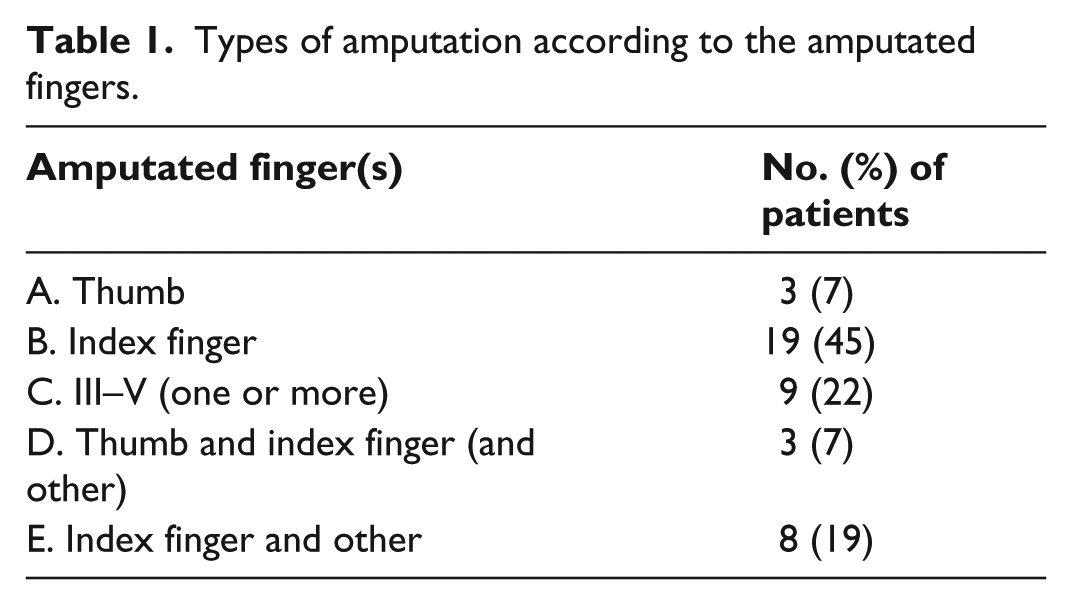
Sample size was estimated according to SHAP overall index score as the primary outcome based on previous research. 16 In order to achieve 80% power (at 5% alpha level) for detecting a 2.5-point difference (i.e. one that exceeds the estimated minimum real difference (MRD) of 2 points 18 ) using a paired-samples t-test, given that the standard deviation of difference scores is 5, a sample size of 34 is required. We included eight more participants to accommodate the lower power of the nonparametric Wilcoxon test that we used in parallel to the t-test, and to increase the size of the amputation-type subgroups. The amputation types (Table 1) were specified in advance as explained in the previous study. 16
Types of amputation according to the amputated fingers.
Results
We included 42 patients (22 women and 20 men) in the study. They were 17–70 years old (average 42.2 years, median 44 years). About one-third of the patients (31%) had completed vocational school or less, 24% had completed high school, 24% had higher educational level (tertiary educational level), 14% were retired and 7% were high-school or university students. Most of the patients were injured in their spare time (64%); 52% of the patients remained employed full time at the same job as before the injury, 19% continued working full time in a different job position, 17% continued their schooling process and 12% retired as a consequence of the injury.
The majority of the patients had single-finger amputation (28, 67%); nine patients had two fingers amputated (21%), four had three (10%) and one patient had four (2%) fingers amputated. Index finger was the most commonly injured finger (Table 1). There were 62 amputations in total; the details of the amputation level are summarised in Table 2. The dominant side (23 patients, 55%) was more frequently involved than the non-dominant side (19, 45%). This was practically equivalent to the right versus left side because the right side (which was injured in 60% of the patients) was the dominant side in 23 of 25 cases, and the left side (injured in 40% of the patients) was the non-dominant side in all the 17 cases.
Location and level of the amputated fingers.
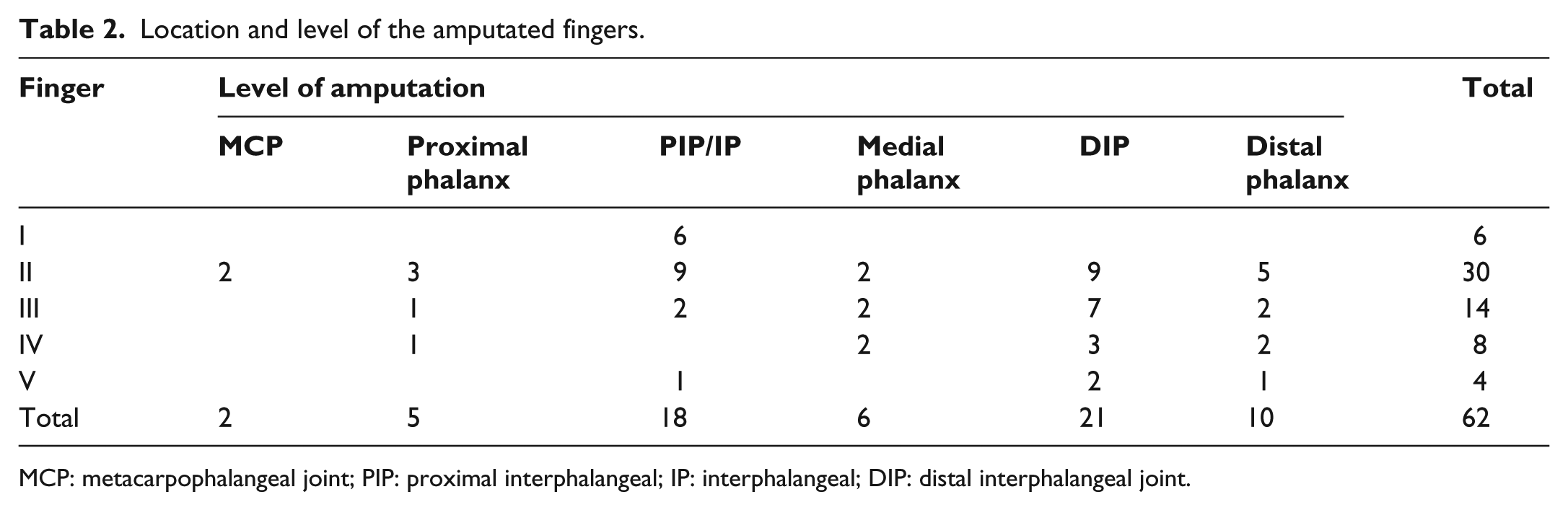
MCP: metacarpophalangeal joint; PIP: proximal interphalangeal; IP: interphalangeal; DIP: distal interphalangeal joint.
Suspension of the prosthesis was ensured with medical glue for three patients and for further three patients with mechanical attachment onto the fingers next to the stump. For the other patients, vacuum suspension was adequate.
The grip indexes obtained from the SHAP test were somewhat better on average with the prosthesis than without the prosthesis, except for lateral grip (Table 3). The prosthesis statistically significantly increased the average score for spherical and extension grip, but both differences were smaller than the recommended MRD. We found no statistically significant differences between amputation types regarding the effect of prosthesis on the performance on the SHAP test (p-values ranging from 0.198 to 0.979; detailed results omitted for brevity and available from the authors upon request).
Descriptive statistics and summary of statistical tests for the SHAP test.
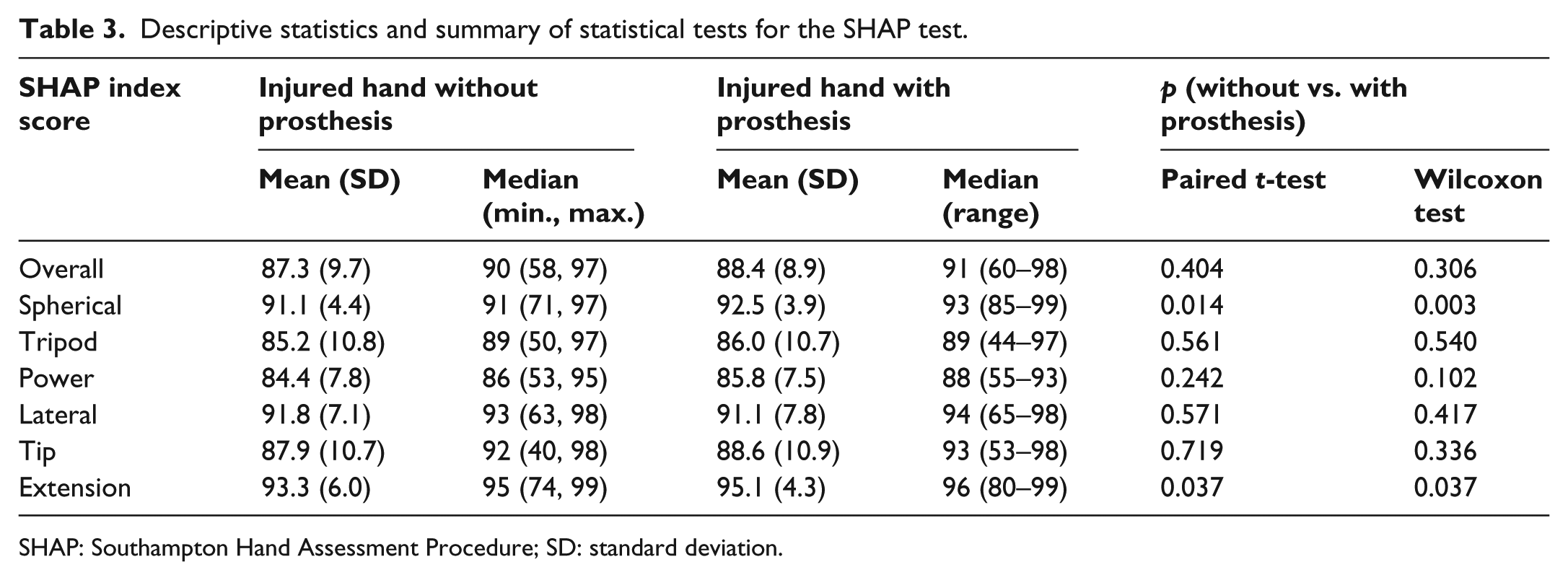
SHAP: Southampton Hand Assessment Procedure; SD: standard deviation.
The power of power grip was not statistically significantly affected by prosthesis use (Table 4). The power of tip grip statistically significantly diminished with the prosthesis (Table 4; by about 10% on average). The effect of prosthesis use on grip power did not differ with respect to amputation type for power grip (ANOVA: p = 0.574, Kruskal–Wallis test: p = 0.850) and tip grip (ANOVA: p = 0.199, Kruskal–Wallis test: p = 0.129), but it did differ for lateral grip (ANOVA: p = 0.031, Kruskal–Wallis test: p = 0.022). Lateral grip power improved with the prosthesis after amputation of one or more among the middle, ring and small fingers (type C) and worsened with the prosthesis after amputation of the index finger together with at least one other finger (types D and E; Table 5). Prosthesis use appeared to worsen lateral grip power after amputation of only the thumb (type A), but there was large variation between those three patients.
Descriptive statistics and results of statistical tests for grip power measurements.
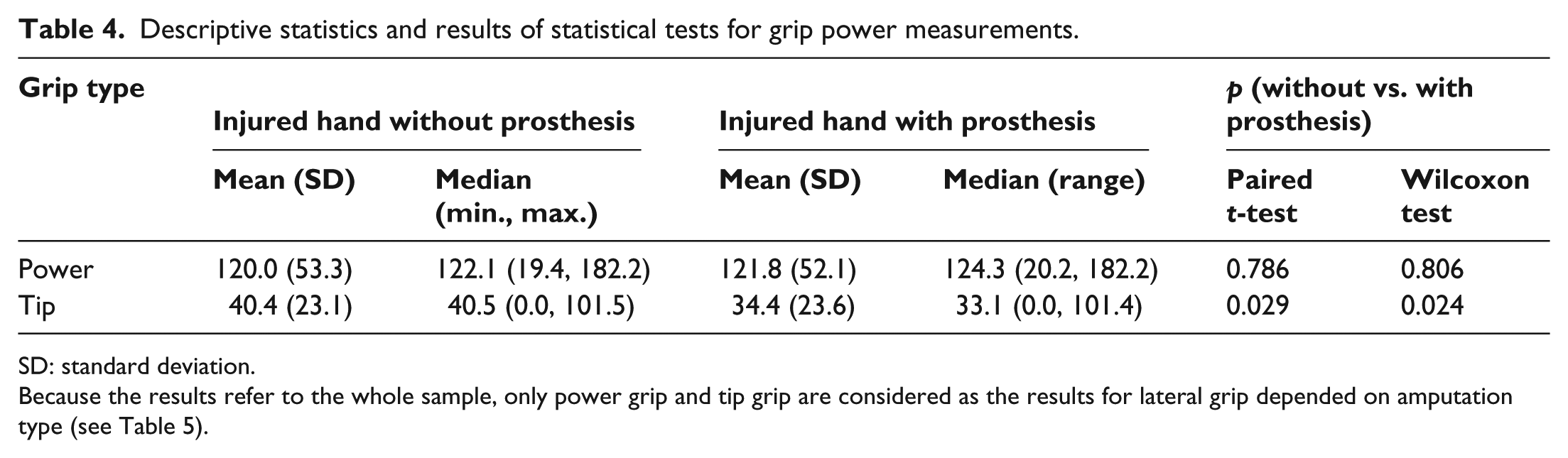
SD: standard deviation.
Because the results refer to the whole sample, only power grip and tip grip are considered as the results for lateral grip depended on amputation type (see Table 5).
Descriptive statistics for the difference in force of lateral grip between using and not using the prosthesis with respect to amputation type.
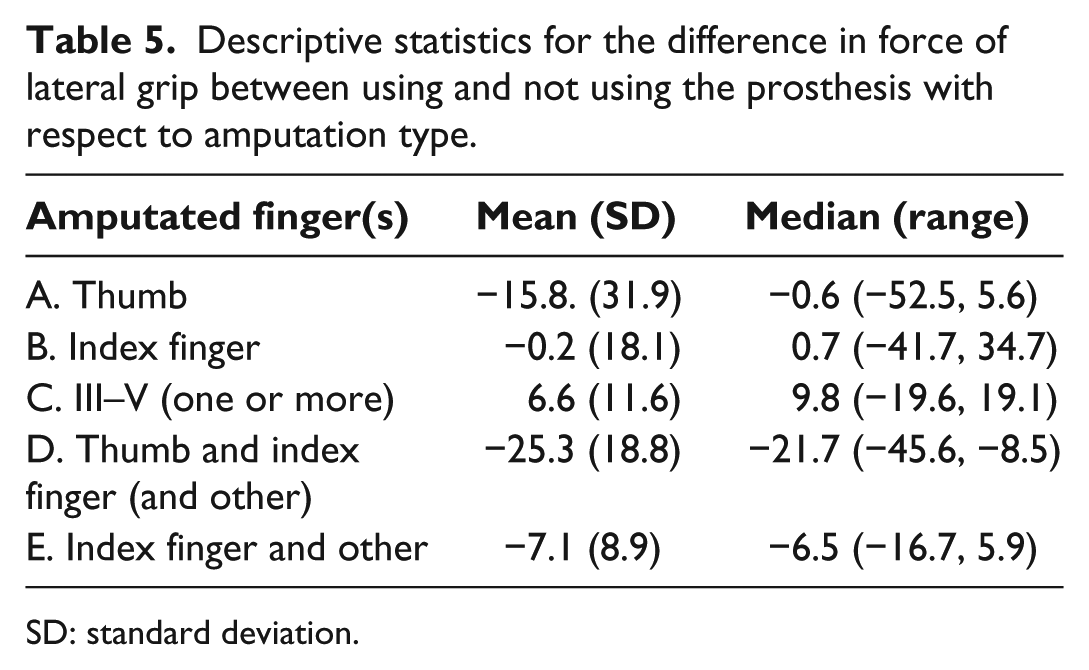
SD: standard deviation.
For grip-force tracking ability, the signal effect was statistically significant for power and tip grip while there was no statistically significant effect of prosthesis or hand-prosthesis interaction (Table 6). Hence, the tracking errors only differed with respect to the signal type with no systematic differences between the injured hand without prosthesis and the injured hand with prosthesis. On average, the tracking error was the smallest with the random signal followed by the sinusoid signal, and it was the largest with the rectangular signal (Figure 2). It should be emphasised that all the statistical conclusions were the same if untransformed data were analysed (results omitted for brevity).
Summary of statistical analyses of tracking errors.
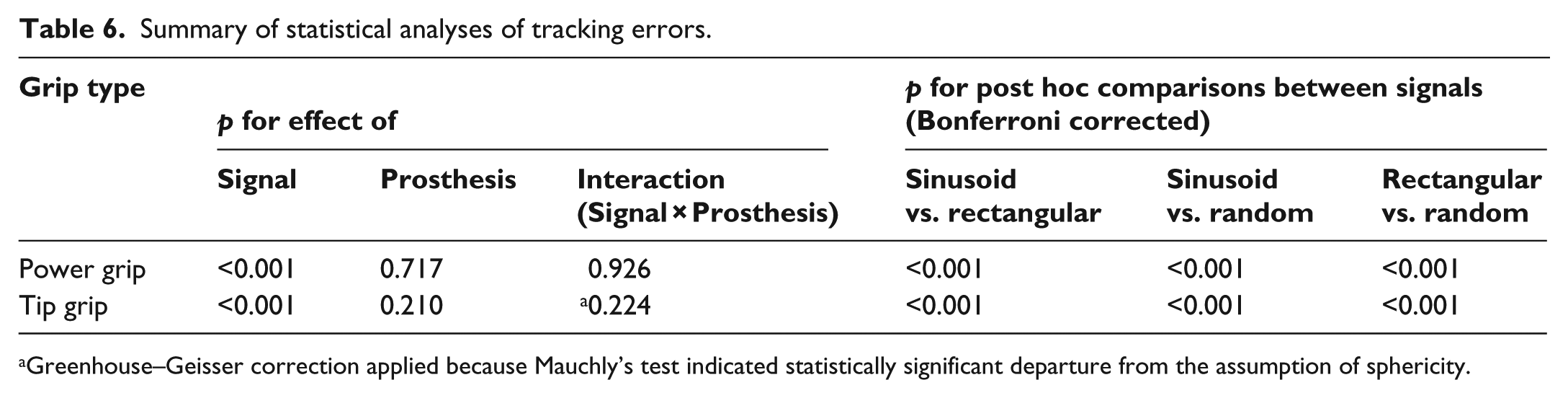
Greenhouse–Geisser correction applied because Mauchly’s test indicated statistically significant departure from the assumption of sphericity.
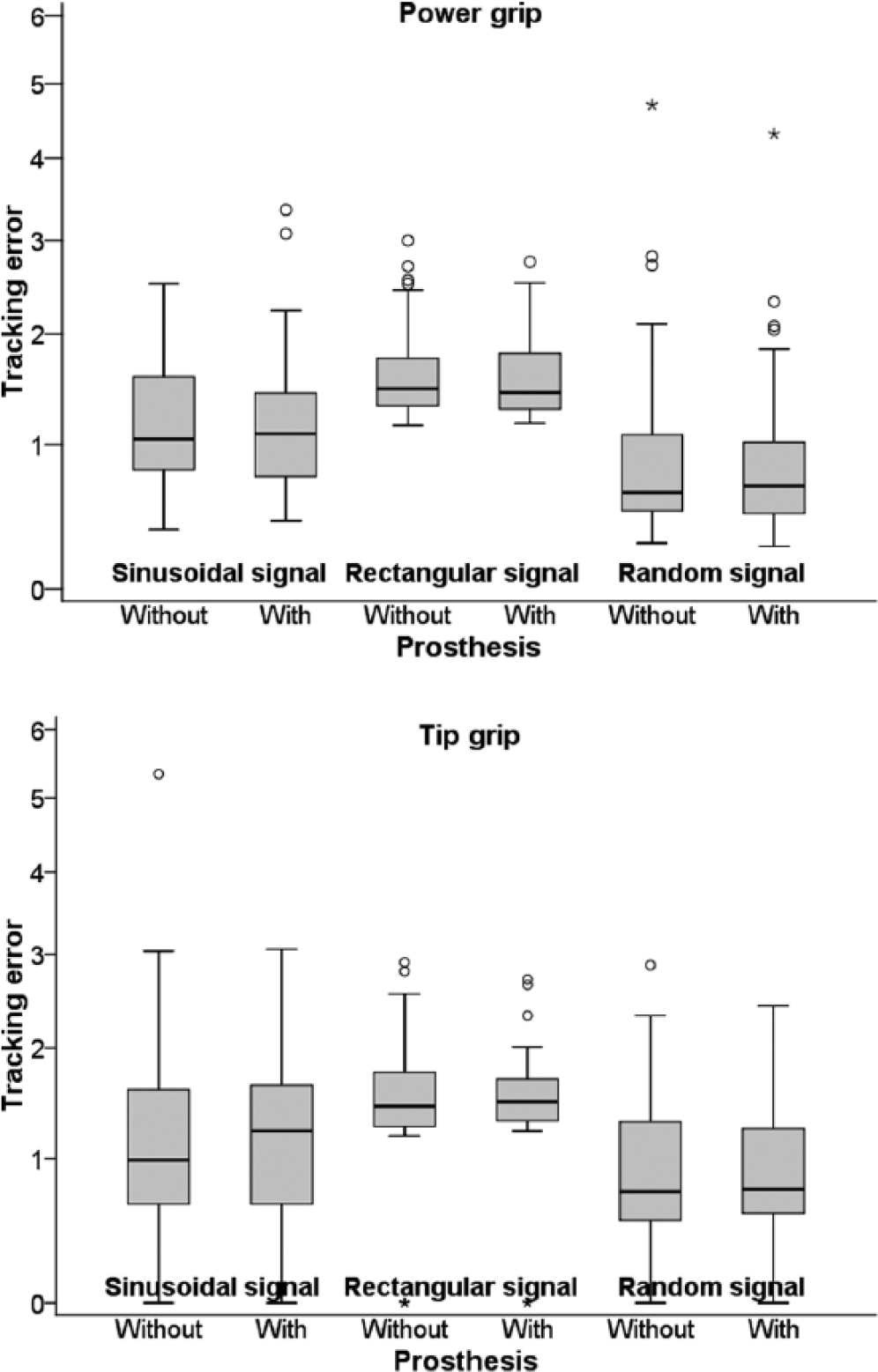
Distributions of tracking errors for power grip and tip grip (boxplots – thick horizontal line denotes median; box denotes interquartile range; whiskers denote non-outlier range; circles denote outliers; asterisks denote extremes; the vertical axis is in square-root scale to display the data as transformed before statistical testing).
To check whether tracking errors differ according to the amputation type, we first calculated the geometric mean for each patient over the tracking error with and without prosthesis. For these data, we tested the difference in average value between the groups defined by amputation type. We found no statistically significant differences in any signal type (p-values ranging from 0.488 to 0.955; detailed results omitted for brevity and available from the authors upon request). These results speak in favour of the validity of the main analysis above in the sense of justifying a pooled analysis of all patients regardless of amputation type.
Discussion
Our study was designed to evaluate the impact of finger prostheses after finger amputation on hand function and grip strength. On average, we found the SHAP grip index scores to be somewhat higher when using the prosthesis as compared to not using it, except for lateral grip. Spherical and extension grip function appeared to be the most improved when using the prosthesis, but the change fell short of the MRD. The improvements should be viewed with particular caution because the MRD had only been estimated for the overall SHAP index score 18 and the MRDs for individual grip scores should have a larger MRD as shorter scales are less reliable by definition and should thus have a larger standard deviation of repeated measures if the scale range remains unchanged, which is the case of SHAP indexes that are all standardised to range from 1 to 100.
Our results of the SHAP test are not in agreement with Pillet’s 14 statement that prostheses improve lateral grip. Pillet’s 14 overview also states improvement of pinch grip of any distal amputation and power grip when using prostheses in thumb amputation, whereas in our study, this was not confirmed. We also found no differences between amputation types regarding the effect of prostheses on the performance on the SHAP test.
Other researchers6–12 used their own questionnaires or semi-structured interviews for evaluation of rehabilitation after finger amputation. In the study by O’Farrell et al., 10 23 of 50 patients reported improvement of hand functionality with prosthesis. A somewhat smaller proportion of patients (12 of 33) described improvement of gripping and picking up objects in the study by Alison and Mackinnon. 8 Pilley and Quinton 12 describe similar results: 4 of their 15 patients reported improved function. The same number of patients reported an improvement of grip function, whereby three of them had amputation of the index finger. Their study also supports a benefit in activities involving striking movements, such as typing, which had been previously described by Beasley and De Beze. 22 Similarly, O’Farrell et al. 10 also described an improvement in typing, although not in playing the piano.
Our results indicate that grip power is not affected by prosthesis use (in the case of power grip), is affected differently by different amputation types (in the case of lateral grip), and is slightly diminished with the prosthesis (in the case of tip grip). Lifchez et al. 13 described improvement of grip power with prosthesis use for tripod grip in one of the five dynamometer positions, while all other grips did not statistically significantly differ from each other. However, their study sample was very small and heterogeneous (10 patients with diverse amputations), so their conclusions are less likely to be generalisable.23,24
Because information on maximal grip strength mainly provides information on short-duration muscle strength, 25 we used tracking error for a better evaluation of the ability to control the grip strength of sub-maximal forces, which are more commonly used in daily activities. 26 We observed no difference in the achievements between the injured hand and the injured hand with the prosthesis. Similar tests have not been used up to now in this population, so our results put into question the objectivity of the improvement in ADL when using a prosthesis observed with the DASH test. 13
The agreement between parametric and nonparametric statistical tests, as well as between inference from untransformed and transformed data, speaks in favour of validity of our conclusions. The total sample size is also an advantage compared to the majority of related studies. Nevertheless, the main limitation of our study is that the sample was not large given the notable heterogeneity between the patients regarding the number of amputated fingers, which finger(s) was/were amputated and the level of amputation. Therefore, we recommend future studies to include a larger sample of patients or focus on a specific amputation type. Furthermore, other groupings of amputation types could be used in the study design and data analysis, such as the division into complete amputation, short stumps and long stumps.
In addition, we may not have assessed all the relevant aspects of hand function despite the wide variety of SHAP tasks and extensive grip power and tracking ability measurements. Our personal clinical experience includes several cases in point, most notably an accordionist to whom a silicone prosthesis for the left hand (with which bass chords are played) restored the possibility to play the musical instrument. His prosthesis was actually reinforced with thin metal bands in order to prevent undesired twisting in the virtual joint, so a future study might confirm larger functional benefits measurable with the SHAP test or a grip-force tracking system for such reinforced finger prostheses.
Conclusion
Our study confirmed that a slight improvement of hand function with a prosthesis is likely in finger amputation, except for lateral grip. The power of power grip and lateral grip was not significantly affected by prosthesis use, whereas the power of pinch grip tended to diminish slightly with the prosthesis. Prosthesis use did not affect grip-force tracking errors. While putting into question some previously published statements, our results are clinically relevant in the sense that evidence-based explanation can be given to the patients after finger amputation about what functional gain, if any, they can expect apart from the known cosmetic (and associated psychological) benefits if they opt for a silicone prosthesis.
Footnotes
Acknowledgements
We are deeply grateful to all the patients who participated in the study.
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.