
Abstract
Background: Prosthetic gait increases demands on stability. Some variability measures can be used to investigate the stability of movement for prosthetic feet.
Objectives: The purpose of this study was to determine the influence of the prosthetic foot on ground reaction force variability for transtibial amputee gait.
Study Design: Comparative analysis.
Methods: Eleven male unilateral transtibial amputees participated in this study. Each subject walked at self-selected speed with both conventional (SACH) and energy storing (Sureflex) feet. Time and ground reaction force variables and their coefficients of variation were calculated for each foot type and limb.
Results: Mediolateral force variables had high variability for all conditions. The Sureflex had a larger variability than the SACH foot for the braking peak (p < 0.05), which may have been caused by gait instability after the heel strike. There were significant differences between intact and prosthetic limbs in total loading (force impulses) with the SACH foot (p < 0.05).
Conclusions: The prosthetic foot and alignment issues related to the foot influence GRF variability. During the braking phase the SACH foot is characterized by higher variability in mediolateral direction and Sureflex by higher variability in anterior-posterior direction.
Differences in variability in ground reaction force variables can represent a person’s stability. Observing variability can contribute to better understanding of critical events in gait cycle with the use of various prosthetic feet.
Keywords
Background
Limb loss is a large trauma to the human body. Afferent signals from proprioreceptors are reduced, which results in deterioration in balance 1 and limited function of selected muscles. 2 An amputee needs to adapt to their loss and learn new, or adjust to existing, movement patterns. The use of prostheses changes the structure of gait and energy consumption increases,3,4 in part due to the inability of the prosthetic foot and other components to generate equivalent energy to an intact limb. All of these factors can influence movement stability.
Stability of movement is very important in amputees because a fall may lead to musculoskeletal injury. Kendell et al. 5 describe six factors that can be related to dynamic stability in lower-limb prosthesis – shifts in anterior- posterior centre of pressure, shifts in mediolateral centre of pressure, cell triggering, maximum lateral force placement, stride time and double support time. They found that the prosthesis users may have adopted a gait pattern that promotes safe forward progression while minimizing adjustments in anterior-posterior and mediolateral motion.
Vanicek et al. 6 compared the gait patterns of recent amputee fallers to those of nonfallers during level walking by investigating their joint kinematics, kinetics and variability of temporal-spatial variables. Fallers had a significantly greater first vertical peak of the ground reaction force (GRF) and load rate on the prosthetic limb. Additionally, they reported a smaller ankle absorption power in terminal stance, larger power absorption in stance, and greater variability in the swing phase time on the intact limb.
Another study by Hausdorff et al. 7 showed a potential use of gait variability measures in augmenting the prospective evaluation of risk of falling in the community-living elderly. They reported lower stride time variability in subjects who had not fallen in 12 months, as compared with subjects who fell.
Ground reaction forces describe the interaction between the body and the ground and have been associated with movement stability. Schrager et al. 8 suggested that quantification of centre of mass control during narrow base gait may improve identification of older persons at risk of falling. With increasing age, walking velocity and step length variability and maximum mediolateral (M-L) centre of mass (COM) velocity and displacement were higher for narrow base gait compared to self-selected gait.
For amputees, foot type can influence GRF magnitude and variability during gait. Sung-Min et al. 9 analyzed GRF for four transfemoral amputees with fixed, single-axis and multi-axis prosthetic ankle assemblies. Based on absolute symmetry index and coefficient of variation analyses, they found that the variation of GRF timing among subjects was relatively lower in the single-axis system.
Further research on the influence of prosthetic foot type on GRF variability can provide a better understanding of course and stability of movement in transtibial amputee gait.
The purpose of this study was to assess the variability of GRF variables for unilateral transtibial (TT) amputees to determine the influence of the type of the prosthetic foot on the variability of gait variables.
Methods
This study compared the variability of GRF variables between intact and prosthetic limb and between SACH and Sureflex prosthetic feet. Each subject walked with both prosthetic feet.
Subjects
Eleven male subjects (age = 46.1 ± 12.0 yrs, height = 1.74 ± 0.12 m, weight = 82.5 ± 13.9 kg) with unilateral TT amputation were recruited from a local orthotics and prosthetics centre. Inclusion criteria were age from 30 to 70, ability to walk without an assistive device, at least 6 months after amputation, good residual limb health, and at least one month experience with conventional and energy storing feet. Exclusion criteria included neurological or physiological diseases that influence walking performance. The subjects had been wearing their current prostheses for 13.8 ± 12.5 years. Each was familiar with SACH and energy storing feet. All participants were fitted with a SACH foot following amputation and had progressed to an energy storing foot.
Six subjects used KBM (Kondylen-Bettung Münster – supracondylar patellar-tendon-bearing) and five TSB (total surface bearing) sockets.
Trauma was the cause of amputation for 10 of the subjects, whereas vascular etiology was cause for one candidate. All subjects performed ordinary daily activities and four actively participated in different sports. The study was approved by the ethics committee of the Faculty of Physical Culture, Palacky University in Olomouc. To take part in this study all participants gave written informed consent.
Experimental procedures
All participants walked with SACH (solid ankle cushion heel, ING corporation, Frýdek Místek, Czech Republic) and Sureflex (energy storing foot, Össur, Reykjavik, Iceland) prosthetic feet. Prosthetic feet were aligned and adjusted by two prosthetists who fitted the subjects throughout their clinical program. At first, subjects walked with the SACH foot and then with the Sureflex foot. Subjects had time to get used to each prosthetic foot before data collection.
Subjects were instructed to walk at a self-selected pace across two force platforms (AMTI, OR6-5, Advanced Mechanical Technology, Inc., Watertown, MA, USA) centred within a 10-m gait laboratory walkway. GRFs were sampled at 1,000 Hz per channel. Each subject performed a minimum of three practice walking trials, allowing him to adjust his starting point so that the feet naturally, and completely, made contact with both force plates. Investigators observed each trial, eliminating trials in which subjects missed or ‘targeted’ the force platforms. Three successful walking trials for each subject, with each prosthetic foot, were evaluated.
Data processing
GRF data were analyzed using software developed by Vaverka and Elfmark 10 in MATLAB (Version 7.0.1., Math- works, Inc., Natick, MA, USA). The data were filtered with a low-pass fourth order Butterworth filter with a cut-off frequency of 6 Hz 11 and normalized to subject’s body mass. Time was normalized to stance phase duration. The vertical GRF was used to determine the beginning and end of stance, with a threshold value of 5% body weight. Time and GRF variables for both the intact and prosthetic limbs are shown in Figure 1.

Observed variables derived from ground reaction force components, (a) mediolateral component (M-L); (b) anterior-posterior component (A-P); (c) vertical component (V).
Statistical analyses
The coefficients of variation (CV) were calculated for the intact and prosthetic limbs for each subject. The Wilcoxon test (Statistica, version 8, StatSoft, Inc., Tulsa, OK, USA) was used to determine statistical differences in CV between prosthetic and intact limbs and between SACH and Sureflex prosthetic feet (p < 0.05). The effect size was evaluated using Cohen’s d for variables with statistical difference, and values higher than 0.8 (large effect) were deemed significant. 12
Results
Variability of observed variables
Mean CV values for all variables are presented in Table 1. All mean CV values for time variables were less than 20%, with seven variables having CV values greater than 10%. The higher CV values occurred in the first half of stance for both intact and prosthetic limbs, with three of seven occurrences for the ‘time to braking peak (t4)’ measure. The largest CV for GRFs and impulses were found in the M-L direction (F1, F2, I1, I2).
Mean CV values of measured variables (%) for intact and prosthetic limbs and SACH and Sureflex feet.
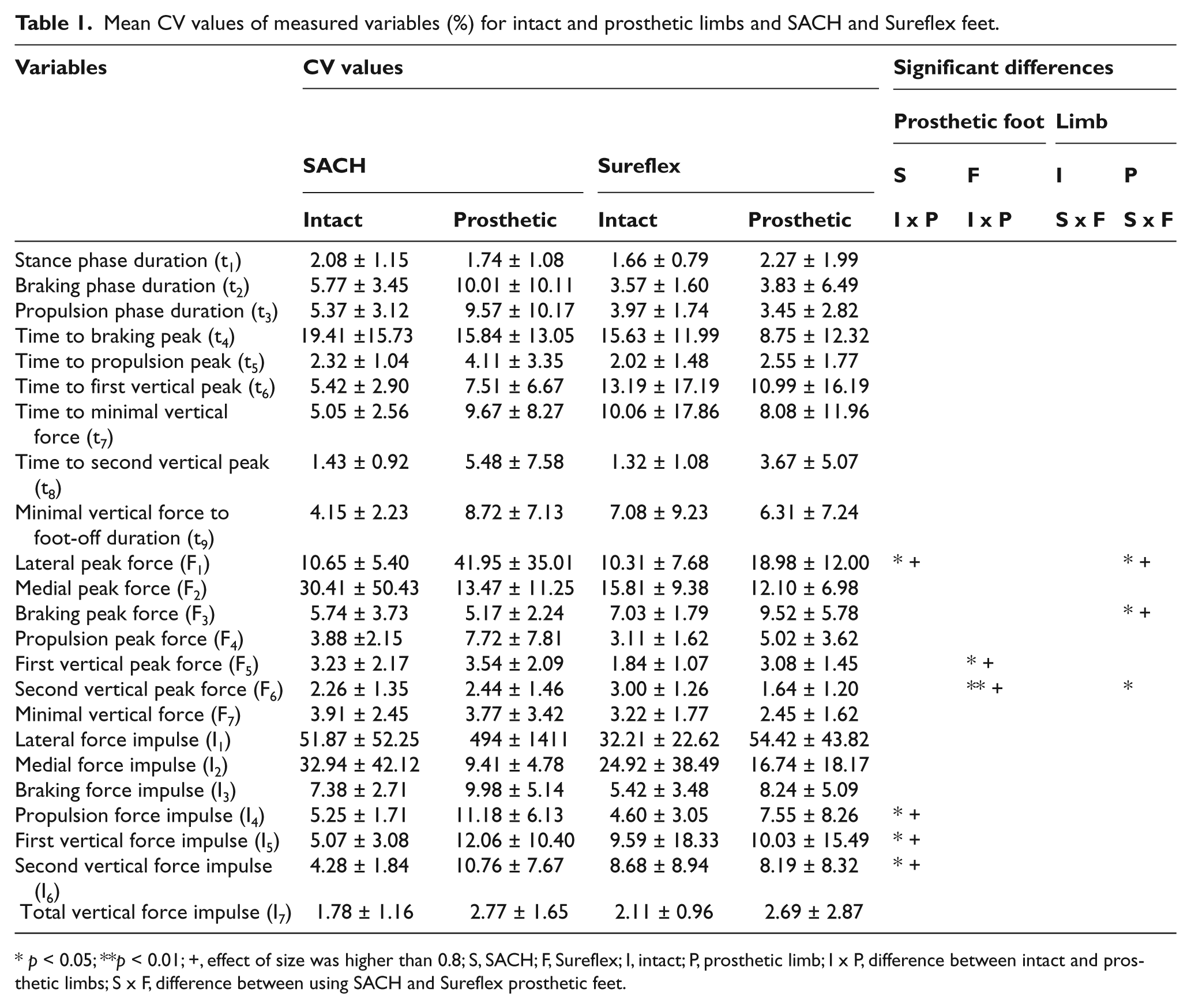
p < 0.05; **p < 0.01; +, effect of size was higher than 0.8; S, SACH; F, Sureflex; I, intact; P, prosthetic limb; I x P, difference between intact and prosthetic limbs; S x F, difference between using SACH and Sureflex prosthetic feet.
Variability comparison between intact and prosthetic limb and SACH and Sureflex prosthetic feet
Few statistically significant differences were found between the two types of prosthetic feet. For the prosthetic limb, SACH foot GRF CV was significantly greater (p < 0.05) than the Sureflex for lateral peak (F1) and lower for breaking peak (F3).
When comparing limbs during gait with the Sureflex prosthetic foot, GRF CV of the first vertical peak (F5) was significantly greater in the prosthetic limb (p < 0.05) and CV for the second vertical peak (F6) was significantly greater in the intact limb (p < 0.01); however, all CV for these measures were low (i.e., less than 3.08%). For the SACH foot, CV for lateral peak GRF (F1), propulsion force impulse (I4), first vertical force impulse (I5) and second vertical force impulse (I6) were significantly lower (p < 0.05) on the intact limb in comparison with prosthetic limb.
Discussion
Variability has been considered a useful physiological system indicator, and its presence is typically considered as a negative phenomenon. However, if we consider variability as a result of multiple interacting controls, then variability reveals itself as a necessary component in aiding system adaptability. Variability in amputee locomotion can be influenced by two components: the person’s body and the prosthesis. The body must accommodate biological and mechanical components for successful movement.
It is important to consider what kind of variability is natural to humans. Winter 13 mentioned low variability for kinematic and GRF data over a complete stride for a healthy population with CV values from 7 to 20%. Shimada et al. 14 showed the variability of maximal and minimal values for vertical, anterior-posterior (A-P), and M-L components of the GRFs CV values below 10% for a normal population. For comparison, we calculated CV values from other studies and found low stance phase duration CVs for both intact (< 3 %) and prosthetic (< 6%) limbs.15-16
The M-L GRF variables in our study had the greatest variability. These differences occurred for both peak and impulse measures. Medial peak GRF for a healthy population was evaluated by Shimada et al. 14 (6.2%) and Masani et al. 17 (8.6%). Our findings showed that medial peak GRF CV for amputee walking was much higher than able-bodied subjects for both the intact and prosthetic limbs, with CV for the intact limb and SACH foot reaching 30.4%. One of the reasons of higher values of CV is that mean values of lateral and medial peaks varies around zero.
The largest CV values occurred for lateral impulse on the prosthetic side with the SACH foot. This variability could be associated with the foot’s cushioned heel; however, lateral impulse CV was also high for the Sureflex foot. Therefore, lateral impulse CV may not be a useful variable for comparing the effect of prosthetic feet on walking variability.
The GRF peak CV values in our study for braking (< 10%) and propulsion (< 8%) were lower than the CV values published by other authors. We calculated SACH foot CV values from the study by Zmitrewicz et al. 16 and found CV results of approximately 20% for intact and 30% for prosthetic limbs. The results from Vanicek et al. 6 showed CV values from 15% to 36% for non-faller amputees and values from 25% to 44% for faller amputees.
CV values for vertical GRF components were the lowest, with prosthetic limb results being comparable to other studies. CV values for the first and second vertical peaks, derived from Nolan et al. 15 for active subjects (only first peak) and Vanicek et al. 6 for faller and non-faller amputees, were less than 9%. Intact limb results from these authors showed greater variability than our study (non-fallers < 12%, fallers < 25%, highly active < 17%).
For braking and propulsion impulse, CV values derived from Postema et al. 18 were also greater than values in our study. Braking and propulsion impulses varied for four prosthetic feet from 16.9% to 23.3%.
In our study the type of prosthetic foot did not significantly influence variability for time variables. While walking speed variance has been found to be lower for amputees than for control subjects 19 and swing time variability on the intact limb was found to be significantly higher for amputee fallers compared to non-fallers, 6 time-based variability parameters may not be as useful when comparing changes in prosthetic feet within subjects.
In our study we did not find any variables that had a significant difference in variability between prosthetic and intact limbs for both prosthetic feet together, except the medial peak. Therefore, most of the changes in variability were influenced by prosthetic feet or alignment issues related to the foot. We found the most significant differences between prosthetic and intact limbs for the SACH foot, which showed higher variability mainly in total loading of the foot (impulse). Similar tendencies can be found in braking and propulsion impulses derived from Zmitrewicz et al. 16
For the Sureflex foot, the two significant differences were between intact and prosthetic limbs for vertical GRF; however, the mean CV for both limbs (4%) were smaller than in other studies.6,15
When comparing feet, we only found significant differences during the braking phase. With the Sureflex foot there was higher variability in the A-P direction while the SACH foot had higher variability in M-L direction. These results could be due to faster shifting between the heel and forefoot, a smaller load on the midfoot area, and smaller deviations from the foot axis with Sureflex feet, in comparison with SACH feet. 20 GRF during the braking phase can also be influenced by foot flexibility 21 or the roll-over shape arc length. 22 Further research is needed to determine if these factors also influence force variability.
Potential limitations of this study include the small number of trials for each prosthetic foot. Also, the population sample could be larger and more homogeneous.
Conclusions
From the perspective of time, GRF and GRF impulses derived from vertical and A-P components, walking performance of TT amputees has lower variability than the able-bodied population. Variables obtained from the M-L GRF component had the largest variability.
Prosthetic feet can significantly influence walking variability for some GRF variables. For SACH feet, prosthetic limb variability was larger than the intact limb for GRF vertical impulse during the propulsion phase. In comparison of SACH and Sureflex prosthetic feet, on the prosthetic limb, during braking phase the SACH foot is characterized by higher variability in M-L direction and Sureflex by higher variability in A-P direction.
Footnotes
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
This work was supported by the Ministry of Education, Youth and Sport of the Czech Republic [grant number MSM 6198959221].