
Abstract
Background:
The aim of this case study was to identify the effect of a powered stance control knee ankle foot orthosis on the kinematics and temporospatial parameters of walking by a person with poliomyelitis when compared to a knee ankle foot orthosis.
Case description and methods:
A knee ankle foot orthosis was initially manufactured by incorporating drop lock knee joints and custom molded ankle foot orthoses and fitted to a person with poliomyelitis. The orthosis was then adapted by adding electrically activated powered knee joints to provide knee extension torque during stance and also flexion torque in swing phase. Lower limb kinematic and kinetic data plus data for temporospatial parameters were acquired from three test walks using each orthosis.
Findings and outcomes:
Walking speed, step length, and vertical and horizontal displacement of the pelvis decreased when walking with the powered stance control knee ankle foot orthosis compared to the knee ankle foot orthosis. When using the powered stance control knee ankle foot orthosis, the knee flexion achieved during swing and also the overall pattern of walking more closely matched that of normal human walking. The reduced walking speed may have caused the smaller compensatory motions detected when the powered stance control knee ankle foot orthosis was used.
Conclusion:
The new powered SCKAFO facilitated controlled knee flexion and extension during ambulation for a volunteer poliomyelitis person.
Clinical relevance
The powered stance control knee ankle foot orthosis has the potential to improve knee joint kinematics in persons with poliomyelitis when ambulating.
Background
Knee ankle foot orthoses (KAFOs) are used by patients suffering from anterior poliomyelitis, but patients must walk with an abnormal and noncosmetic gait pattern with the knee locked in extension, and also with increased upper-body lateral sway, vaulting, hip hiking, or leg circumduction when compared to normal walking. 1 Walking with the knee locked in extension has been shown to cause a reduction of 24% in gait efficiency; 2 increased vertical displacement of the center of mass by 65%; 3 and increased energy consumption and also fatigue, which consequently results in high rejection rates by this group of patients.2,4
Stance control knee ankle foot orthoses (SCKAFOs) are designed to hold the knee locked in extension at specific points during stance phase while reducing limb length during swing via knee flexion. However, controlled knee flexion during loading response and pre-swing, knee extension assistance, and smooth switching between stance and swing modes remain challenges for future designs. 5
Powered lower limb orthoses have been shown to be useful devices for aiding walking for patients with spinal cord injury (SCI), stroke, or poliomyelitis. 6 These devices restore a portion of the torque that is applied normally to the lower limb joints during walking. 7 This study extended this technology to enable it to be potentially incorporated in a new knee joint mechanism for use in SCKAFOs. This study was designed to evaluate the effect of a new powered knee joint mechanism on a single KAFO-user’s gait to determine the extent to which the new orthosis would correct KAFO-induced gait abnormalities when compared to normal gait.
Case description and methods
Participant
A 54-year-old male subject (weight = 68 kg and height = 168 cm) suffering from poliomyelitis volunteered for this study. He had previously routinely used a locked knee KAFO for 47 years for ambulatory purposes for his right leg. His upper extremity function was normal, but he had a flaccid right knee and ankle, with muscle atrophy and no voluntary movement in these joints. The muscle strengths and joint ranges of motion in the left leg were normal. 8
Powered knee joint design
A brushless EC electromotor (EC30; Maxon Motors Co. Ltd, Switzerland) coupled with planetary gearbox (reduction ratio of 110:1) was utilized for supplying the required torque via a linkage mechanism. The orthosis structure weighed 2.8 kg. One rechargeable 24 V battery (Li Po Battery, Thunder Power RC G6 Pro Lite 25C 5400mAh 6-Cell/6S) was used as power supply and placed on a waist belt with a lead passing to the knee joint to apply a constant power source. The additional components of the powered SCKAFO added 0.8 kg of extra weight, and widened the knee joint to 33 mm both mediolaterally and anteroposteriorly (Figure 1).
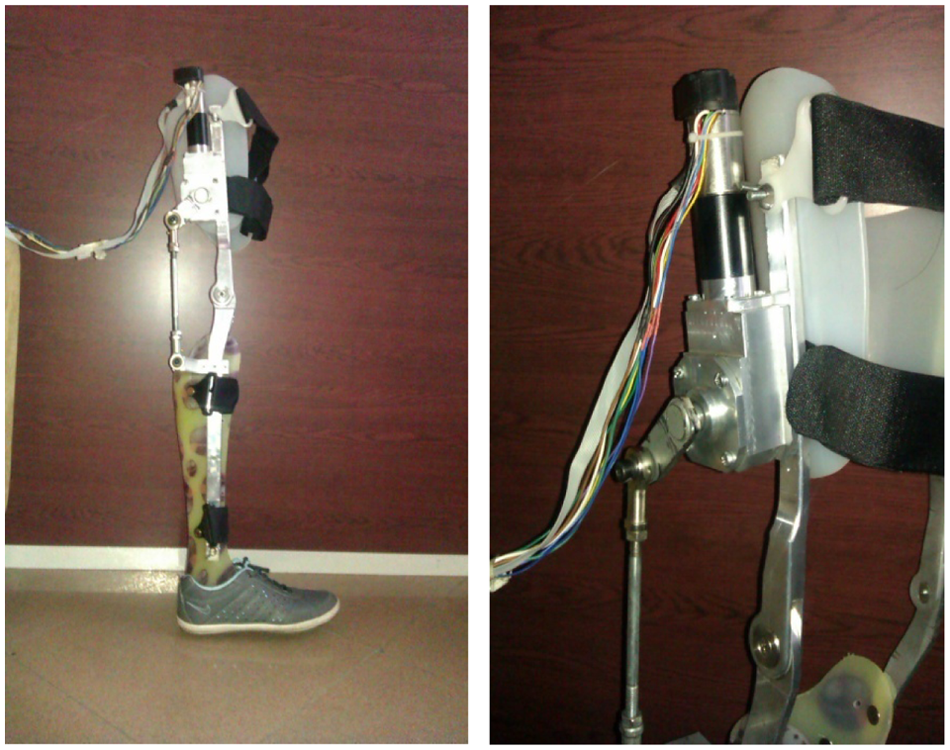
The new powered SCKAFO used in this study. Pictures show the knee actuator and its mounting place.
A load cell mounted underneath the heel of the healthy side was used to initiate motion using a controller, which was programmed to start when the weight fully transferred onto the healthy foot. This enabled the powered knee to flex during mid-swing and then extend during late swing phase. In order to move the powered knee to 50° of flexion, 8 N m of torque was applied by the actuator. The alteration from flexion to full extension for initial contact took approximately 0.4 s. When the load cell has been unloaded, it means weight has been transferred onto the disabled leg and power will be applied to the joint via the main control board to facilitate swing phase.
During full knee extension prior to heel strike, a constant torque of approximately 1 N m was applied, which was abruptly increased to 18 N m at heel strike in order to compensate for the heel strike moment applied by the ground reaction force (Figure 2). The knee was actively locked in an extended position from heel strike to toe off by controlling the current supplied in reaction to any changes of knee position.
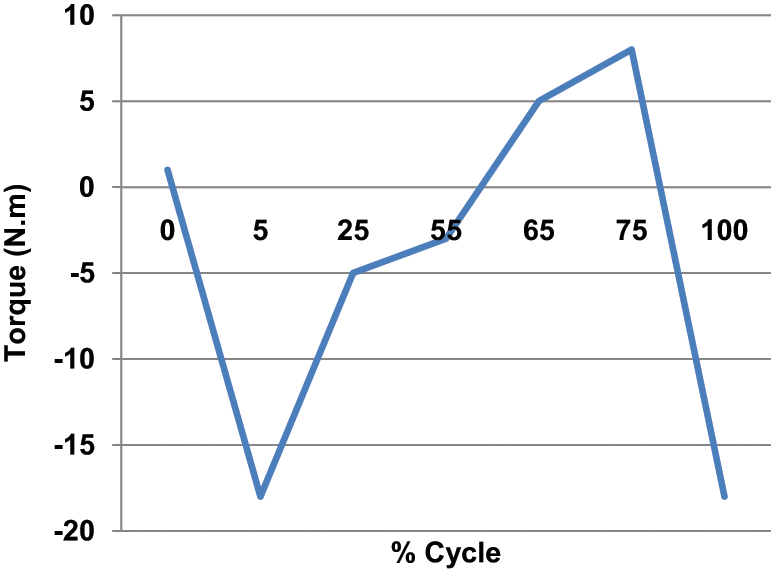
Applied torque during a gait cycle.
Analysis procedures
A calibrated 6-camera Vicon 370 motion analysis system (Oxford Metrics, UK) with a frequency of 100 Hz was used to collect lower limb kinematics via reflective markers placed as per the Helen Hayes model on the uprights of the orthosis as close as possible to the considered points.
The person with poliomyelitis used the KAFO with powered knee joints for walking therapy and gait training 2 months prior to the gait analysis, and walked three times when wearing the KAFO first before being adapted with the actuator. Before participation in the study, the subject read and approved a statement acknowledging informed consent. The ethics committee of the University of Social Welfare approved performance of this study.
Findings and outcomes
Walking with the new orthosis resulted in a mean slower walking speed and shorter stride length compared to walking with the KAFO (Table 1). The vertical and horizontal compensatory motions, evaluated from the trajectory of markers placed on both anterior superior iliac spines (ASIS), both also decreased as demonstrated in previous studies.9–11
Spatiotemporal parameters with the orthoses (±SD).
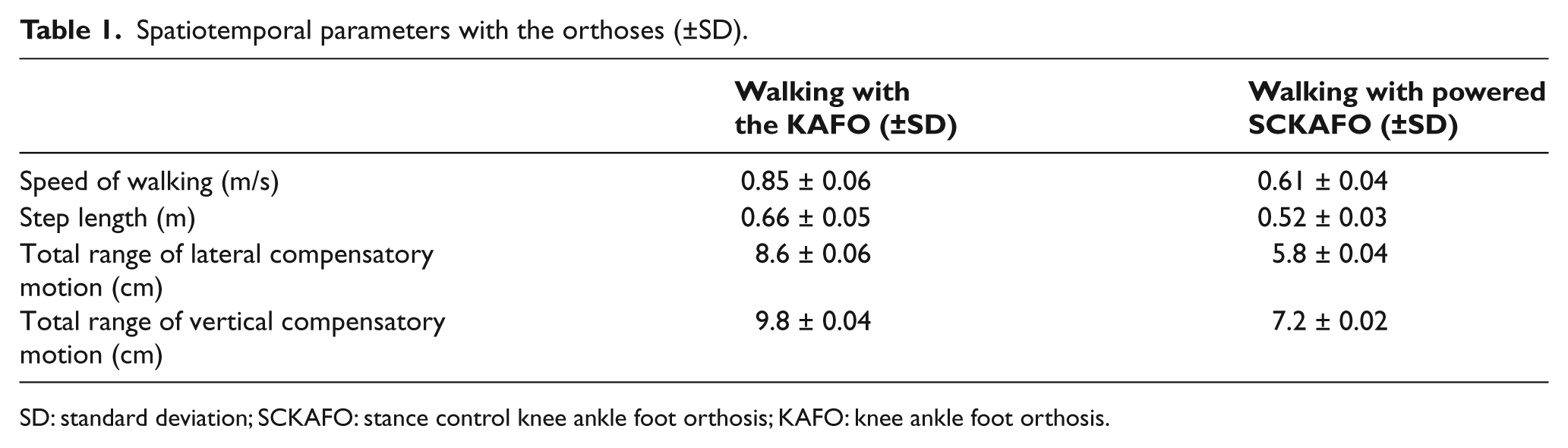
SD: standard deviation; SCKAFO: stance control knee ankle foot orthosis; KAFO: knee ankle foot orthosis.
At mid-swing, the SCKAFO knee joint flexed to a maximum of 42.5° ± 1.8° compared to 7° ±1.6° when walking with the KAFO with drop locked knee joints (Figure 3). During stance, very little flexion was achieved (lower than the normal 20°). However, at pre-swing, knee flexion provided by the actuator was similar to the angle demonstrated during normal walking but slightly later than normal. This knee flexion lag was negated at the point of mid-swing, where the knee flexion angle increased to 42.5° ± 1.8°. The “knee flexion lag” in early swing was due to the control method, which only flexed the knee when maximal weight was transferred to the unaffected limb. For optimal gait, knee flexion needs to be initiated before full weight transfer to the contralateral lower limb. This knee flexion delay therefore adversely affected toe clearance during early swing on the affected leg. The subject who volunteered for this study had used a KAFO with drop locked knee joints for 47 years, and 2 months of gait training proved to be too short a time for being able to adapt his walking pattern to transfer his full weight onto the unaffected limb and to provide a more normal gait pattern with the new system.
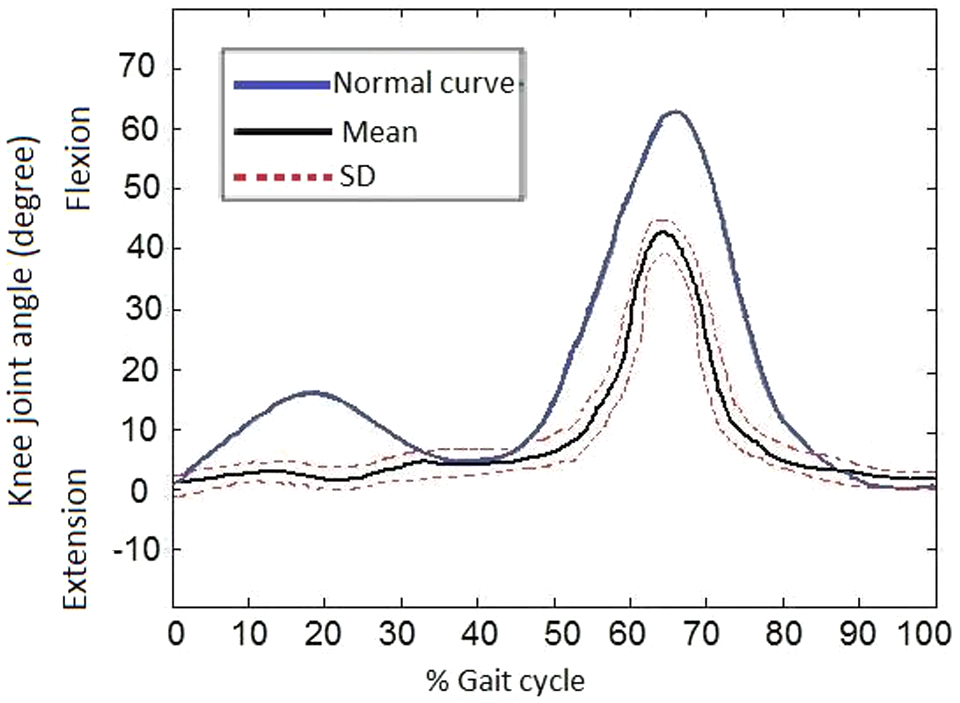
Flexion and extension of knee joint for the person with poliomyelitis walking with powered SCKAFO compared to normal walking curve.
Discussion
Increased knee flexion was produced when walking with the powered SCKAFO compared to the KAFO (mean of 42.5°), which was similar to that previously reported (44°) when walking with a SCKAFO.1,4,12–13 When knee joint movement was improved, hip compensatory motions also improved in walking with new powered SCKAFO. Yakimovich et al. 14 observed similar results in improving pelvic obliquity of hip joint. McMillan et al. 1 demonstrated smoothness of pelvic movement when patients walked with a SCKAFO, while Irby et al. 13 reported a decrease in the range of motion in pelvic obliquity when walking with SCKAFO.
Reduction of lateral and vertical compensation motion may have been caused by the demonstrated reduction in gait velocity when wearing the new powered SCKAFO compared to the KAFO. 15
The speed of walking and step length both decreased with the powered SCKAFO compared to the KAFO with drop locked knee joints. A similar result has been reported for person with poliomyelitis walking with a SCKAFO.13–14 However, McMillan et al. 1 observed that the speed of walking and stride length increased and compensatory motions were reduced when persons walked with a Horton SCKAFO compared to a KAFO with fixed knee joints.
The slower speed of walking and shorter step length as compared to the conventional KAFO in this study was caused by the concentration needed for control of the new powered KAFO, even though the patient had received appropriate gait training. Further improvements to the control strategy should be performed to increase the ability of a person with poliomyelitis to control this type of orthosis.
Further evaluation of this new orthosis on a further cohort of patients and longer training periods for walking with this orthosis is planned, along with improvements in knee joint bulk and weight, as well as development of a more advanced control software design. One limitation was that energy consumption was not measured when using the two orthoses in this study.
Key findings
In this article, the new powered SCKAFOs were used for walking by a person with poliomyelitis;
Controlled knee flexion and extension during ambulation was facilitated by a new powered SCKAFO for a volunteer person with poliomyelitis;
The person’s gait was better than when walking with a locked knee, but the outcomes were not better than nonpowered SCKAFO outcomes in the literature.
Conclusion
The new powered SCKAFO facilitated controlled knee flexion and extension during ambulation for a volunteer poliomyelitis person and also demonstrated a reduction in compensatory displacements compared to walking with a conventional KAFO.
Footnotes
Conflict of interest
The authors have no conflict of interest in this study.
Funding
This research received no specific grant from any funding in the public, commercial, or not-for-profit sectors.