
Abstract
Background:
The body is a kinetic chain and all the systems and muscle groups play important roles in this chain. Core stability, strength and balance are important components of performance within many sports, and in particular soccer. However, the relationship between these components is not fully understood.
Objectives:
To investigate the relationship between core stability, balance and strength in amputee soccer players.
Study Design:
Clinical pilot trial.
Methods:
Eleven amputee soccer players (mean age = 24.63 ± 6.48 years) participated in our study. A Kinesthetic Ability Trainer device was used to assess balance. Trunk strength was evaluated by isokinetic dynamometer. Gillet test was used to evaluate the sacroiliac joint movement. Modified plank test was used to determined dynamic core stability. Disability was evaluated using the Oswestry Disability Index.
Results:
The results showed that there was a correlation between flexor isokinetic trunk muscle strength at the velocity of 60°/sec and modified plank test (r = 0.630, p = 0.038). There was a negative correlation between flexor isokinetic trunk muscle strength at the velocity of 180°/sec and Oswestry Disability Index score (r = −0.649, p = 0.031).
Conclusions:
Amputee soccer is a sport which is generally performed with one limb balance with crutches. It is therefore perceived that a relationship between balance and sacroiliac mobility, and should be considered for evaluation process and performance analysis in amputee soccer. However, in future studies, we recommend that such evaluations on amputee soccer players should be carried out with increased numbers.
Clinical relevance
Many aspects should be considered in the evaluation of amputee soccer players. Core stability, balance and strength should not be ignored when designing a training program for an amputee soccer team.
Background
Absence of a member of the body, or part of it imposes changes in customary walking, which becomes inefficient and compels greater effort in a person’s locomotion. Lower extremity amputations in particular may cause functional disabilities or generate changes in the locomotor system.1,2 Endurance, balance, physical and cardiovascular performance are affected negatively as a result of amputation.3-5
Amputee soccer involves explosive activities like jumping, kicking, tackling, turning, sprinting, changing pace, and sustaining forceful contractions to maintain balance and control of the ball against defensive pressure. Balance is necessary for coordination, whatever position the body adopts. Before any movement, it is necessary to place the crutches firmly on the ground before the foot lands. In the course of the movement, both crutches are brought forward at the same time to ensure that balance is maintained as the step is taken. 1
As in regular soccer, good muscular support, balance and core stability are also very important in amputee soccer. In recent years the use of the term ‘core stability’ has increased in popularity among healthy individuals and athletes. The core of the body is a term used to refer to the trunk or, more specifically, the lumbopelvic region. Muscular support in this region is critical to maintain the integrity of the spine to support body mass plus additional loads that are supported during resistance training and sports activities.6-8 Core stability and strength is an important component to maximize efficient balance and athletic function in upper and lower extremity movements. 9
The body is a kinetic chain and all the systems and muscle groups play important roles in this chain. Taking this chain into consideration, core stability, strength and balance are all interrelated.5,9 Although it may be considered that the lack of a member of the body part can predispose to core stability problems, there appears to be limited evidence of this relationship in disabled athletes.
Therefore the aim of this study was to investigate the relationship between core stability, balance and strength in amputee soccer players.
Methods
Subjects
Two different teams, TSK Karagucu Team (n = 6, 54.5%) and Ankara Genclık Team (n = 5, 45.5%) one goalkeeper and others with a total of 11 amputee soccer players (age: mean ± (standard deviation) SD = 24.63 ± 6.48 years old, body mass index (BMI) : mean ± SD = 21.88 ± 2.08 kg/m2) participated in the study.
The data related to the descriptive and clinic characteristics of the subjects were collected. Before study participation, all subjects were informed verbally of the details of the study and all of them signed informed consent forms. The ethical approval was taken from the Turkish Sports Federation for the Physically Disabled.
The eligibility criteria were as follows:
≥ 18 years old
male
usage of prosthetics ≥ 4 hours/day
having played amputee soccer for at least two months prior to the start of the study.
Exclusion criteria were as follows:
suffering from any chronic or systemic disease (diabetes mellitus, hypertension, heart disease)
suffering from any vestibular, visual or cerebellar disease that effects balance
bilateral amputation.
Testing procedures
All the tests were done by the same physiotherapist on the same day. Firstly, descriptive and clinic characteristics of subjects were reported based on recall. Secondly, in order of disability, balance test, Gillet test, modified plank test, trunk strength were evaluated. A five minute interval was given between all tests.
Disability
Disability was evaluated by using the Oswestry Disability Index. The Oswestry Disability Index consists of 10 items; each item is scored from 0–5. Items include pain intensity, personal care, lifting, walking, sitting, standing, sleeping, employment/homemaking, traveling, and social life. 10 The total score ranges from 0–50. The disability level is increased by an increased total score. 11
Balance test
The Kinesthetic Ability Trainer (SportKAT 3000®) (LLC, Vista, Calif) device was used to assess static balance. The SportKAT 3000® consists of a movable platform supported on a central point by a small pivot. A tilt sensor on the platform is connected to a computer, which registers the deviation of the platform from a reference position18.2 times each second. The distance from the central point to the reference position is measured at every registration. From the summation of these distances, a score, the balance index (BI) can be calculated (a low BI implies good ability to perform the balance test). Static balance was evaluated without prosthesis standing on non-amputated limb. Each subject was allowed to practice a one-minute adaptation and learning period before the test. After that introductory session, the subjects participated in the static balance measurement for 30 seconds. During the static balance test, the subjects kept their eyes open to view on the monitor screen and tried to keep the red ‘X’ in the center of the screen. Each subject stood barefoot on the force platform in a natural position with arms placed across the chest. The pressure pillow of the force platform was set on six bars. To ensure that the balance measurement was accurate, the SportKAT 3000® device was calibrated, as recommended in its manual, before the test (Figure 1).12,13

Balance asessment with the Kinesthetic Ability Trainer.
Gillet test
The Gillet test was used to evaluate the sacroiliac joint movement. It was evaluated with prosthesis standing on the non-amputated limb. A physiotherapist palpated the sacroiliac joint and each subject was instructed to stand on the non-amputated limb and to flex the contralateral hip and knee towards the waist with arms placed near the body. The changes in the palpation points were noted by the physiotherapist. Reliability of the Gillet test has been previously reported (Figure 2). 14

The Gillet test.
Modified plank test
The modified plank test was used to determine dynamic core stability. Subjects lay on their non-amputated limb with the forearm of the bottom arm on the floor and the elbow bent. They rested their other arm on their top side. Subjects raised their body up, off the ground, and maintained a straight line from neck to feet and lowered their body down as a continuous movement. The number of repetitions of the movement was measured for dynamic core stability (Figure 3). 15

The modified plank test.
Trunk strength
A computerized isokinetic dynamometer (Cybex 770 Norm, Lumex Inc, Ronkomma, NY, USA) was used to evaluate trunk flexion and extension strength. Concentrically isokinetic trunk strength was tested at the velocities of 60°/sec, 120°/sec and 180°/sec. The lower limb or limbs were stabilized by pads. A belt was used to secure the pelvis and to limit the use of the hip flexor muscles. A shoulder harness and backrest provided anchorage to the moving upper section of the apparatus. Subjects performed five repetitions of trunk flexion and extension for each angular velocity. One trial repetition was allowed before starting the tests. A three-minute rest period was allowed between each set. Verbal encouragement was given by the physiotherapist during testing. Peak torque values at the velocities of 60°/sec, 120°/sec and 180°/sec were used for statistical analysis (Figure 4).12,16,17

Trunk strength assessment using isokinetic dynamometer.
Statistical analysis
The Statistical Package for the Social Sciences, version 15.0 (SPSS 15.0) was used to perform statistical analyses. Means, SDs and percentiles were calculated for descriptive and clinical characteristics of amputee soccer players. Spearman correlation coefficients were calculated to determine the relationships. r-value of ≥ 0.50 and p-value of ≤ 0.05 was accepted as the level of statistical significance for the correlation data.
Results
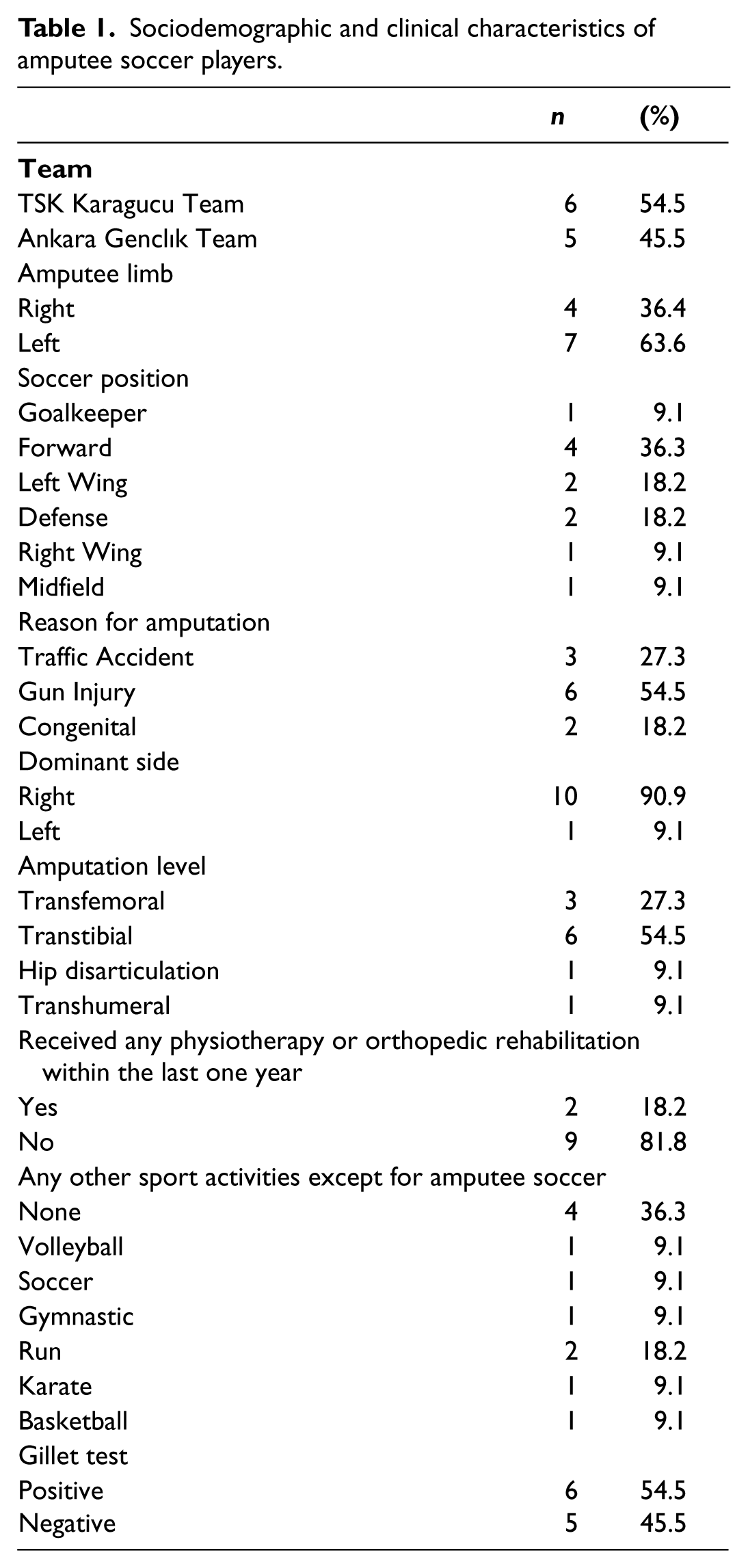
Descriptive and clinic characteristics of participants are shown in Tables 1 and 2.
Sociodemographic and clinical characteristics of amputee soccer players.
Descriptive and clinical characteristics of amputee soccer players.
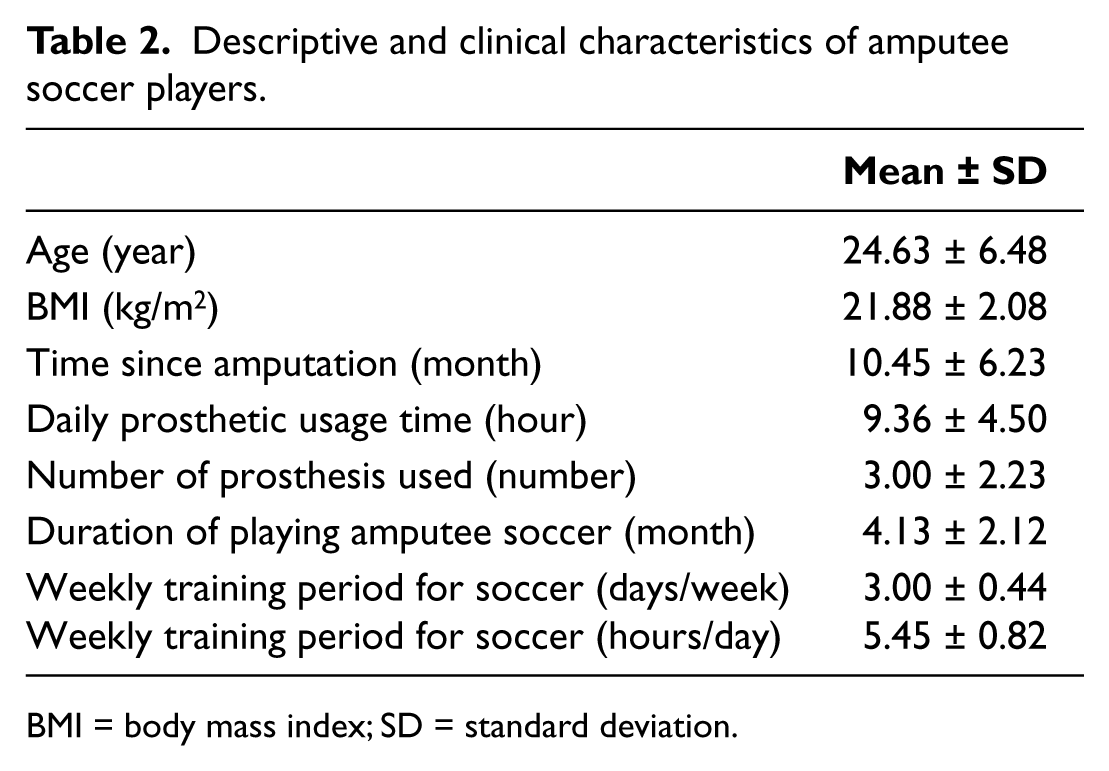
BMI = body mass index; SD = standard deviation.
There was a difference between core stability and Gillet test results (p = 0.017). There was a significant correlation between flexor isokinetic trunk muscle strength at the velocity of 60°/sec and modified plank test (r = 0.630, p = 0.038). There was a negative correlation between flexor isokinetic trunk muscle strength at the velocity of 180°/sec and the Oswestry Disability Index score (r = -0.649, p = 0.031) (Tables 3 and 4).
Outcome measurements of amputee soccer players.
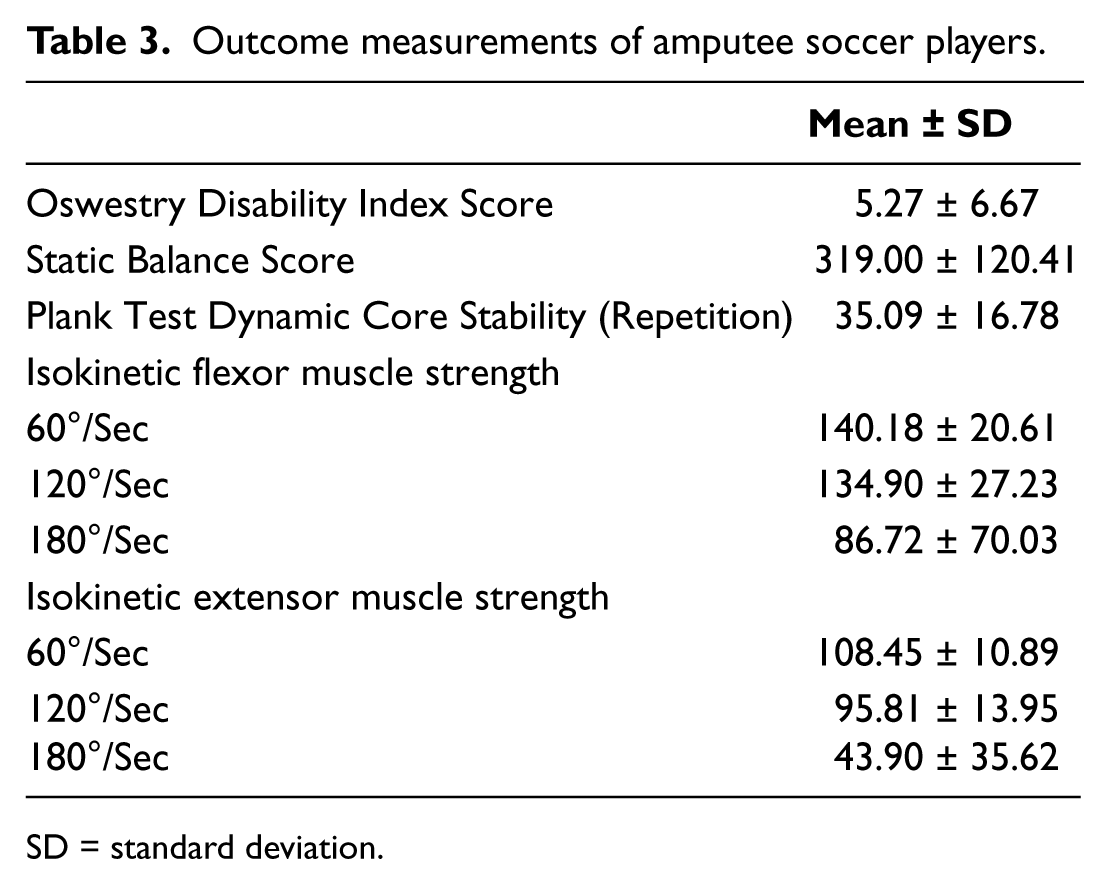
SD = standard deviation.
Correlation results of the study.
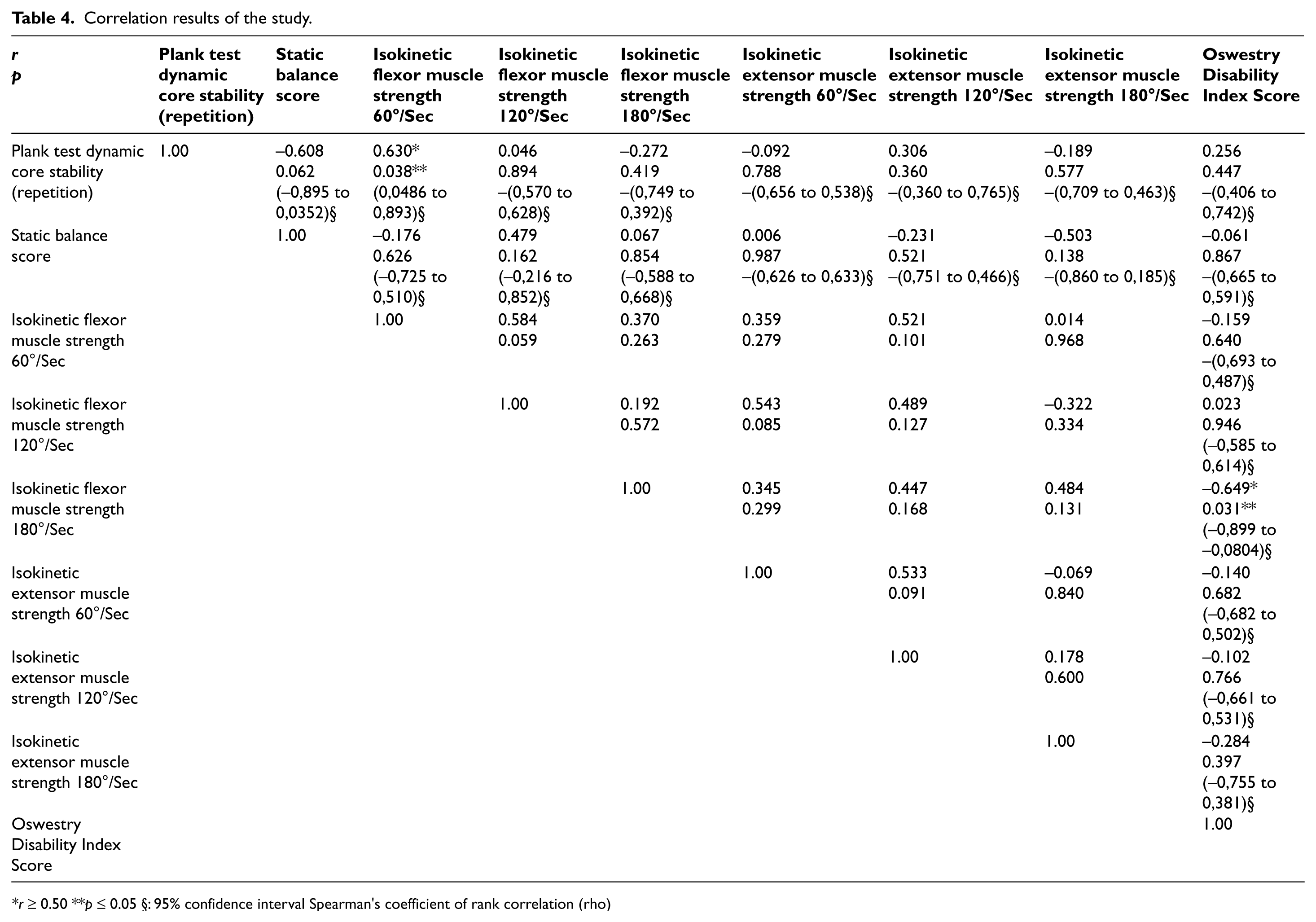
r ≥ 0.50 **p ≤ 0.05 §: 95% confidence interval Spearman’s coefficient of rank correlation (rho)
Discussion
Although amputee soccer is not considered to be a Paralympics’ sport, it is newly developing and popula. 1 Even so, the literature on the subject is relatively limited. We investigated the relationship between core stability, balance and strength in amputee soccer players to attract attention to disabled sport and make way for, and encourage, future studies on the subject. In our study a relationship was found between core stability and strength but balance was not a factor related to these parameters in amputee soccer players.
A weak core is believed to interrupt the transfer of energy, resulting in reduced sport performance and risk of injury to a weak or underdeveloped muscle group. For this reason there is an assumption that an increase in core strength will result in increased sport performance. 18 To develop an athlete’s full strength and power potential, the primary focus of the training program must be trunk strength. 19 Our results suggest that strength was related with dynamic core stability but Nesser et al. 18 had not identified significant correlations between core strength and athletic performance in healthy female soccer players. Although flexor trunk muscle strength had a positive relationship with dynamic core stability in male amputee soccer players, it had a negative relationship with disability. This contrast in the relationship between disability and strength was an expected result.
The most common musculoskeletal injuries among amputee athletes are sprains and strains to the lumbar spine and sacroiliac joint on the uninvolved side. 20 Our study results showed that there was a relationship between core stability and sacroiliac mobility.
There are several limitations of our study. First, the sample was small. Second, there was no control group. Third, while lower and upper extremities strength were also important for core stability, just modified plank test and sacroiliac joint movements were evaluated in this study. Lastly, different statistical analyses, such as multiple linear regression, would have given more information, but were not possible due to the size of the sample. This was a small population of amputee soccer players and, as such, the results of this study cannot be generalized to fit all populations of amputee players.
Strength, balance and stability could be affected by biomechanical and etiological problems among other. Many aspects should be considered in the evaluation of amputee soccer players. When designing a training program for an amputee soccer team to focus core stability, balance and strength should not be ignored.
Conclusion
Amputee soccer is a sport which is generally performed with one limb balance with crutches, so a relationship between balance and sacroiliac mobility should be considered for evaluation process and performance analysis in amputee soccer. However, we recommend that such evaluations and studies on amputee soccer players should be carried out with more cases in the future.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.