
Abstract
Background:
There is a lack of data and consensus concerning the most appropriate functional evaluation in clinical practice at the definitive prosthetic phase after lower limb amputation.
Objectives:
To determine among several selected functional tests the most pertinent to evaluate balance and prosthetic walking.
Study Design:
Validation of a diagnostic procedure.
Methods:
Sixty-four patients were included. Outcome measures: Timed Up and Go test, Functional Reach test (FRT), one-leg balance, tandem test, Modified Houghton Scale, Berg Balance Scale, two-minute walk test (2MW test). Correlations were assessed with the Pearson correlation coefficient and the Principal Component Analysis. Score distribution was analyzed with the Shapiro-Wilk W normality test. Receiver operating characteristic curves were drawn to identify the best predictor for the function.
Results:
The clinical tests correlated highly with each other. Only 2MW test and FRT did not have either a floor/ceiling effect, or a bi-modal distribution. The 2MW test was the best predictor of prosthetic walking limitations (area under the curve 0.93 (0.83–0.97), the best threshold was between 130 and 150 meters), and FRT was best for balance.
Conclusions:
2MW test can be proposed as the first-line clinical test. The FRT can be indicated for the specific assessment of balance disorders.
Clinical relevance
This validation of a clinical evaluation of balance and walking capacity after lower limb amputation may be useful in everyday practice to ensure in a simple and standardized way the follow-up of patients and adapt treatments – especially prosthetics – at the definitive prosthetic phase.
Background
After lower limb amputation, the principal objective is to restore independent prosthetic walking and to enable patients to return to prior activities in optimal conditions of safety and comfort. The initial management of amputees as inpatients in a rehabilitation unit is recommended, since it ensures considerable gains in the recovery of walking ability, morbidity and mortality. 1 When the patient has completed this initial phase of rehabilitation, it is necessary to evaluate balance and walking capacity in accordance with the International Classification of Functioning. 2 This functional assessment is justified in clinical practice to quantify the true abilities of the patient in terms of walking autonomy, and to search for factors that limit prosthetic walking. Among these factors, balance disorders play an important role. 3 Indeed, amputation causes a deficit in the proprioceptive information that normally interacts with vestibular, visual and somatosensory systems of regulation. 4 These balance disorders may be exacerbated in the frequent context of senescence and cerebrovascular disease.
Despite numerous proposed clinical tests there are currently no recommendations concerning the most appropriate one at the definitive prosthetic phase. This situation has led to huge variety in measurement methods in rehabilitation units, making it impossible to compare the results of interventions in this population. 5
The principal objective of this study was to select one or more outcome assessment tools to provide a quantified evaluation of balance and walking capacity that is currently applicable (without expensive technology) for every adult amputee stabilized with regard to the prosthetic fitting. The choices had to:
be made from the outcome measures considered pertinent by experts in balance and the rehabilitation of amputees;
be compatible with use in everyday clinical practice;
preclude the use of expensive equipment, notably gait assessment instruments such as biomechanical or kinematic devices 6 ;
be applicable to any amputee, regardless of the age, the aetiology, the level of amputation (transfemoral or transtibial amputation) and the type of prosthesis.
A review of the literature, conducted by a group of clinicians specialized in rehabilitation for patients with lower limb amputation and in balance disorders was carried out on MEDLINE databases with the keywords: lower limb amputation, functional evaluation, balance assessment, survey of lower limb amputation and prosthetic walking. This analysis led to the selection of six clinical scales and one questionnaire to evaluate balance and prosthetic ambulation. The first three scales more specifically explored balance.
The Berg Balance Scale comprises 14 items at five levels of score (total ranging from 0 to 56), and evaluates the ability to maintain balance in different situations. 7 It is the most widely used postural scale in balance disorders 8 and shows good intra- and inter-examiner reproducibility. 9 Significant correlations have been found with instrumental studies of posture.10,11 It has already been used in active amputees.12,13
The Functional Reach test (FRT) consists in measuring the distance covered by the horizontally outstretched arm when patients move from the vertical standing position to the maximum lean forward position, with the feet firmly placed on the floor. 14 Its reproducibility is reasonable, and it is inversely associated with the risk of falling in frail elderly patients. 15
One-leg balance on the unaffected limb has been applied in the follow-up of amputations with the following categories: not able to stand on one leg; able to stand on one leg with support, able to stand on one leg without support ≤10 seconds; able to stand on one leg without support >10 seconds. 16 As in this study, patients were evaluated in the medium term after the amputation, the test was modified with regard to the duration of balance without support. A tandem test was associated: duration of full-tandem stance, with the amputated limb behind. In the medium term following amputation, this test significantly correlates with the quality of prosthetic walking in subjects aged over 60 years. 17
The 2MW test measures the distance covered by the patient in two minutes at the self-selected walking speed. It correlates significantly with the six- and 12-minute walk test from which it is derived. 18 The main advantage is that it is shorter and thus more appropriate for patients with severe disabilities. In amputees, it is feasible, sensitive to changes linked to rehabilitation and correlates with physical ability and the use of the prosthesis. 19 The patient is asked to cover the greatest possible distance in two minutes on a marked indoor track, without encouragement. Pauses are authorized. An assistant follows the subject, remaining behind. The patient uses his usual assistive device (crutches, walker . . .). The average walking speed can thus be calculated (ratio of the distance covered and of the duration of two minutes. m/s). It corresponds to the free walking speed (or comfortable walking speed), which reflects the greatest bioenergetic efficiency of walking, that ranges from 0.90 to 1.60 m/s in healthy adults. 20
The Timed Up and Go (TUG) test was initially proposed to evaluate balance in elderly subjects 21 ; the TUG test was later timed. It identifies elderly subjects with a risk of falling, and as such was validated in patients amputated for vascular disease.10,22,23 In transtibial amputees it distinguishes between multiple fallers (TUG test above or equal to 19 seconds) and non-multiple fallers. 24
The Modified Houghton Scale is a questionnaire that evaluates the perceived use of the prosthesis in everyday life. 25 This score includes five items: daily duration of prosthesis use; walking indoors and outdoors; walking aids indoors and outdoors; abilities in different situations (standing up from a chair, stairs, different surfaces, carrying objects). The reliability, validity and responsiveness to change of this score have been confirmed. 26 A slightly modified French version has been validated.27,28
Methods
Participants
Participants were screened for eligibility in the medium term after their amputation, that is to say, after they had returned home with their definitive prosthesis. They had all been managed in the same university hospital’s rehabilitation centre during the immediate follow-up of their amputation to be equipped with a temporary prosthesis. Participants were included if:
they were more than 20 years old (to include only adult patients sufficiently later than the period of growth during adolescence);
they had undergone unilateral transtibial or transfemoral amputation;
they had been equipped with the definitive prosthesis;
at least five months had passed since the amputation surgery;
they were able to perform an TUG test autonomously, i.e. patients able to get up from a standard arm chair (seat height: 46 cm, arm height: 67 cm), cover a distance of three metres, and turn round to sit down again, 21 with the usual prosthesis and without the help of another person, whatever the device to assist walking.
The aetiology of the amputation, whether vascular, traumatic, congenital or tumoral, was not among the inclusion criteria. Participants were excluded if:
they presented cognitive troubles that hampered understanding and participation in the tests (Mini-Mental State Examination ≤23) 29 ;
there had been a modification in prosthetic fitting during the preceding three months to be sure that the conditions of prosthetic walking were stable: the objective of this study was to validate an outcome measure at the definitive phase of fitting, not at the early stage.
Pain and/or other deficits, such as neurological or orthopaedic disorders, associated with the amputation, were not a reason for exclusion, provided that they were compatible with the TUG test. All subjects gave their written consent after being clearly advised about the protocol, which was approved by the institutional ethics committee.
Study procedure
In order to simulate the conditions of everyday practice, neither the 2MW test nor the TUG test were preceded by a trial run. Concerning the chronology of the tests, the TUG test was performed first, so as to make sure that the patient had the minimal abilities to allow inclusion. The FRT, the one-leg balance on the unaffected limb, the tandem test, the Modified Houghton Scale, the Berg Balance Scale, and finally the 2MW test were successively performed (without randomization) to limit the consequences of fatigue on balance regulation. The patients were allowed to use their usual walking aids (crutches, walker) so as to be in their usual conditions of walking. All of the tests were carried out under the control of three physicians specialized in physical medicine with experience in the rehabilitation of amputees and the evaluation of gait disorders.
Statistical analysis
For all gait and posture variables, averages and standard deviations were computed. In order to detect particular patterns in values (i.e. floor or ceiling effects), the shape of the distribution was drawn and the Shapiro-Wilk W normality test was run for each variable. Relationships between clinical variables were tested with Pearson’s correlation coefficient, Principal Component Analysis (PCA), and receiver operating characteristic (ROC) curves. PCA is a data analysis tool whose aim is to study relationships between clinical variables all at once. It computes independent factors which are a weighted average of the original variables. In our study, variables that correlated highly with a particular factor (high ‘factor loading’) are supposed to assess the same aspect of balance and are more or less redundant. Patients were divided into two groups, according to the Modified Houghton Scale: no limitation of walking capacity (score = 20) and existence of incapacity to walk, whatever the degree of severity (score <20). Then ROC curves were used to compare the performance of the six clinical scales in predicting the presence of functional limitations and to determine their appropriate cut-off values. NCSS 2000 was used for all statistical analyses (Hintze J. NCSS (Number Cruncher Statistical System) 1997: Atlanta, USA).
Results
Seventy unilateral amputees older than 20 years old were initially contacted. Among them, three were excluded because they were unable to perform the TUG test, two because of recent modification of the prosthesis, and one because a contralateral amputation was planned. Finally all of the 64 patients screened agreed to take part in the study. Their characteristics were as follows: 54 (84%) males and 10 (16%) females, aged between 22 and 87 years (mean age ± SD, 58 ± 16 years), body weight 42 to 110 kilograms (mean weight ± SD, 74.1 ± 13.9 kilograms), 47 (73%) transtibial amputations and 17 (27%) transfemoral amputations. The reason for the amputation was vascular for 42 (66%) patients, traumatic for 16 (25%), infection for three (5%), cancer for two (3%) and congenital for one (<1%). The time since the amputation was two to 360 months (mean time ± SD, 33 ± 54 months, median 13 months).
For the whole group of patients, the mean walking speed was 0.86 ± 0.41 m/s. Gait speed was slower in transfemoral than in transtibial amputees (0.74 ± 0.38 versus 0.91 ± 0.42m/s), but the difference was not significant.
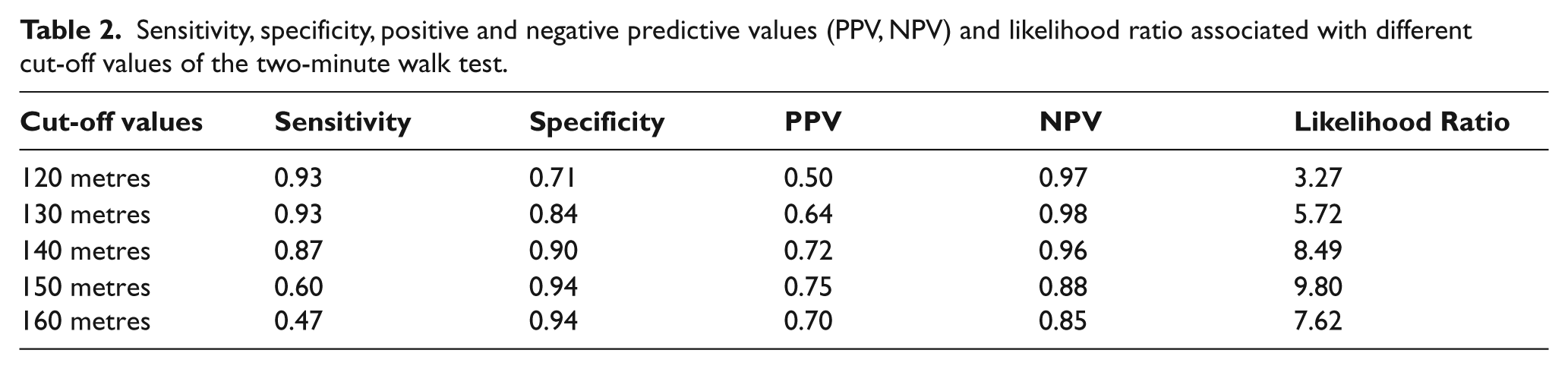
Mean scores for gait and balance scales are reported in Table 1. Fifteen patients (23%) had no functional limitation, according to the Modified Houghton Scale (score = 20/20). The area under the ROC curves and the 95% confidence limits of the six clinical tests are reported. From this point of view, the best test was the 2MW test. Cut-off values between 130 and 150 meters were associated with satisfactory values for sensitivity, specificity, positive and negative predictive values and likelihood ratios (Table 2).
Mean scores for all tests.
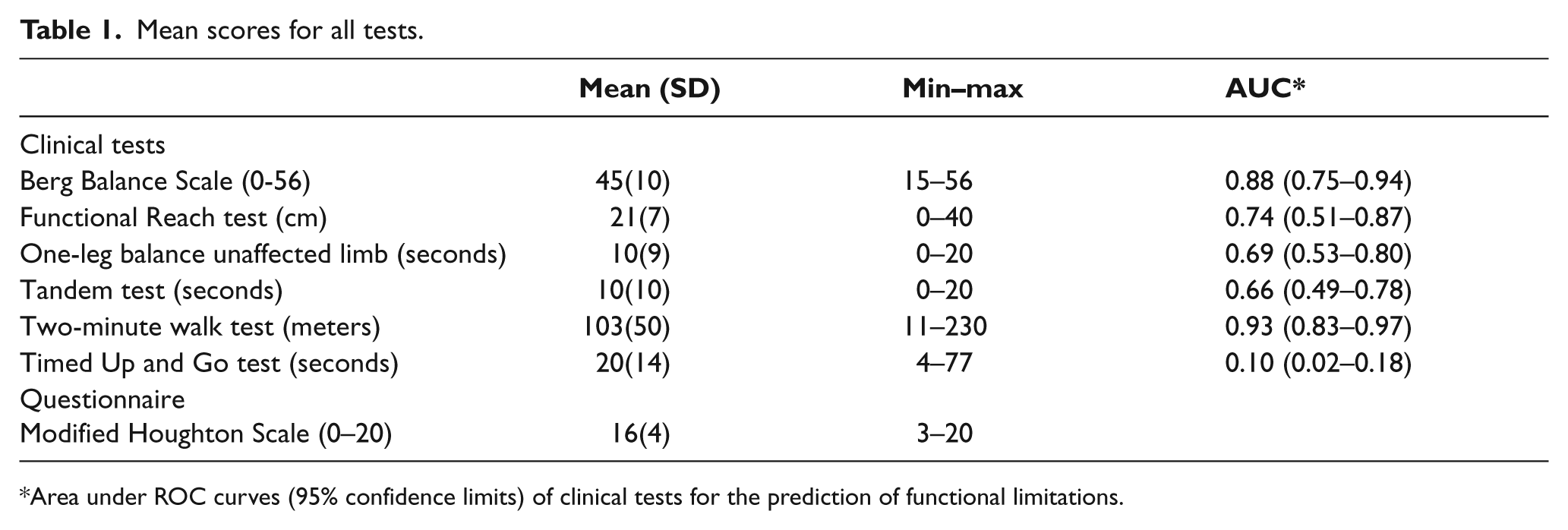
Area under ROC curves (95% confidence limits) of clinical tests for the prediction of functional limitations.
Sensitivity, specificity, positive and negative predictive values (PPV, NPV) and likelihood ratio associated with different cut-off values of the two-minute walk test.
Normality was rejected (Shapiro-Wilk W Test) for all scores except those for the FRT and the 2MW test. As shown in Figure 1, other scores had either a floor/ceiling effect, or bimodal distribution. All gait and balance tests correlated highly with each other (r = 0.35 to 0.80, p < 10-2 to p < 10-6).
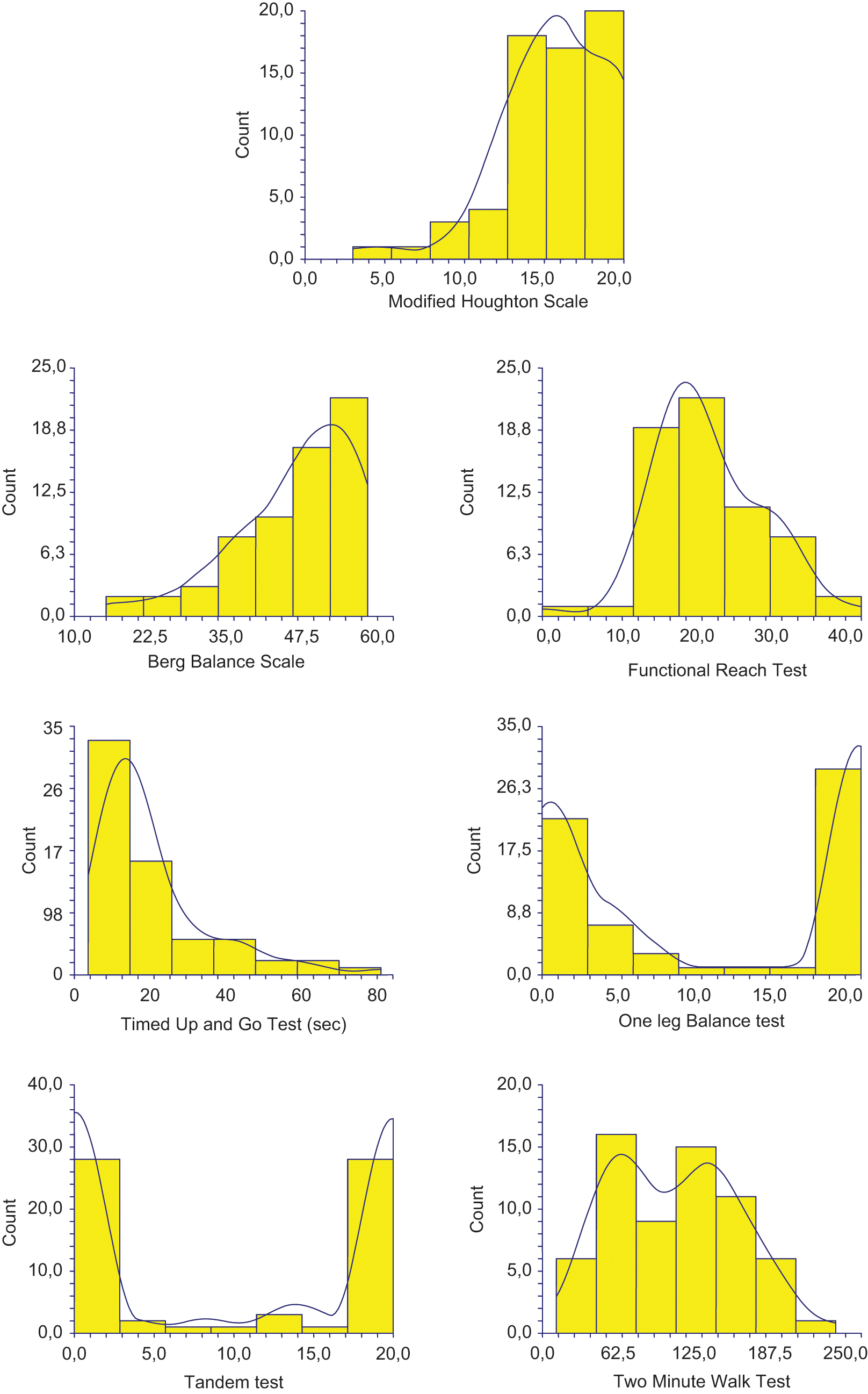
Frequency distributions of gait and balance score.
The PCA showed that three factors included 88% of the information. The three-dimensional structure, after quartimax rotation, could be described as follows, scores with the greatest absolute factor loadings (>0.80) were factor 1 (52% of the information): the Berg Balance Scale (0.81), the Modified Houghton Scale (0.92), the 2MW test (0.90) and TUG test (0.92); factor 2 (26% of the information): one-leg balance on the unaffected limb (0.87) and the tandem test (0.89); factor 3 (11% of the information): the FRT (0.84). The factor loading of the PCA (factors 1 and 2) are plotted in Figure 2. Two variables that correlate with the same factor are supposed to measure the same aspect and are more or less redundant, whereas variables that correlate with different factors are supposed to measure different aspects.
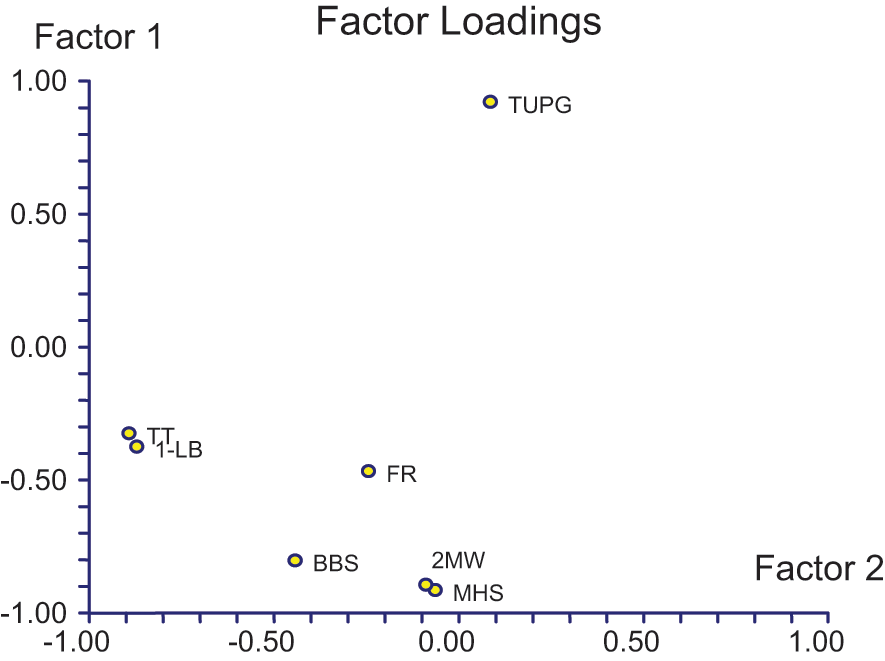
Factor loading of the PCA. Only factors 1 and 2 are plotted.
Discussion
The characteristics of this population of patients were in keeping with epidemiological data, which show a preponderance of transtibial amputations compared with transfemoral amputations, and the usual vascular etiology. 30 These findings are thus relevant to daily clinical practice. Preservation of the knee is systematically sought when amputation is necessary because the functional result is better. 31 This difference is particularly related to the lower level of energy expenditure in prosthetic walking for transtibial amputees than for transfemoral amputees. 32 The worse result in bioenergetic efficiency after transfemoral amputation was reflected in this study by a more marked reduction in walking speed. The difference, however, was not significant. This was possibly due to the relatively small size of the transfemoral amputees group. Nonetheless, if age is taken into account (slightly higher in transtibial amputees) in a multiple regression model, the impact of the level of amputation becomes statistically significant (p = 0.038), as does age (p < 10-4). The distribution of the levels of amputation, the large variance in the time since the amputation and the variety in the underlying aetiology, meet one of the objectives of this study which was to investigate a wide population of amputees, provided that all were at the stage of the definitive prosthesis, in order to reflect a ‘real life clinical setting’.
The evaluation of prosthetic walking in everyday clinical practice must be applicable to as many patients as possible, while keeping to a minimum the consumption of resources in terms of medical time and technologies. These criteria led us to choose this set of clinical tests to evaluate adult amputees, whatever their age, and whatever the cause and level of the amputation. The choice of the clinical tests used was made following a review of the literature, from a wide range of possibilities.
Particularly, in a review of the literature, 35 questionnaires that specifically evaluate prosthetic walking were identified with considerable variety in the parameters measured. 33 For the moment, it seems impossible to make a perfectly justified choice of the most appropriate score. These different scales are affected by the perceptive, cognitive and communication abilities of patients. 34 Because of this and like quality of life scores, they suffer from insufficient sensitivity, which is clearly revealed when the data are compared with the results of walking analyses measured by a step activity monitor. 35 For this study, we retained the Houghton Scale as it is the only questionnaire that has been validated in the language of the authors.27,28 It presents the interest to be a multimodal scale which investigates various activities inside and outside, depending both on balance and on walking with a prosthesis.
Concerning clinical tests that specifically assess balance, this study was, to our knowledge, the first to use the FRT in lower-limb amputees.
The distributions of all the tests but the 2MW test and the FRT were very different from the ideal bell-shaped symmetrical distribution (floor or ceiling effect, bimodal distribution). All of the tests significantly correlated with each other. The PCA identified three groups of variables (three PCA factors), which suggests that three different aspects of prosthetic walking were assessed. The first factor was supported by the Berg Balance Scale, the Modified Houghton Scale, the 2MW test and the TUG test. This first factor reflected general walking and posture performances assessed either by a clinical scale or a questionnaire. As only the 2MW test had a near-normal distribution in this group of amputees, this test seems to be the best choice among these four scales. Variables correlating with the second factor were one-leg balance on the unaffected limb and the tandem test. Their distributions were bimodal, as if they were yes/no (success/failure) tests. Like the TUG test, these tests are not sufficiently discriminating and progressive and are thus more appropriate for early evaluation in the immediate follow-up of the amputation in order to establish a prognosis for success in prosthetic ambulation. 16 The FRT alone reflects the third factor. This is probably due to its specificity in the evaluation of balance. Whereas the other tests are static, the FRT creates a forward disequilibrium that is controlled by the patient and therefore brings into play dynamic regulation mechanisms that may be affected by fear of falling.
Thus, by its psychometric and clinical properties the 2MW test seems better than the others selected tests in assessing function in amputees. Furthermore, cut-off values of 130 or 150 meters for the 2MW test were highly associated with the existence of functional limitations in daily life. In particular, the highest values of the 2MW correspond to the absence of a need for a walking aid outdoors assessed by the Modified Houghton Scale. Moreover, a recent study confirmed the good correlation between the 2MW test and ambulation performance measured by a step activity monitor in active amputees. 36 A minimal set of tests should comprise the 2MW test (first PCA factor) and the FRT (third PCA factor). A more extensive set could also include the one-leg balance on the unaffected limb or the tandem test (second factor). These, however, have limited clinical interest because like the FRT, they focus on balance.
Study limitations
Our study does have a number of limitations. First, the subjects were evaluated in the medium term after their amputation and the results were not validated at the initial phase of the rehabilitation. Of course, in the immediate follow-up of amputation, prosthetic walking is very often restricted, and tests that focus on balance, such as the one-leg balance on the unaffected limb are recommended. 16 The other important limitation concerns the patients. First of all, there were few (64) and secondly, all of the patients evaluated in this study received inpatient rehabilitation, which creates a selection bias. Moreover, they did not suffer from severe cognitive disorders, which creates a second bias. These results are therefore not applicable to the general population of amputees, in particular to patients presenting with cognitive disorders and to bilateral amputees. A new study, with more comprehensive and a more inclusive set of patients, is thus recommended. Our initial selection of seven tests could be criticized, in particular those that explore balance, given the large number of tests available. Finally, this study did not evaluate the intrinsic properties of validity of each clinical test (specificity, sensitivity to change). These were considered to have been determined in earlier studies. Concerning the data analysis, the constitution of two groups, with one group with no limitation of walking and the other with walking disability, whatever the severity, induces a lack of grading in the assessment of walking function. However, this data analysis did allow us to establish ROC curves, as for a diagnosis test (‘disease’ or ‘no disease’). Furthermore, it allowed us to determine one threshold value of the 2MW test, above which the walking capacity can be considered as satisfactory (objective to achieve by prosthetic fitting).
Conclusion
Taking into account the limitations described above (non-exhaustive tests, patients without cognitive disorders and patients who had benefited from rehabilitation beforehand), the 2MW test could be proposed as the first-line test in routine clinical practice, to evaluate function (balance and walking capacity) in unilateral lower-limb amputees, during the stable phase. Among the various methods of evaluation used in this study, it is the one that combines the best psychometric properties, which makes it suitable for this population of patients, whatever the level of amputation, the aetiology and the type of prosthesis. As a second-line test, when questions arise concerning the specific implication of balance disorders and the fear of falling in the restriction of prosthetic walking, the FRT appears to be appropriate from a clinical point of view.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None.