
Abstract
Background:
Patients who undergo transfemoral amputation after infection of a total knee arthroplasty do not have good functional outcomes and have major difficulty walking.
Objectives:
To evaluate the quality of life and walking ability among patients who underwent amputation and among those who refused to undergo amputation following infection of a total knee arthroplasty.
Study design:
Retrospective case series.
Methods:
Patients who received an indication for amputation following an infection of a total knee arthroplasty were evaluated retrospectively. The patients were divided between those who accepted the amputation procedure and those who refused amputation (four amputee vs four non-amputees). Walking ability and quality of life were evaluated using the Short Form–36 questionnaire.
Results:
The average physical health was 27.4 for the amputees and 31.3 for the non-amputees. The average mental health was 49.9 for the amputees and 47.1 for the non-amputees. In relation to walking ability, only one (25%) of the amputees was able to walk, as opposed to 100% in the non-amputee groups.
Conclusion:
Twenty-five percent of the amputee patients continued to be able to walk. The functional outcome of non-amputee patients was better, with 100% being able to walk, though with limitations.
Clinical relevance
This is the first study evaluating patients who refused the amputation procedure and remained with the spacer. Despite the fact that this option is not recommended by the medical community, we believe that these data are useful when discussing, with a patient, quality of life after amputation.
Background
Total knee arthroplasty (TKA) is an increasingly common surgical procedure. It is estimated that in the United States, 3.5 million TKAs were performed in 2003. 1 With the increasing number of arthroplasties, the number of complications arising from this procedure has also increased, especially deep infection.2,3
Currently, services that deal with arthroplasty infections have well-defined treatment protocols, 4 some with success rates of over 90%. 5 However, some cases still develop unsatisfactorily, and failure to treat the infection can culminate in an indication for transfemoral amputation, considered the last resort in the treatment flowchart 6 (Figure 1).
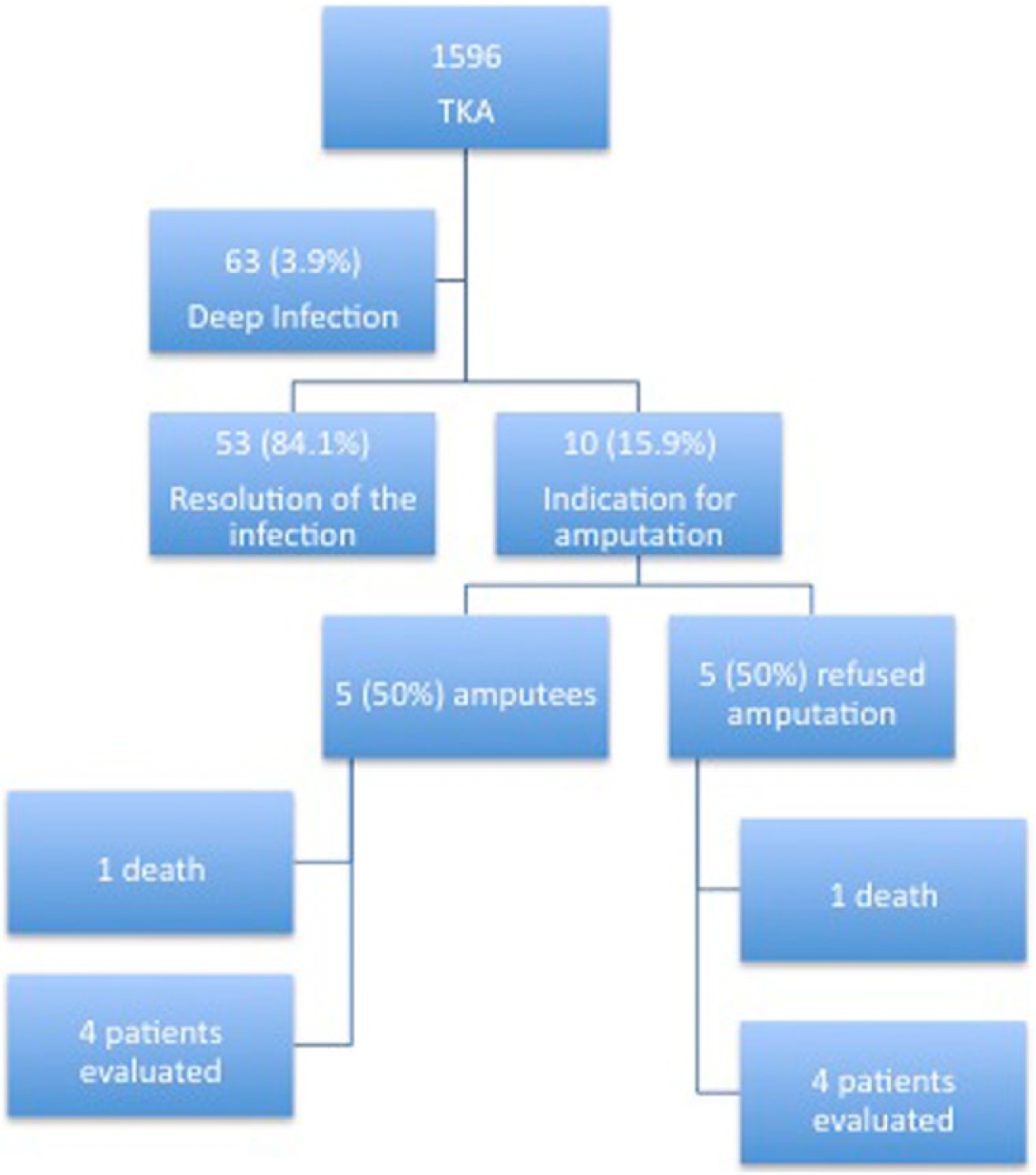
Flowchart for transfemoral amputations following total knee arthroplasty in our study.
Unlike traumatic amputations, where the outcome may often be better than the alternative of retaining the limb,7,8 the results of amputations following total knee arthroplasties are unsatisfactory, with few patients being able to walk with the use of prostheses.6,9 In recent literature, the best index of walking ability after amputation by infection after knee arthroplasty was 44%, with most series being around 30%.9–12
Another treatment option that can be considered after failed TKA is arthrodesis. Knee fusion proved to be better than amputation in a recent systematic review; however, this option has limited applicability in patients with severe bone loss and poor soft tissue coverage. 13
Even with clear indications for amputation, it is sometimes difficult for patients to accept this solution, 14 as amputees face social barriers, 15 find it difficult to look forward to the future, 16 and have limitations in their intimate and interpersonal relationships. 17 As a result, some patients do not accept this treatment under any circumstances.
The aim of our study is to compare patients for whom amputation was indicated for infections following total knee arthroplasty and who either underwent amputation or who did not accept the amputation procedure (and remained with a cement spacer).
Methods
A total of 1596 cases of total knee arthroplasty, performed from 2000 to 2012 at the authors’ service, were evaluated retrospectively. Of these cases, 63 (3.9%) developed deep infections and required surgical procedures such as debridement, polyethylene exchange, one-step revision surgery, or revision surgery with two treatment steps. In 53 patients (84.1%), success was achieved through treatment of the infectious process; however, 10 cases (15.9%) were considered unsuccessful (Figure 1).
In these 10 cases in which control of the infection was not achieved, treatment included several surgical cleanings, the use of spacers, and even rotational flaps for cutaneous coverage of skin lesions. Transfemoral amputation was indicated as a treatment for these 10 patients.
Of these 10 cases, five (50%) underwent amputations and five (50%) refused to undergo the amputation procedure, remaining with the cement spacer and inguinal maleolar immobilizer support. Three of the spacers were non-articulating and one of them was articulating, with the range of movement restricted between 5° and 45° (Figure 2). The patients who did not undergo amputation were counseled about the risks they could be running by maintaining an active infectious process in the knee joint. In our service, if an infection is considered to be local and there is no medical urgency, amputation is only performed with the patient’s formal acceptance, through the signing of a consent form, under the supervision of a social worker.
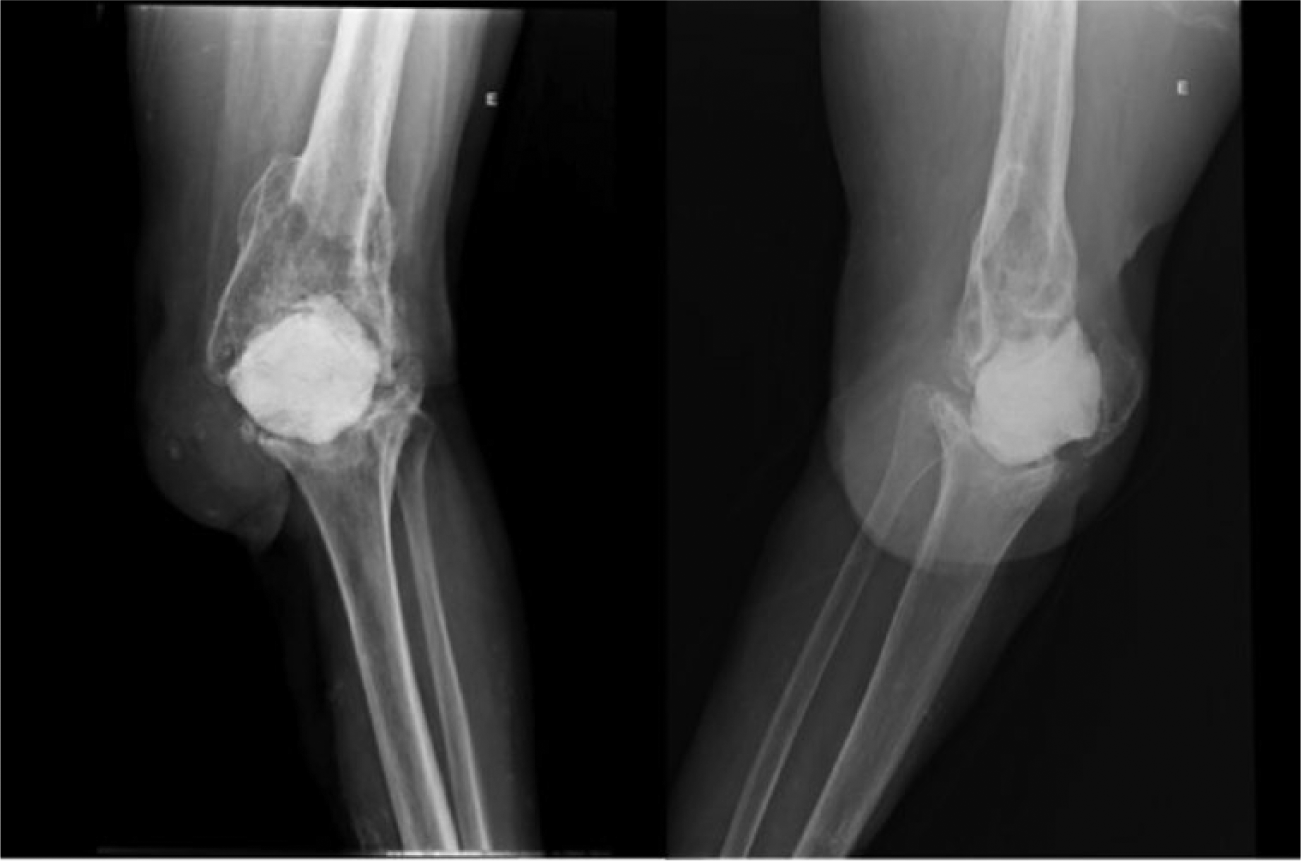
Front and lateral radiography of the knee of a patient who refused amputation and has a non-articulating cement spacer.
Of these 10 patients, a current clinical evaluation could be performed with 8 patients. One of the patients who refused amputation developed sepsis and underwent an emergency surgical amputation procedure, but died. Another patient who did undergo amputation also died due to a clinical pathology that was unrelated to the orthopedic condition.
The eight patients were assessed for age, comorbidities, cause of the total knee arthroplasty, infectious agent of the prosthesis infection, number of procedures performed in the attempt to control the infection prior to the indication of amputation, current quality of life based on the Short Form–36 (SF-36) questionnaire, and walking ability with the use of prostheses and accessory appliances.
The study was approved by the Ethical Committee of our institution, and informed consent was obtained (number 0742/08).
Results
Eight patients, four males and four females, with an average age of 66.3 years (42 to 84 years) were evaluated. The average age of the amputee patients was 61.75 years, and the average age of patients with spacers was 71 years. The evaluation took place 38.7 months post-amputation for the group of amputees and 34.2 months following the indication of amputation in the non-amputee group. The data are summarized in Table 1.
General data for patients included in the study.
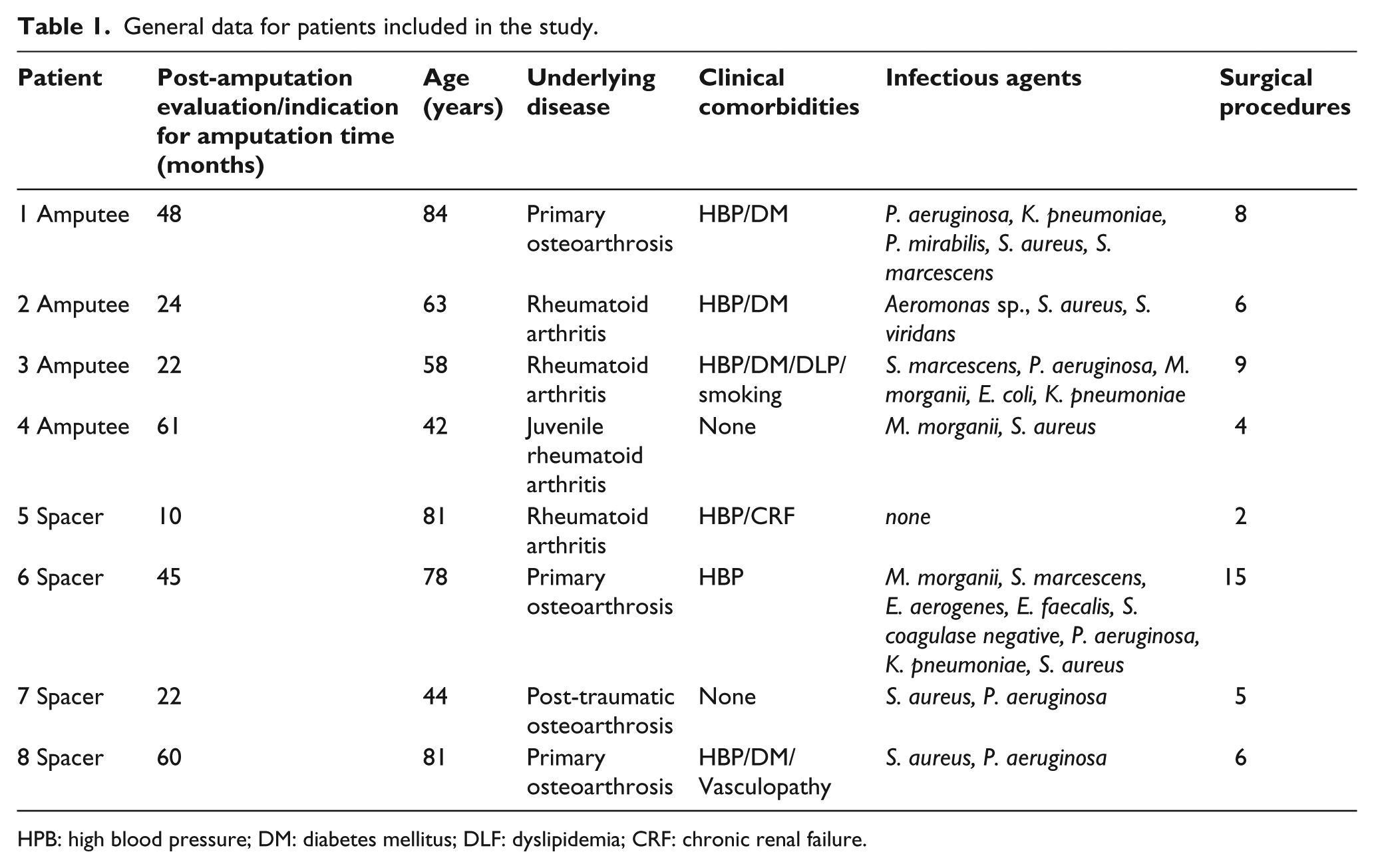
HPB: high blood pressure; DM: diabetes mellitus; DLF: dyslipidemia; CRF: chronic renal failure.
Three patients had primary osteoarthritis as the indication for the procedure, one patient had post-traumatic osteoarthritis, three patients had rheumatoid arthritis, and one patient had juvenile rheumatoid arthritis.
In accordance with the criteria established in the literature, two infections were classified as acute infections and six as chronic infections. All the infections, except one for which the agent was not identified, were polymicrobrial during the course of their evolution. The average number of infection-causing agents isolated per patient was 3.3 (ranging from 0 to 8 agents).
Before the indication of amputation, patients underwent an average of 6.8 (ranging from two to 15) surgical procedures in an attempt to control the infections.
All the amputations were unilateral and were performed above the knee, between the middle and distal thirds of the femoral shaft, above the adductor tubercle, and myodesis of the adductors and myoplasty of the extensor and flexor muscles were performed. The patients who did not accept amputation remained with the cement spacer and inguinal maleolar immobilizer for support.
All patients entered into strengthening programs, especially for upper limbs and quadriceps in an attempt to achieve walking ability and better fitting the prosthesis. Amputees only started the rehabilitation program when the stump was completely healed.
Assessing the quality of life based on the SF-36 questionnaire, the average physical health of the patients (PCS) was 27.4 for the amputees and 31.3 for the non-amputees. The average mental health of the patients (MCS) was 49.9 for the amputees and 47.1 for the non-amputees.
As regards walking ability, only one (25%) of the amputee patients was able to walk at home with the aid of a walking frame. The other three patients (75%) are not ambulatory, being restricted to a wheelchair for mobility. All of the non-amputee patients are able to walk, three of them with the assistance of a cane on the side opposite the affected knee and one of them with a walking frame (Tables 2 and 3).
SF-36 and walking ability of amputee patients.
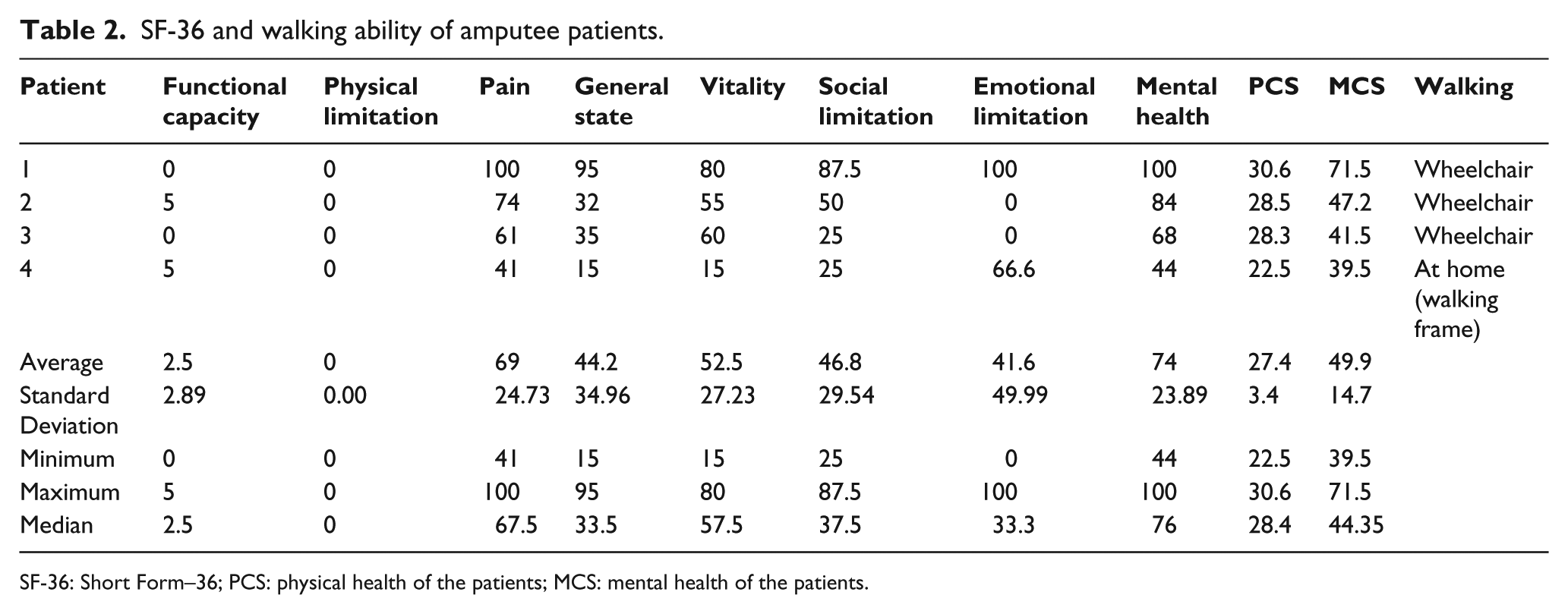
SF-36: Short Form–36; PCS: physical health of the patients; MCS: mental health of the patients.
SF-36 and walking ability of non-amputee patients.
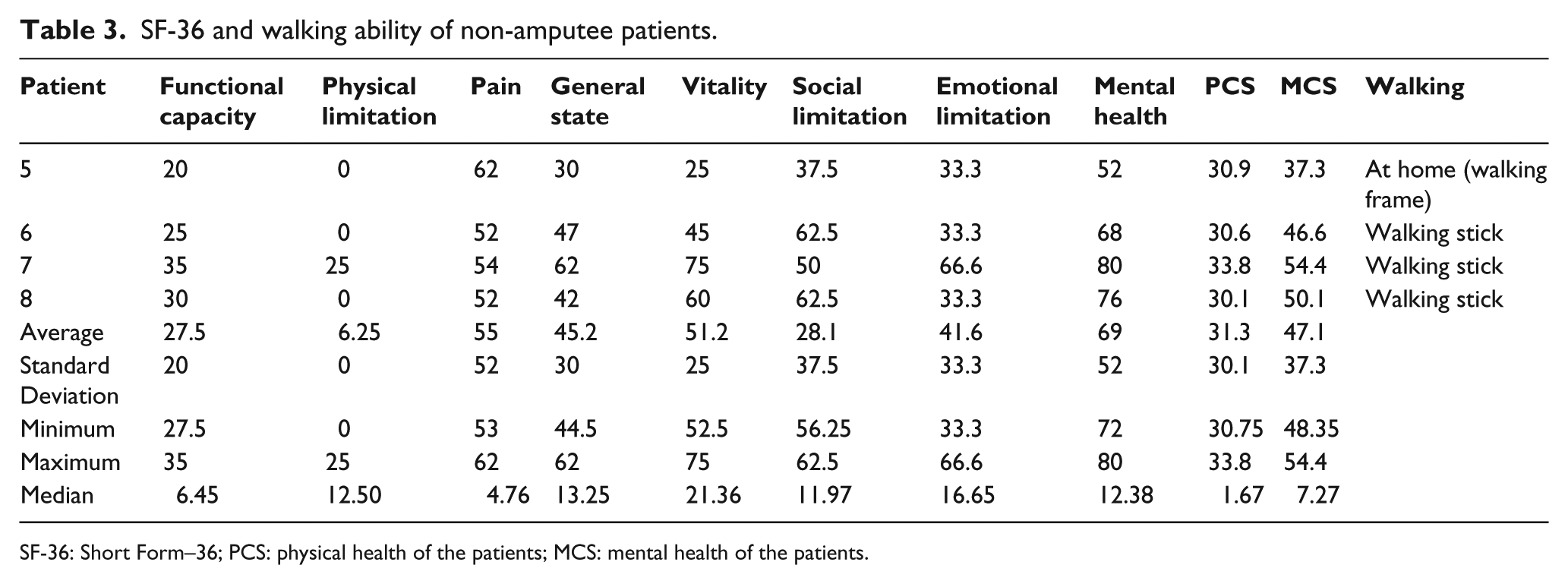
SF-36: Short Form–36; PCS: physical health of the patients; MCS: mental health of the patients.
Discussion
Amputation following a TKA is considered to be last-resort surgery for extreme cases, and is most often indicated following an uncontrolled infection. Although not well documented, several case series are found in the literature. Sierra et al., 9 in a survey of more than 18,000 TKAs performed over a 30-year period at the Mayo Clinic, found an amputation rate of 0.14% for problems directly related to TKA (the most common being infection), with an average patient age of 71.5 years. In the current study, amputation was indicated in 0.63% of 1596 cases over a 12-year period (all for infection), with an average patient age of 66.3 years. The difference in the rates is probably due to populational and socioeconomic differences. In another national case series, Mozella et al. 10 found a 0.41% amputation rate for 2409 TKAs, which is similar to our findings.
It is also important to note that the rate of deep infection found in our service is slightly higher than the rates documented in the current literature. Namba et al. 18 found an infection rate of 0.72% and Debarge et al. 19 reported an infection rate of 2.1%. This increase in numbers is due to the fact that most of our cases who underwent surgery were patients with a higher number of clinical comorbidities such as diabetes, autoimmune diseases, neoplasias, and kidney failure, and patients with post-traumatic arthrosis who had already undergone prior surgery. According to our healthcare system flowchart, patients with primary osteroarthrosis and few comorbidities who have not undergone prior knee surgery are transferred to smaller hospitals for arthroplasty procedures, so that only the more complex cases and, consequently, those with higher risk of infection, according to a study conducted by Rodriguez-Merchan, 20 are referred to our hospital.
Regarding the studied groups, it is possible to notice that in the amputation group, three of the patients had rheumatoid arthritis against only one from the group of non-amputees, a situation which may be considered to be of worse prognosis for walking, as rheumatoid patients may have dysfunction of several joints. Even though the rheumatoid patients in our study had mild involvement of other joints of the contralateral lower limb and the upper limbs, all of them were able to walk after arthroplasty and continued with functional gait until the infection. On the other hand, the mean age of the non-amputees group was almost 10 years higher than that of the amputee group, which could cause a worse walking capability.
In relation to walking ability, Sierra et al. 9 found that only 6 out of 22 patients were able to use a prosthesis and walk (27.3%), and only 1 of them was able to walk without support. Pring et al. 11 reported that only 30% of patients who underwent amputation were capable of walking regularly, and Isiklar et al. 12 corroborated these findings, identifying 35% of their sample as ambulatory. In Mozella et al.’s 10 case series, 44% of the amputees were able to walk with support. In our case series, only one (25%) of the patients (the youngest) was able to walk, but only with the aid of a walking frame. None of the other patients could walk at any point following amputation. Some patients were never able to adapt to using a prosthesis over the stump. The age of patients who are actually able to walk tends to be lower, since the functional demands and energy expended following a transfemoral amputation are significant. 21
Walking difficulty also occurs as a result of the general condition of the patients, who are usually malnourished and debilitated after the difficult treatment of the infection, bearing in mind that they have undergone, on average, six to eight surgeries before amputation, not to mention the existing comorbidities. In addition, these patients tend to have other affected joints, making walking even more difficult, especially in cases of rheumatoid arthritis, as was the situation in three of the four amputee patients in our case series.
Even with reduced walking ability, limited to inside their homes and only about the span of a block when out in the community, the patients who remained with the cement spacer were able to perform day-to-day activities like going to the bathroom without the help of other people, presenting greater functionality than the amputees.
Regarding the infectious agent, we found positive cultures for polymicrobial flora in all patients, probably due to the high number of surgeries to which they were subjected. The principal agents found were S. aureus in 75% and Pseudomonas aeruginosa in 62.5%. Other frequently occurring agents were Klebsiella pneumoniae, Serratia marcescens, and Morganella morganii, flora that are very similar to those found by Mozella et al. 10
The functional outcome in amputee patients is poor, which is corroborated by other studies in the literature.6,9,10,18,19 Assessing the quality of life through the SF-36 questionnaire, the average PCS was 27.4 for the amputee patients, while their average MCS was 49.9.
We did not find any studies in the literature comparing amputation with the preservation of the limb with a cement spacer in the knee. We emphasize that our case series can be considered to be accidental since the four patients who insisted on retaining the limb with a spacer had received an indication for transfemoral amputation and refused to undergo the procedure for personal reasons. Although the infections have caused no systemic effects to date, these patients can never be considered to be cured from the infection, opting to live with the risk of a more serious infection like that which occurred in the case where emergency amputation was necessary because of sepsis and ended in death. However, the law prohibits amputations from being performed without the patient’s consent, except where there is imminent risk to life, setting a precedent for the formation of the small case series presented here.
Comparing the amputee patients and those with spacers, we found a similar quality of life, with a PCS of 31.3 and an MCS of 47.1. The only difference in the SF-36 was in the area of functional capability (2.5 among the amputees as opposed to 27.5 among those with a spacer), as a result of the fact that all patients who retained the limb were able to walk with assistance. We once again emphasize that maintaining the limb with a cement spacer should not be recommended in any situation and is not defended by the authors, as it is a palliative and risky measure.
This article may be criticized as a retrospective series with few cases. However, if we consider that the post-TKA amputation rate is very low, a different study design would not be feasible. Because of the sample size, only a simple descriptive analysis was conducted, since statistical tests would not be appropriate. An important bias is the increased presence of rheumatoid patients in the group of amputees, since the presence of inflammatory disease with involvement of other joints may have compromised these patients’ gait.
In summary, our case series agrees with most articles in the literature that show a poor functional outcome for post-TKA amputee patients, with a less than 50% chance of walking. This is a critical item in discussing the prognosis of the proposed treatment with patients.
Conclusion
The percentage of indications of amputation in our service following TKA was 0.63% during the period analyzed, with only 25% of the amputee patients retaining their ability to walk. The functional outcome of patients who remained with the spacer was better, with walking ability of 100%, though limited and requiring support.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.