
Abstract
Background: The main determinants of prosthetic use known from literature apply to the younger patient with lower limb amputation. Studies aimed at identifying determinants of outcome of lower limb amputation in elderly patients with multimorbidity that rehabilitate in skilled nursing facilities (SNFs) are scarce.
Objectives: To predict prosthetic use and physical mobility in geriatric patients admitted to SNFs for rehabilitation after lower limb amputation and the impact of multimorbidity.
Study Design: Prospective design.
Methods: Univariate and multivariate logistic and linear regression analyses were used to identify determinants that were independently related to prosthetic use and the timed-up-and-go test (TUG test).
Results: Of 55 eligible patients, 38 had complete assessments on admission and at discharge. Fifty per cent was provided with a prosthesis. Multimorbidity was present in 53% of the patients. Being able to ambulate independently, and having a transtibial amputation (rather than a higher level of amputation), without phantom pain determined prosthetic use (R2=56%), while cognitive abilities, low amputation level, and pre-operative functional abilities were independently associated with the TUG test (R2=82%).
Conclusions: Elderly patients referred to an SNF for prosthetic training have a high probability of using a prosthesis when having an independent ambulation after transtibial amputation, without phantom pain. These patients should be considered for prosthetic training.
This study gives more insight into the outcomes of geriatric patients with lower limb amputation after rehabilitation in skilled nursing facilities. This is the first study that focuses on determinants of prosthetic use in these elderly patients, often with multimorbidity.
Background
The impact of a major lower limb amputation on mobility is high, especially in elderly patients. Learning to live with a lower limb amputation and to use a prosthesis in daily life activities demands good physical, as well as cognitive, capacities. Even young healthy patients with a traumatic lower limb amputation may need a considerable period to regain their pre-existent functional status, in which many of them only partially succeed. 1 Prediction of rehabilitation outcome, in particular prosthetic use, is of great interest to physicians and therapists as well as health insurance companies that reimburse the costs of the prosthesis and the rehabilitation process. From a patient perspective, an accurate prognosis of the outcome of rehabilitation is also important. Several studies on rehabilitation outcome after lower limb amputation show that age,2-4 amputation level,5-7 stump problems,1,8 and cognitive abilities3,5,9 are clinically important determinants. However, most of these studies have been conducted in rehabilitation centers with relatively young patients.1,2,4,5,8 Only two studies focused specifically on the geriatric patients with lower limb amputation; Wong et al. 6 studied predictors of mortality, while Fletcher et al. 7 focused on predictors of successful fitting of a prosthesis in patients above the age of 65 years in a rehabilitation center.
At an advanced age, the most important reason for lower limb amputation is peripheral arterial disease (PAD). Patients with PAD often have other medical conditions, such as diabetes mellitus (DM), that may negatively influence their physical and mental capacities which, in turn, may affect their prosthetic use. However, a consistent relationship between multimorbidity and prosthetic use has not been established in the literature. It has been reported that patients with coronary arterial disease are less likely to walk with a prosthesis.10,11 While cerebrovascular disease, 12 respiratory problems, 13 and ‘other comorbidities than cardiopulmonary diseases and DM’ 3 would also be independently and negatively associated with prosthetic use. However, other studies could not establish a significant and independent relationship between prosthetic use and comorbidities. 4 In a systematic review on predictors of prosthetic use after lower limb amputation, Sansam et al. concluded that the effect of comorbid conditions on walking with a prosthesis is not clear at all. 14 They found large differences between the used methodology and definitions of medical conditions in these studies. In all studies, single medical conditions were investigated in relation to prosthetic use, instead of multiple interacting diseases, often seen in geriatric patients. As a consequence, the influence of multimorbidity on prosthetic use in geriatric patients with a lower limb amputation is still unknown.
In the Netherlands, elderly patients with impaired physical capacities are often admitted to skilled nursing facilities (SNFs) for ‘low intensity’ rehabilitation after lower limb amputation. These patients usually suffer from multimorbidity and often additional cognitive impairments. 15 Literature suggests that they have a low probability of prosthetic use and obtaining ambulatory skills. 14 Although there is some literature on outcomes of patients who rehabilitated in skilled nursing facilities,3,16 there are no studies that have systematically investigated the probability and determinants of prosthetic use in this geriatric population. Therefore, the aim of this study was to determine the predictors of prosthetic use and the association with multimorbidity in geriatric patients with a major lower limb amputation admitted to SNFs. It was hypothesized that multimorbidity would have an independent negative influence on prosthetic use and ambulatory skills in this population.
Methods
This study is part of the Dutch Geriatric Rehabilitation in AMPutation and Stroke (GRAMPS) study, which is a prospective, multicenter, cohort study primarily aimed at identifying determinants of rehabilitation outcome in SNFs. From January 2008 until March 2010, multidisciplinary teams collected data within two weeks after admission and at discharge from the rehabilitation ward, or at the latest one year after admission to the SNF. The regional medical ethics committee approved the study protocol.
Participants
All patients who were consecutively admitted to one of 11 SNFs in the southern part of the Netherlands for rehabilitation after lower limb amputation were eligible. No additional inclusion criteria were applied. After admission, patients were provided with oral and written information about the study by the local elderly care physician or nurse. The patients gave their written informed consent, while the attending physicians judged their legal capacity. In the case of any doubt, the caregivers were consulted and asked for their written informed consent. Patients who were legally incapable on admission, and those who had minor amputations that did not require a prosthesis were excluded from participation. Demographic characteristics, length of stay in the SNF, and discharge destination were also registered for the excluded patients.
Outcome measures
The primary outcome measure was prosthetic use, as assessed by the Special Interest Group of Amputee Medicine (SIGAM) classification. 17 The SIGAM measures mobility in patients with major lower limb amputation, which ranges from level A (not using prosthesis or use of cosmetic limb only) to F (normal or nearly normal use of prosthesis). We dichotomized the SIGAM in level A versus level B-F. In our study, we used the Dutch version called the SIGAM-WAP. 18 The timed-up-and-go test (TUG test) 19 was used as a secondary outcome measure to measure physical mobility. In the TUG, a physiotherapist measures time while a patient stands up from a sitting position, walks three meters (with or without a walking aid), turns, walks back and sits down again. Both outcome measures were also assessed at discharge from the rehabilitation ward.
Independent variables
Multimorbidity was measured using the Charlson Index (CI). 20 The CI comprises 19 categories of diagnoses derived from the International Classification of Diseases (9th Revision Clinical Modification ICD-9CM), and is based on a set of risk factors for one-year mortality risk. We excluded PAD and DM from the total score of the CI, because these two items reflect the condition being investigated, and DM was entered as a separate factor in the analyses. Multimorbidity was defined as having a CI score of > 1. 21 The attending elderly care physician also collected characteristics, related to the amputation, i.e. amputation level (high versus low), the presence of phantom pain (patients were asked if they experienced phantom pain), stump pain (patients were asked if they experienced wound pain), and wound healing problems (these were assessed by the physician). A ‘high’ amputation level was defined as hip disarticluation, transfemoral amputation (TFA) or knee disarticulation. A ‘low’ amputation level was defined as transtibial amputation (TTA). Other relevant characteristics, such as age, gender, and length of hospital stay, were collected from patients’ charts.
For evaluation of the functional status at baseline, various research instruments were selected. The Barthel Index (BI) 22 was recorded as a measure of basic activities of daily living (ADL). In addition, the preoperative BI was estimated based on history taking. For the assessment of extended ADL, the Frenchay Activities Index (FAI) was registered.23,24 The FAI scores the actual activities undertaken by patients and has three domains: domestic housework, indoor activities and outdoor activities. The one-leg-standing balance test, first used by Schoppen et al., 3 was used to assess standing balance on the unaffected leg, and is categorized in: not able to stand on one leg, able to stand on unaffected leg with support, able to stand on one leg without support < 10 seconds, and able to stand without support on unaffected leg without support > 10 seconds. The most obvious differences are observed between patients that can hold their balance and patients that cannot while standing on the unaffected limb without support. 3 The Functional Ambulation Categories (FAC) 25 measures (in)dependency of gait. FAC is an ordinal six-point scale: FAC0, FAC1, FAC2, FAC3, FAC4, and FAC5, with 0 indicating total dependency for walking and 5 indicating independent walking on all surfaces. The use of a walking device is allowed. Global cognitive functioning was measured using the Mini Mental State Examination (MMSE). 26 It comprises items testing orientation, attention, memory, language and constructive abilities. The clock drawing test 27 gave additional information about cognitive abilities.
Statistical analysis
The data were processed using the Statistical Package for Social Science 16.0 (SPSS 16.0). First, the intraclass correlation coefficients (ICCs) were calculated to determine whether outcome measures of the participants were nested within the 11 participating SNFs, which would require multilevel analysis. In addition, to exclude selection bias, differences in demographic characteristics between included and excluded patients were tested using t-tests, or non-parametric tests.
The association of each independent factor to prosthetic use was calculated using Chi square test, Student’s t-test, and non-parametric tests when appropriate. The associated factors for the TUG test were obtained by univariate linear regression analysis. The associated variables that were statistically significant (p < 0.10) were subsequently entered in a multivariate regression model. Variables that were found to have high correlations with other variables in the model (Spearman’s Rho > 0.9) were eliminated to allow for convergence of the model. Through stepwise elimination, all non-contributing variables were excluded, thus, leading to the best-fit model (p < 0.05). Odds ratios and beta coefficients, with corresponding 95% confidence intervals, were calculated for each of the independent variables. The independent contribution of each of the factors in the model was calculated using (Nagelkerke) R2 and R2 change scores.
Results
Of the 55 patients admitted for rehabilitation after amputation, 46 patients were included in this study. Four patients were legally incapable, three did not give informed consent, and two patients were admitted for rehabilitation after minor amputations. Of the included patients, 43 underwent an amputation because of PAD with or without DM, one patient had a tumour, one patient had an osteomyelitis due to infected ostesynthesis, and one patient had a trauma, which required amputation. The patients included in the analysis did not differ significantly from the excluded patients in terms of age (Mann-Whitney U 168.0, p = 0.375) or gender (Chi square 1.085, p = 0.298). The duration of rehabilitation period between included and excluded patients was borderline significant (Mann-Whitney U 101.50, p = 0.060). The median length of stay of the included patients was 143 days (range 15–365), while the median length of stay of excluded patients was 64 days (range 17–255). Table 1 presents the characteristics of the included patients. The ICC of the outcome measure prosthetic use nested within the participating SNFs was 0, indicating that aggregation of data is allowed to perform further analysis.
Patient characteristics (n = 46) and prosthetic use (n = 38) in patients with lower limb amputation in skilled nursing facilities (SNFs).
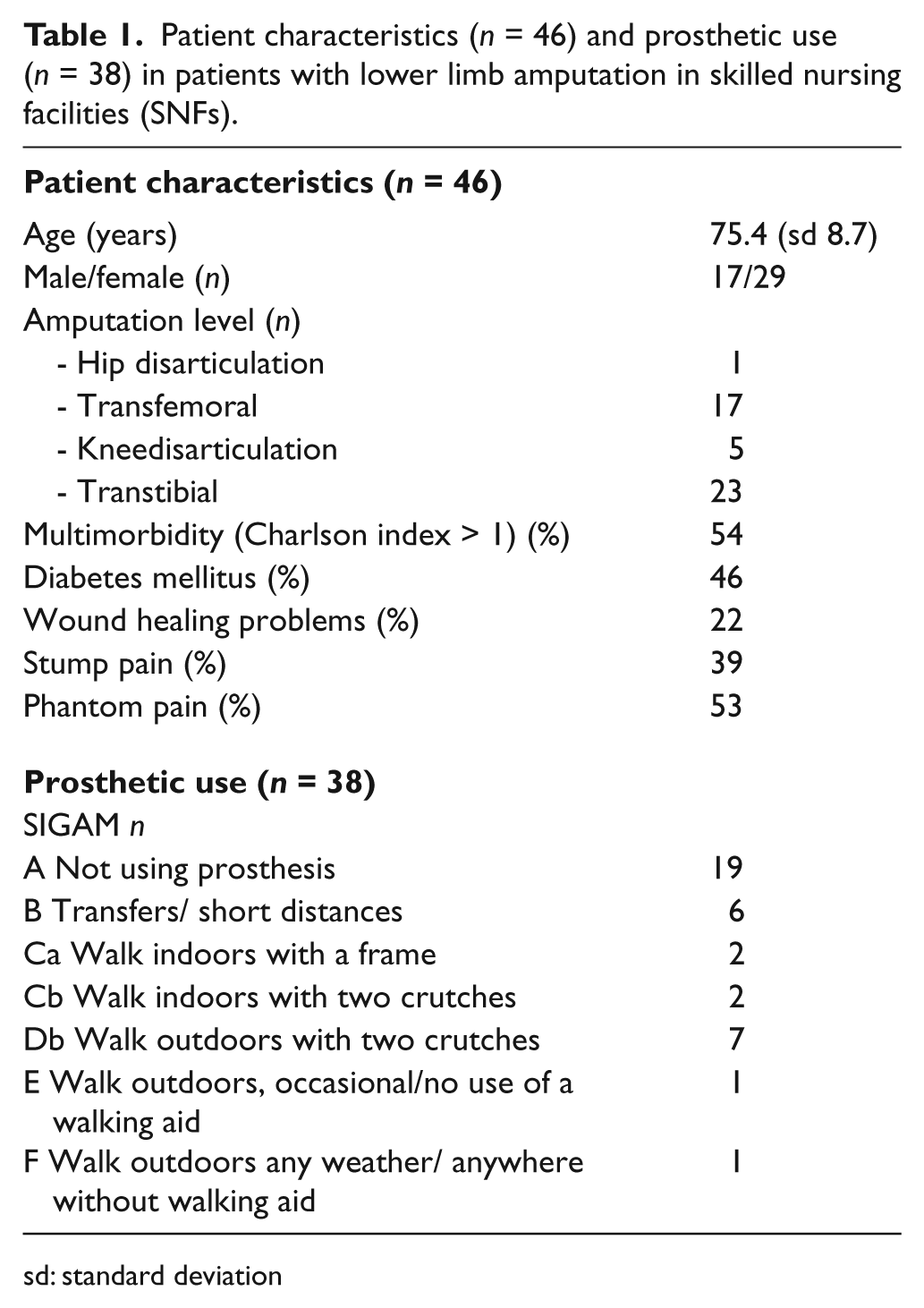
sd: standard deviation
Of the 46 included patients, eight patients died during the rehabilitation. Seven died of congestive heart failure. Outcome data, concerning the primary outcome measure prosthetic use, were therefore available for 38 patients, of which 31 could be discharged to an independent living situation within one year after admission. Fifty per cent of the patients made use of a prosthesis at discharge from the rehabilitation program (Table 1). Of the 19 patients that were fitted with a prosthesis, only two were not discharged to an independent living situation and were transferred to nursing home long-term care units. Outcome data for the secondary outcome measure, TUG test, were available of 15 patients. Of the four randomly missing values, two patients used their prosthesis for transfers or short distances only (SIGAM category B) and two used their prosthesis outdoors (SIGAM category Db). The mean TUG test at discharge was 33 seconds (SD 23).
Fifty-four percent of the patients had multimorbidity. The median CI score was 2 (range 0–5). Diseases of the vascular system were highly prevalent. Cardiovascular diseases (ischemic heart disease and/or congestive heart failure) were present in 46% of the patients, and 22% had had a stroke. Additionally, 13% had moderate-to-severe kidney disease. Chronic pulmonary diseases and diseases of the musculoskeletal system were present in 20% and 15% of the patients, respectively. The CI score did not significantly correlate with length of stay (Spearman’s Rho -0.04, p: 0.820).
Predictors of prosthetic use and TUG test
Table 2 shows the univariate analysis of the potential predictors and the outcome parameters prosthetic use and TUG test at discharge from the rehabilitation ward. Amputation level (high versus low), the presence of phantom pain, preoperative BI, FAC-score, and one-leg balance were significantly associated with prosthetic use. Gender, amputation level, impaired wound healing, MMSE, and preoperative BI were significantly associated with the TUG test.
Associations for prosthetic use and univariate linear analyses for timed up-and-go test (TUG-test) after rehabilitation for lower limb amputation in skilled nursing facilities (SNFs).
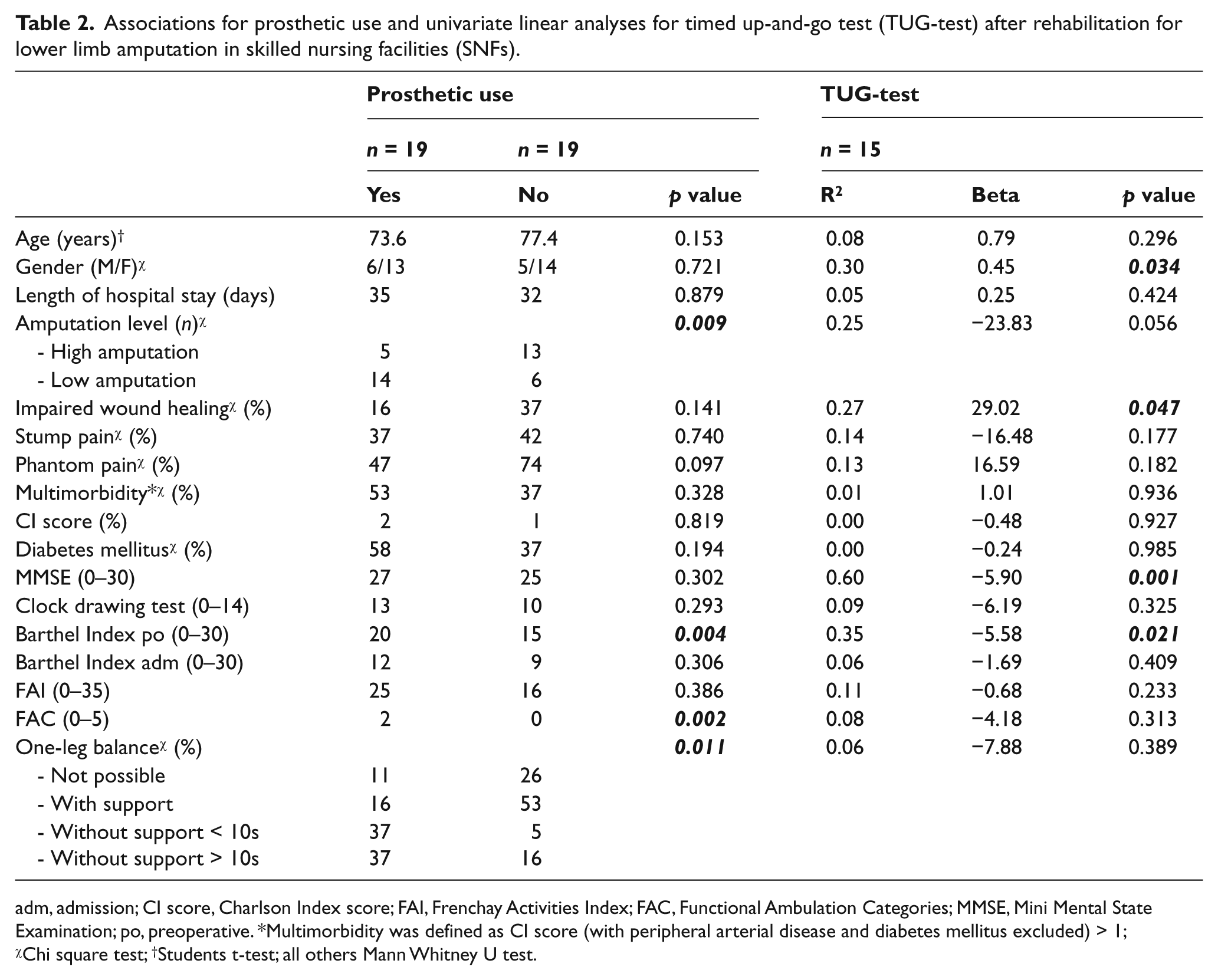
adm, admission; CI score, Charlson Index score; FAI, Frenchay Activities Index; FAC, Functional Ambulation Categories; MMSE, Mini Mental State Examination; po, preoperative. *Multimorbidity was defined as CI score (with peripheral arterial disease and diabetes mellitus excluded) > 1; χChi square test; †Students t-test; all others Mann Whitney U test.
Multivariate logistic regression analysis revealed low amputation level, the absence of phantom pain, and high FAC score to be independently associated with the use of a prosthesis, with a total explained variance of 55.6% (Table 3). The TUG test had a total explained variance of 81.7% with the MMSE, amputation level, and preoperative BI as independent correlates. The MMSE was the most important determinant of TUG test at discharge (Table 3), accounting for nearly 60% of the explained variance.
Multivariate analyses for prosthetic use and timed up-and-go test (TUG test) of lower limb amputees in SNFs.
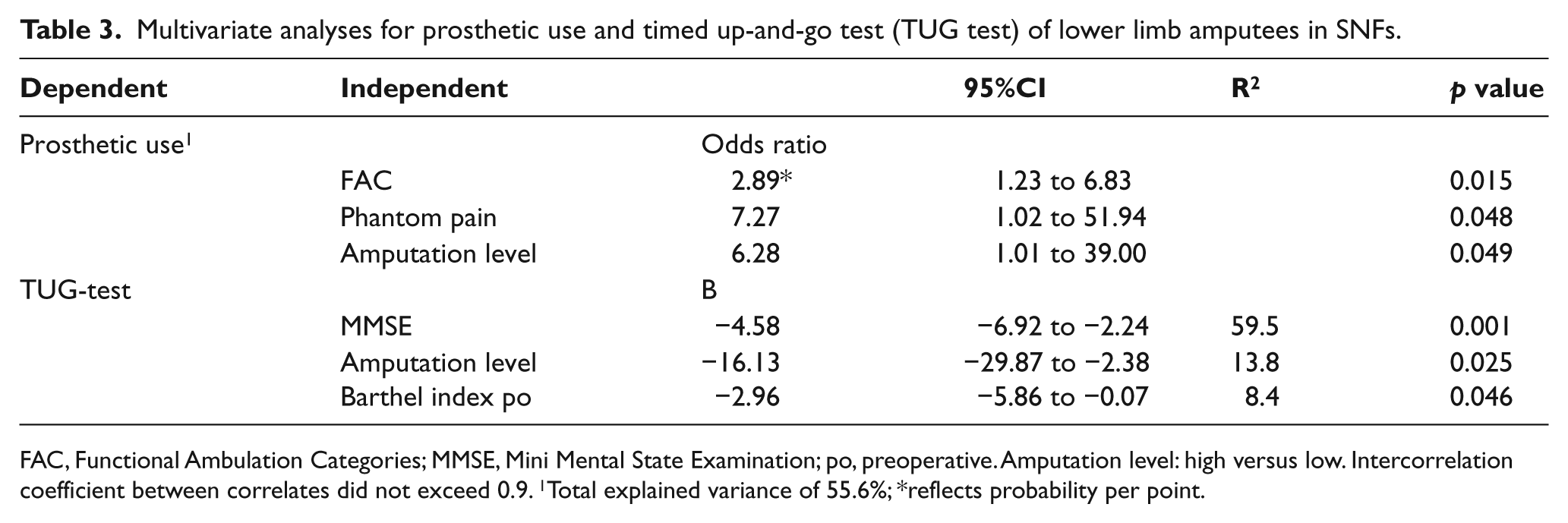
FAC, Functional Ambulation Categories; MMSE, Mini Mental State Examination; po, preoperative. Amputation level: high versus low. Intercorrelation coefficient between correlates did not exceed 0.9. 1Total explained variance of 55.6%; *reflects probability per point.
Discussion
In this study, we found that good functional ambulation on admission, the absence of phantom pain, and low amputation level were independently associated with using a prosthesis after rehabilitation, while good cognition on admission, low amputation level, and preoperative functional independence are highly predictive for functional use of a prosthesis, accounting for almost 82% of the variance of the timed up-and-go test. Multimorbidity, which was hypothesized as being an important factor in determining prosthetic use, did not contribute significantly.
Pre-operative functional ability is important in predicting walking ability after lower limb amputation. Patients with a premorbid limitation in ambulation are not likely to walk with a prosthesis. 5 In contrast, postoperative functional ability does not seem to be related to prosthetic outcome. 14 Leung et al. 28 found that the motor subscore of the functional independence measure (FIM) nor the FIM total score on admission was correlated to prosthetic use in their sample of 33 patients with lower limb amputation. However, in the present study, ambulation ability after amputation was an important factor determining prosthetic use. Six of the seven patients that had an independent ambulation on admission (FAC > 3) received a prosthesis for walking. Consistent with the literature, we found preoperative BI, rather than postoperative BI, to be independently related to prosthetic use. Apparently, when looking at the postoperative functional situation it is useful to evaluate ambulation, rather than global functional assessment.
Good cognitive abilities are a consistent factor, in the literature, predicting prosthetic use. Larner et al. 9 underlined the importance of learning skills in order to adequately use a prosthesis after major limb amputation. Others established a significant relation between cognitive abilities and the level of achieved mobility.3,29,30 Furthermore, patients with dementia have low probability of wearing a prosthesis, and should be grouped with bedridden patients, who usually are best served with a palliative TFA, according to Taylor et al 5 However, the outcome of patients with dementia with a knee disarticulation (KD) is not clear. The surgical procedure is less traumatic, 16 with the preservation of the thigh muscles, and therefore, patients with dementia could benefit from a KD instead of performing a TFA. 31 Cognitive abilities, in this study, were a major determinant of the TUG test. However, they did not significantly contribute to having a prosthesis. This is probably due to the definition of prosthetic use in our study; meaning that prosthetic use is ranging from transfer only/short distances (SIGAM B) to maximum walking ability outdoors (SIGAM F).
Amputation level is a known predictor for rehabilitation outcome and prosthetic use. Patients with a more distal amputation level achieve better walking abilities than patients with a higher amputation level.5,7,13,32,33 The main reason for this finding probably is that the energy required for walking with a prosthesis after TFA is significantly higher compared to walking with a prosthesis after TTA.10,34 At the same time, this energy level may be negatively affected by other physical disabilities in elderly patients with an amputation.
Phantom pain is a common complication of limb amputation with high morbidity rates. 35 Some authors have suggested that prosthetic use alleviates phantom pain, 36 while others described increased pain sensations after prosthesis fitting. 37 Schoppen et al. 3 did not find any association between stump and/or phantom pain and prosthetic use in their sample of elderly patients. The presence of phantom pain, rather than the presence of stump pain, was independently associated to prosthetic use, in the present study.
Surprisingly, multimorbidity was not independently related to prosthetic use. Other authors did find an association between comorbidity and prosthetic outcome,3,4,12,13 but none of these studies have used a standardized comorbidity questionnaire. They focused on specific diseases or organ-system impairments. Multimorbidity was defined as having a Charlson index score of more than 1, modified for amputation. This implicates that at least two more diseases, besides the index disease of PAD with or without DM, were present. This definition of multimorbidity was not arbitrary and has been used in other research, such as stroke research. 21 Multimorbidity was, in this study, evenly distributed between patients with, and patients without, a prosthesis. Therefore, it could not give an independent contribution to prosthetic use. Further research about the influence of multimorbidity on prosthetic use in all age groups is still necessary.
An issue, not fully addressed in this paper, is whether geriatric patients with a lower limb amputation are best served in a ‘low intensity’ rehabilitation program provided in SNFs, or if they could achieve better results in a specialized rehabilitation center. The presence of multimorbidity is not a good outcome measure. Apparently, the preoperative functional status has a strong relationship with rehabilitation outcome and, thus, gives a better understanding of the outcome compared to the number of interacting diseases. 38 The most important reason for admission to a low intensity rehabilitation program in SNFs is not the multimorbidity per se, but the existence of a fine balance between functioning and the decline of functional reserve, which makes an individual frail. Usually, frailty is accompanied by multimorbidity and high age. 39 Low intensity rehabilitation, combined with the specific skills of geriatric problems, is best addressed in SNFs. On the other hand, the number of patients annually admitted for rehabilitation in SNFs is low. In this study, only 55 patients were admitted to 11 SNFs in a period of one year, questioning the maintenance of appropriate quality for prosthetic training of the multidisciplinary team.
This is the first multicenter cohort study that aimed at identifying predictors for prosthetic use in elderly patients that rehabilitate in SNFs. Unlike other researchers, 7 we excluded the patients who died from the analyses. All patients that were admitted for rehabilitation after major lower limb amputation were eligible, and only a few dropped out because of legal incapability, not giving informed consent, or minor amputation. The excluded patients did not differ from the study population in terms of age or gender. The borderline significant difference in rehabilitation length of stay is largely due to the limited stay of the patients with minor amputations and the low number of excluded patients. No significant influence of SNFs on outcome measures was found, which underscores the comparability of patient groups, interventions and assessment procedures.
Some limitations warrant further consideration. First, the small number of included patients in this study is a major limitation. Despite this, the regression analyses revealed significant independent correlates, although with large confidence intervals. Second, although in line with the literature, the results of the preoperative BI should be carefully interpreted, because of possible recall bias. The preoperative BI was assessed on admission to the SNF. Usually, the patient was accompanied by their partner, which gives a lower chance of recall bias. Third, gender and amputation level distribution is different compared to the literature. In our predominant female population, there was a high number of TFA. However, in their statewide hospital discharge study, Dillingham et al. 40 described that patients discharged to an SNF were more likely to be older, female and with a higher level of amputation. Lastly, we did not assess the influence of disease, or the interactions between diseases, during the rehabilitation. These so-called intercurrent diseases also play an important role in the functioning of patients and, therefore, influence the rehabilitation process and probably the rehabilitation outcome.
The results of this study can offer clinicians helpful information in the decision-making process of providing a prosthesis after major lower limb amputation in geriatric patients. Geriatric patients with good ambulation after amputation, no phantom pain, and a low amputation level have a fair chance of using a prosthesis and should be given the opportunity to receive prosthetic training. Furthermore, good cognitive abilities, low amputation level, and preoperative good functional status predict physical mobility with a prosthesis. In conclusion, the results of this study indicate that elderly patients admitted for prosthetic training to SNFs are also able to successfully use a prosthesis.
Footnotes
Funding
This study was funded by two Dutch care organizations Zorgboog and SVRZ. Additionally, a grant was received from the science promotion foundation for nursing homes (SWBV).
Conflict of interest
The organizations that sponsored this study were not involved in its design, data collection, data processing, or manuscript preparation. None of the authors have financial or personal conflicts of interest.