
Abstract
Background and Aim:
The physical asymmetries associated with a prosthesis raises the question of validity of the Sensory Organization Test (SOT) measures (equilibrium score (ES) and strategy score (SS)) in lower limb amputees. This study explores the validity of these measures in transtibial amputees by correlating with their corresponding centre of pressure (COP) excursion/velocity measures.
Technique:
Fifteen transtibial amputees (69.5 ± 6.5 years) completed three trials for each of the six SOT conditions.
Discussion:
The Spearman’s rank correlation coefficients between ESs and global COP excursion/velocity measures ranged from 0.52 to 0.71 for Conditions 1, 4 and 5, 0.79 to 0.85 for Conditions 2 and 3, and 0.39 to 0.43 for Condition 6. The coefficients for SSs ranged between 0.78 and 0.97 for Conditions 1 to 5 and 0.55 to 0.67 for Condition 6. The corresponding sound and prosthetic side COP variables demonstrated varying strengths of association with ES and SS.
Clinical relevance
Of the two clinical measures examined, the SSs are strongly reflective of COP excursion/velocity measures and these findings have application in the interpretation of SOT when evaluating balance in transtibial amputees.
Background and Aim
The Sensory Organization Test (SOT) supported by the NeuroCom Equitest® is an objective tool used to assess balance under a range of sensory testing conditions. 1 The SOT comprises a series of six different standing balance testing conditions with eyes open and closed on a fixed/movable platform with a visual screen. In doing so this test effectively challenges each of the somatosensory, visual and vestibular systems and analyses the subject’s ability to adapt when information from one or more of these systems is unavailable or inaccurate. 2 The six SOT conditions and the respective sensory systems they solicit are as depicted in Figure 1.
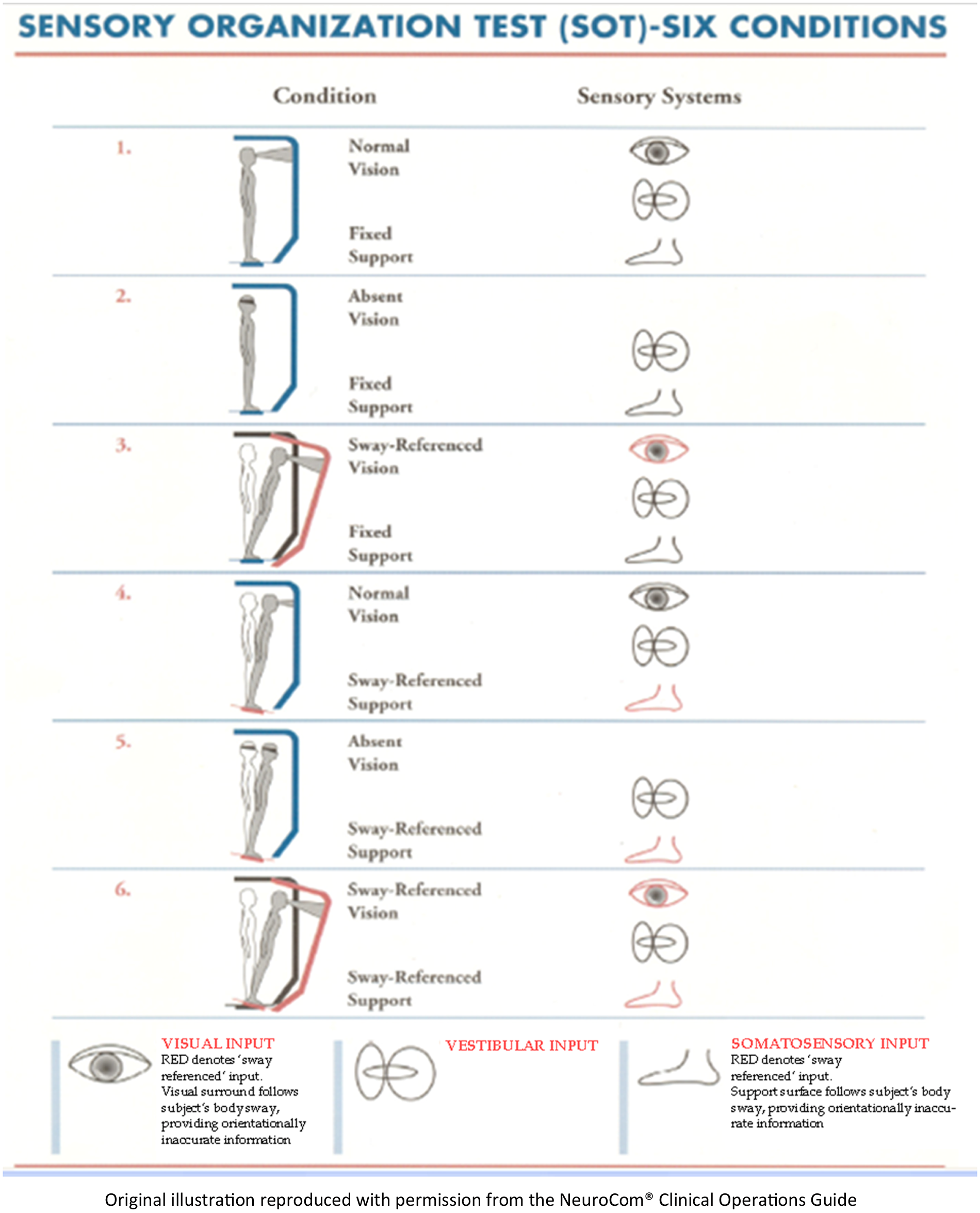
The six conditions of the Sensory Organization Test.
The customised outcome measures of the SOT are the equilibrium score (ES) and the strategy score (SS) both of which have applicability when evaluating balance performance in lower limb amputees. 3 The ES is reflective of how well the subject will stay within a theoretical sway envelop of 12.5 degrees whereas the SS indicates the dominant postural strategy employed as to whether an ankle (SS=100) or hip strategy (SS=0) is employed in a given SOT test condition. 4 Both the ES and the SS are derived from the centre of pressure (COP) trajectories of the raw data 1 and are based on the underlying premise that in the healthy physiological balance response both of these measures should closely align with the antero-posterior (AP) COP trajectories and time domain measures. 2
In persons with a transtibial amputation the ankle on the prosthetic limb is considered to be a stiff insensitive component of the kinematic chain which impacts directly on the COP variables and temporal loading patterns. 5 Despite the SOT having been used to measure balance performance in amputees in the past3,6 its use is queried on the basis of marked physical and postural asymmetry characterized by increased medio-lateral sway and asymmetric weight bearing. 5
Therefore this study aims to determine the concurrent validity of the ES and the SS measurements when compared with the conventional COP variables computed from the raw data of the same test protocol. The study also seeks to determine if the association differs between the prosthetic and sound side variables of the person with a lower limb amputation.
Technique
Participants aged 45 years or older with a unilateral transtibial amputation were recruited from the local artificial limb centre. The criteria for inclusion into the study were that the participant should have completed their formal rehabilitation, be able to walk for at least 500 m without any support and be free from any residual limb problems such as skin lesions and/or phantom limb pain. The protocol was approved by University of Otago Human Ethics Committee.
The NeuroCom SMART Equitest® version 8.4.0 was used to administer the SOT. In addition to the customised outcome measures the system also provided data corresponding to the raw force platform signals from the left and right force plate and the global measure (right and left force plate combined). The variables derived from these raw force platform data were antero-posterior (AP) COP excursion (cm) and velocity (cm/s) for the individual limbs (sound and prosthetic) and global measure. 1 The default sampling frequency of the Equitest® force platform was 100 Hz and prior to analysis the COP measures were digitally low pass (10 Hz) filtered using the zero lag fourth order Butterworth filter. 7
As the ES and SS measures were derived from the AP COP values, 4 the AP-COP (excursion/velocity) measures were used for the purposes of this analysis. Higher values of the ES and SS imply relatively better balance performance whereas higher COP excursion and velocity is reflective of poor balance performance. Hence negative correlations between the two sets of measures were anticipated within this context.
After obtaining written informed consent, all participants were screened with a questionnaire to determine their age (years), duration of prosthetic use (years) and body mass index (kg/m2). Participants then completed three trials for each of the six SOT conditions (Figure 1). The conditions were administered sequentially from simple to complex (Conditions 1 to 6). Descriptive statistics (mean and standard deviation (SD)) were determined for the anthropometric data and for the key outcome variables based on the mean of the three trials.
Spearman’s rank correlation coefficients (r s ) were used to determine the relationship between the clinical measures and the force platform measures (AP-COP excursion and velocity). The criteria to determine the strength of the correlations 8 was as follows; r s ≤ 0.25 = little or no relationship; r s = 0.25 -0.50, fair; r s = 0.50-0.75, moderate to good and r s ≥0.75, good to excellent relationship.
Results and Discussion
Fifteen transtibial amputees with a mean (SD) age of 69.53 (6.59) years and mean duration of prosthetic use of 11.94 (13.92) years participated in the study. The mean body mass index of the participants was 27.3 (6.4) kg/m2. Seven participants had undergone amputation due to a dysvascular condition while in eight persons it was due to a traumatic cause. The descriptive statistics for the clinical and force platform measures are given in Table 1.
Descriptive statistics (mean (SD)) of the equilibrium score (ES), strategy score (SS) and antero-posterior centre of pressure variables (global, sound, prosthetic side).
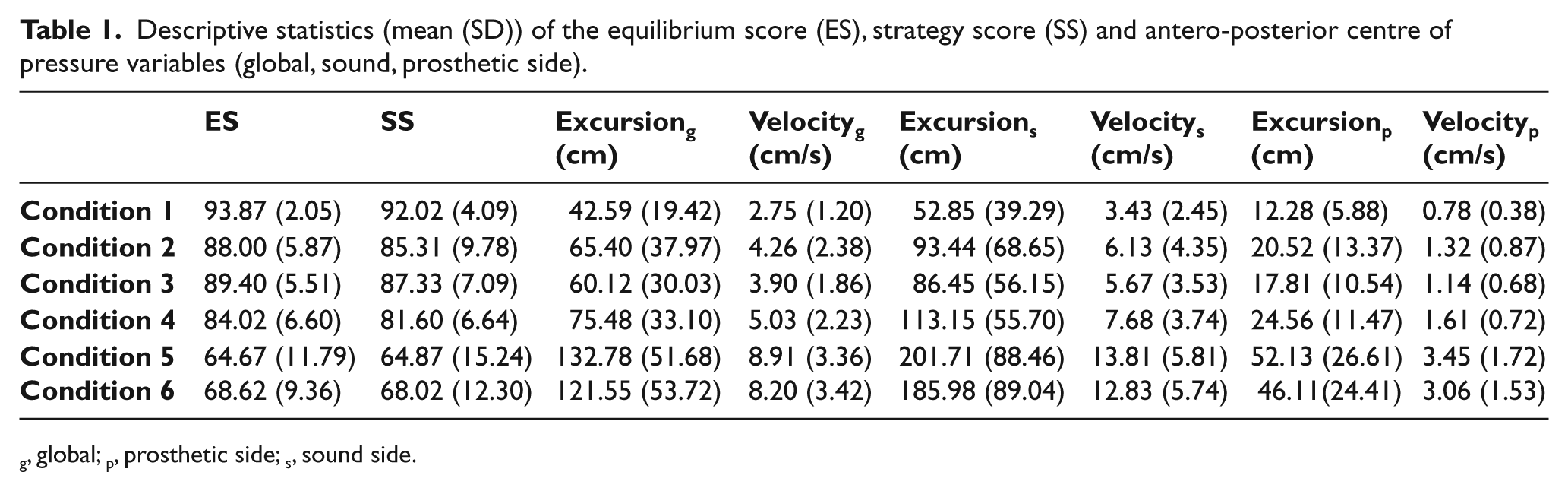
g, global; p, prosthetic side; s, sound side.
The Spearman’s rank correlation coefficients (Table 2) between the ES and global COP excursion/velocity were ‘good to excellent’ for Conditions 2 and 3, ‘moderate to good’ for Conditions 1, 4 and 5, and ‘fair’ for Condition 6. The SS demonstrated ‘good to excellent’ correlation with the global COP excursion and velocity variables for conditions 1 to 5 and ‘moderate to good’ relationship for Condition 6.
Spearman’s rank correlation between the equilibrium, strategy scores of six Sensory Organization Test conditions (C) and their respective antero-posterior centre of pressure variables (global, sound, prosthetic side).
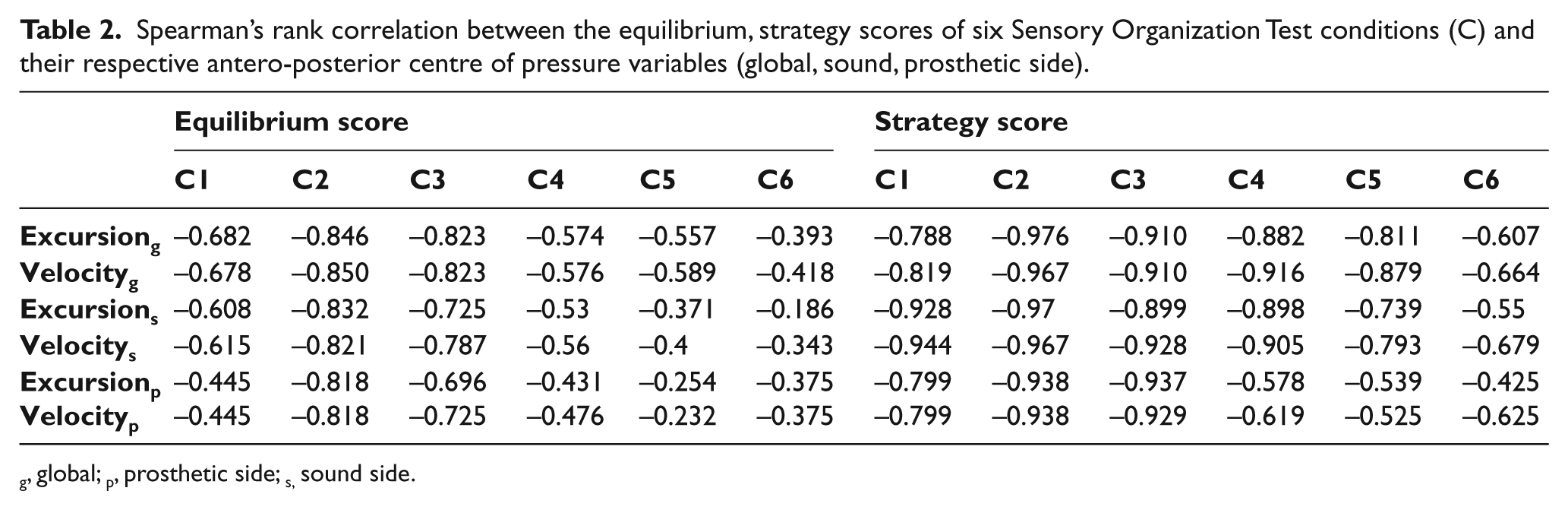
g, global; p, prosthetic side; s, sound side.
The comparison of prosthetic and sound side COP variables (excursion and velocity) with the ES and SS demonstrated varied strengths of association. The prosthetic side had ‘little’ or ‘fair’ association with the ES on Conditions 1, 4, 5 and 6 while with SS had demonstrated ‘good to excellent’ on Conditions 1, 2 and 3 and, ‘fair to good’ on Conditions 4, 5 and 6. The sound side coefficients with SS were ‘good to excellent’ on all conditions except 6; whereas the ES had demonstrated ‘good to excellent’ association with sound side variables only on Conditions 1, 2 and 3.
The investigation revealed a strong relationship between the SS and the global AP-COP measures (excursion/velocity) of transtibial amputees for most conditions but a similar relationship was not found for the ESs. This result is in contrast to a previous investigation in healthy young adults which reported the ES as a valid measure when compared with the sway area obtained from the force plate data. 9 These authors demonstrated high correlation coefficients, 9 although sway area is a combined measure of the AP and medio-lateral sway whereas the ESs and SSs were derived from the AP sway.
The computation of ES is described as the estimation of the individual’s performance with respect to a predetermined AP sway (12.5°) of healthy control subjects. 4 In healthy people, the muscles around the ankle work to restore the postural stability for subtle perturbations (ankle strategy) and muscles around the hip and trunk muscles work during larger perturbations. 10 In persons with a lower limb amputation the muscles of the sound side ankle may work to restore postural stability, whereas on the prosthetic side muscles above the level of amputation 11 and/or the torque modulated by the stiffness of the prosthetic foot, 12 are required to negotiate the dynamic situations such as during platform perturbation. This structural and functional asymmetry owing to the prosthetic ankle and foot raises the question of validity of the ES and SS that are derived from the comparison with healthy adults. The difference in the strength of associations between the prosthetic and sound side with the ESs of all conditions also support this hypothesis.
Interestingly ES demonstrated a weak correlation with the COP variables on a simple condition (Condition 1) when all three (visual, vestibular and somatosensory) sensory systems were available and strongest correlation on Conditions 2 and 3 when the visual input was absent or manipulated. This suggests that an alternative postural adaptation takes place in amputees when all three sensory systems are available but a postural strategy similar to the healthy adults occur when the visual input is altered.
The strongest association was identified between the SS and AP-COP in Conditions 1 to 5 across global, sound and prosthetic measures. These can be taken to be indicative of effective postural strategies closely approximating healthy subjects. The coefficient (‘fair to good’) for the prosthetic side COP variables with the SSs of Conditions 4, 5 and 6 indicate that the strategy employed by the prosthetic side differs from that of the sound side and perhaps from that of the healthy adults when the somatosensory and/or vestibular input are manipulated. Collectively, the pattern of postural asymmetries identified in transtibial amputees from this study highlights the need for condition specific interpretation of the ES and SS values. Although it is acknowledged that there may have been underlying differences in balance performance between the dysvascular and traumatic amputees the small sample used in this study did not permit any sub-group analysis.
A limitation of this study is modest sample size for a validity design and the results are to be interpreted with due caution. Nevertheless they suggest that future studies designed to determine the content and construct validity of the SOT measures in lower limb amputees are necessary to support its clinical utility.
Key points
The SS variable of the SOT is a valid measure of balance performance in transtibial amputees when compared with the AP-COP measures derived from the corresponding force platform measures.
The ES is reflective of the AP-COP measures in transtibial amputees for only two of the six SOT test conditions in which the somatosensory and/or vestibular systems are directly challenged.
The strategy employed by the prosthetic side is different from that of the sound side with altered somatosensory and/or visual input.
Footnotes
Acknowledgements
The authors would like to thank the Dunedin Artificial Limb centre staff for helping in the recruitment of participants. The authors also thank Bruce Knox for his technical support in processing the force platform data.
Funding
This work was funded by the New Zealand Artificial Limb Board, Wellington, New Zealand [grant number: PL10674001PLX].
Conflict of interest
The authors declare that there is no conflict of interest