
Abstract
Background and Aim: Until recently, robotic devices for stroke rehabilitation had multi-joint designs that were often tethered to a treadmill for gait training. A new single-joint wearable robotic knee orthosis (RKO) has been designed that provides patient-initiated powered-assistance in untethered functional mobility. This case-series documents application of the wearable RKO in untethered functional training with stroke survivors.
Technique: Three ambulatory adult stroke survivors used a wearable RKO during 18 one-hour sessions within a six-week physical therapy programme. Subjects were assessed with a variety of balance, gait and functional tests including the Berg Balance Scale (BBS); six-minute walk test (6MWT); and Emory Functional Ambulation Profile (EFAP) at pre-treatment, post-treatment, one-month and three-month follow-up.
Discussion: All subjects improved balance, gait and functional performances with mean individual improvements of 12.6% for BBS, 12.0% for 6MWT and 16.7% for EFAP post-treatment. No adverse events occurred. These three stroke survivors may have benefited from the task-specific functional training programme augmented by RKO use.
Physical therapists may find a wearable robotic knee orthosis useful for providing patient-initiated assisted movement for ambulatory chronic stroke survivors during functional task-specific balance and mobility training.
Background and Aim
Stroke is a leading cause of long-term disability with over one million survivors reporting gait and balance impairments that led to persistent limitations and lower functional ability.1-3 Half of stroke survivors report hemiparesis and over 30% require assistance with gait. 4
Various rehabilitation approaches improve balance and gait function after stroke. Functional strengthening through sit-to-stand training can improve balance. 5 Over-ground gait training can improve walking speed, though effect sizes are small. 6 Greater increases in gait speed have been reported after high intensity body weight-supported treadmill training, 7 which allows longer treatments that benefit cardiovascular fitness and endurance. 8 However, being tethered to a treadmill limits concurrent training of functional tasks and gains made in treadmill training may not transfer to untethered daily functional tasks. This may explain why task-oriented training, focusing on specific activities like stairs and transfers, has yielded the strongest evidence and largest effect sizes for functional gait, with gains maintained after two months. 9
Some stroke survivors require orthotic intervention for optimal gait. Studies demonstrate that wearing an ankle-foot orthoses (AFO) after stroke can benefit gait speed,10,11 though lack of large controlled studies make consensus elusive. 8 Robotic hip-knee-ankle-foot orthoses (HKAFO) have been developed for stroke survivors to augment treadmill training,12,13 but tether the individual to the treadmill, limit functional task-oriented training, and provide less benefit than therapist-assisted training without the orthosis. 14 A robotic orthosis that could be worn during untethered functional activities may benefit rehabilitation after stroke.15,16
The weight of a wearable robotic orthosis could negate the benefit of mechanically-assisted movement. While no negative effects occurred in stroke survivors walking with an unpowered robotic KAFO, 17 neither was any benefit derived from wearing a robotic HKAFO for a single stroke survivor after over-ground and treadmill walking training. 12 To reduce the weight and complication of robotic orthoses that incorporate multiple joints, a wearable robotic knee orthosis (RKO) spanning only the knee has been introduced that provides mechanized-knee extension assistance to patient-initiated functional movement but weighs only half as much. 18
Wearable robotic lower-limb orthoses have been designed for, but not typically tested with, those with hemiparesis.15,16,18 The wearable RKO has been introduced but specific clinical results from use with any patient population remain lacking. The purpose of this case-series was to document use of the new wearable RKO with three chronic stroke survivors for untethered over-ground balance, gait and functional training.
Technique
Subjects
Three stroke survivors recruited from a rehabilitation research registry gave informed consent to participate in this study, approved by the Columbia University Medical Center Institutional Review Board. All subjects had one stroke, confirmed by imaging, with resulting gait alterations at least six months later (Table 1) and were receiving no treatment affecting leg strength. Subjects could actively move their leg and ambulated independently. Exclusion criteria included: other neurologic disorders, excessive plantarflexor spasticity (Ashworth Scale >3), absent leg sensation (score of 2 on NIH Stroke Scale item #8), uncontrolled hypertension, unstable coronary artery disease, lower-limb contractures preventing neutral position, impaired cognition (Mini-Mental Status Exam score <24) or medical conditions preventing participation.
Subject information.
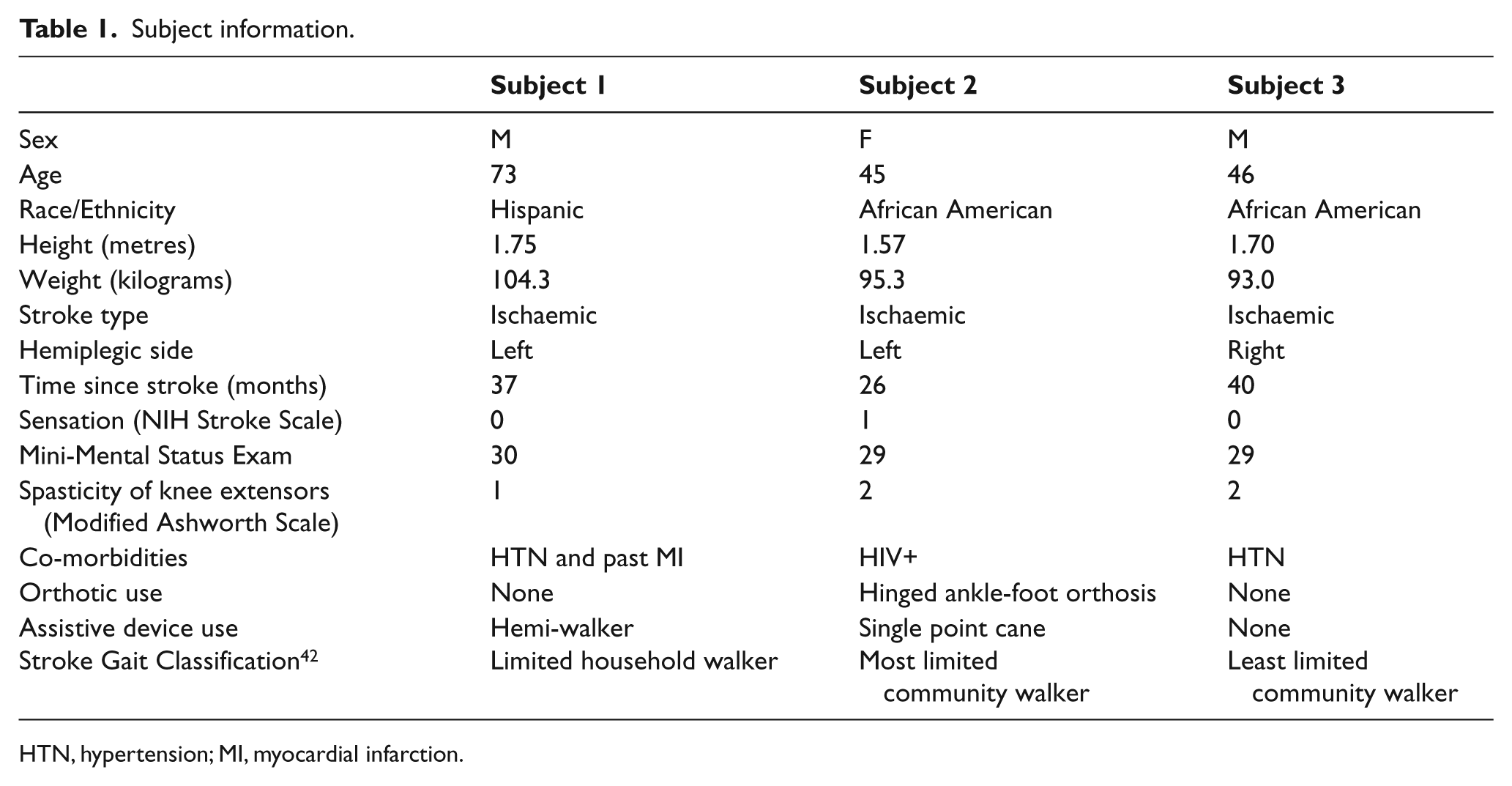
HTN, hypertension; MI, myocardial infarction.
Design
This pre-post treatment case-series, assessed balance, gait and functional ability:
re-treatment
ost-treatment
at one-month follow-up
at three-months follow-up
Device
The Tibion Bionic Leg (Tibion Corporation 247 Santa Ana Court, Sunnyvale, CA 94085 www.tibion.com) is a wear-able RKO that provides mechanized-assistance to patient-initiated active movement. 18 The RKO has a flexible plantar pressure-sensing shoe insert; loose-fitting plastic ankle straps attaching the shoe insert without providing ankle support, leg and thigh uprights, single-axis knee joint with angle sensors; textile straps secured with zippers, Velcro and adjusting knobs; onboard actuator motors with control panel housing; and rechargeable lithium battery. The long lever design with full length Velcro straps minimize migration during use of RKO alignment; which was assessed by observation of patellar alignment in the anterior opening of the RKO (Figure 1). Designed to support patients weighing over 100 kg, the RKO weighed 3.7 kilograms 18 and required five to eight minutes to don and doff.

Using the Tibion Bionic Leg, a wearable robotic knee orthosis, for transfer training with a man after stroke.
The RKO uses plantar pressure, angle and actuator torque sensors to determine the assistance level and timing needed during activity. Plantar pressure sensors detect gait phase based on sequence and timing of heel-toe weight-bearing. Angle sensors determine knee motion angles. Actuator torque sensors determine knee torque. A proprietary formula incorporating amount and distribution of forces, in the context of an internal gait-prediction algorithm, defines knee state and function thus determining which knee extension assistance mode is applied. During stance phase, stair ascent or sit-to-stand movements, the knee actuator actively assists concentric extension. At toe-off, during swing phase or in non-weight bearing, the actuator decouples to allow free knee swing. At heel strike, stair descent or stand-to-sit, the knee actuator resists knee flexion by providing an eccentric knee extension torque. Patient-initiated knee extension with weight-bearing triggers mechanically-assisted knee extension according to predetermined assist or resist factor parameters – expressed as a percentage of the total required knee extension force – calculated with the proprietary formula. Redundant foot sensors provide normal operation despite connection or sensor failure. 18
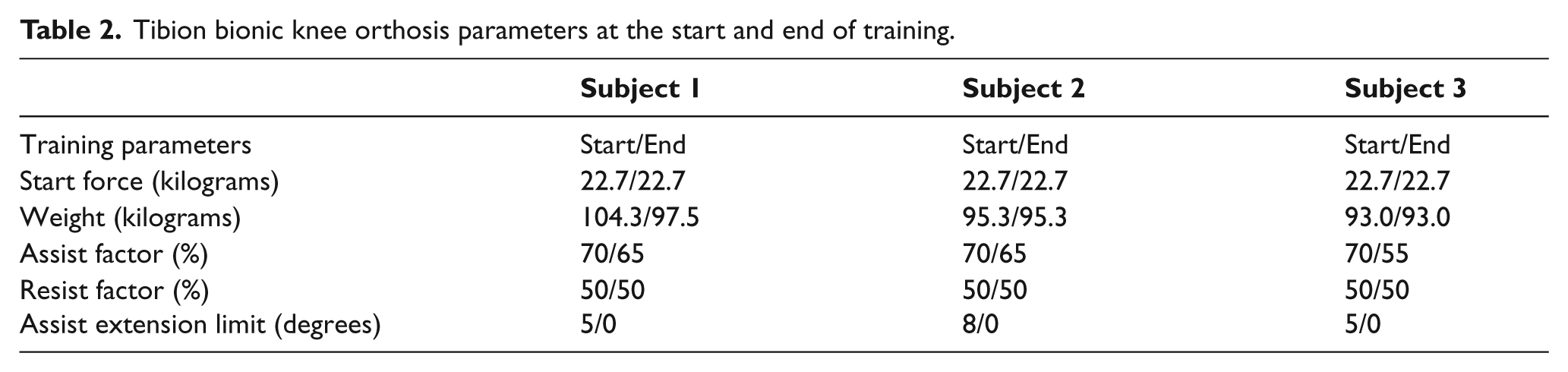
Resistance and timing parameters were set and updated by a trained physical therapist based on individual patient performance (Table 2). Parameters included:
weight: patient’s body weight;
start force: weight on foot plate required to initiate the powered-assist;
assist factor: amount of knee extension assistance provided;
resist factor: amount of knee extension assistance provided during knee flexion;
assist extension limit: degree of extension through which assistance is provided. This feature helps limit knee hyperextension when present.
Tibion bionic knee orthosis parameters at the start and end of training.
Procedures
The robot-assisted physical therapy training programme included 18 sessions conducted three times per week for six weeks (Table 3). Each one-hour session included approximately 45 minutes of training wearing the RKO and brief rest when needed. One physical therapist with stroke rehabilitation and Tibion RKO experience conducted all training sessions. The RKO was not provided for home use.
Tibion robotic knee orthosis physical therapy training plan.
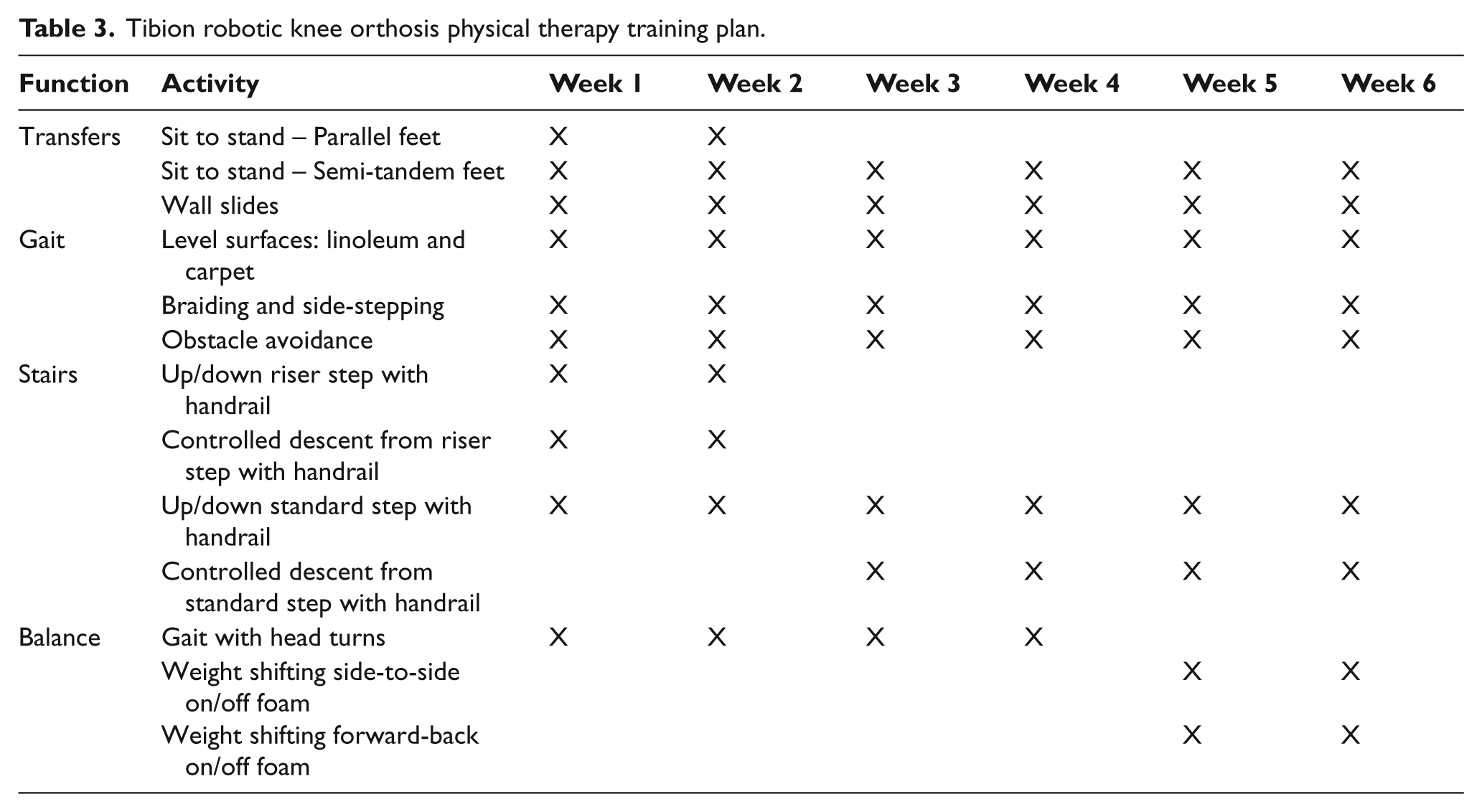
Sessions included standardized weight-bearing functional mobility activities designed to develop functional strength, balance, gait and endurance. Activities included sit-to-stand transfers; static and dynamic standing balance; gait with various surfaces and speeds; and mobility on stairs, around obstacles, and in functional tasks. If RKO migration occurred during use, the physical therapist corrected patellar alignment before continuing the training, though no measures were taken. All activities were performed to individual ability using each subject’s assistive device but no AFO consistently throughout (Table 1). As each subject’s abilities changed, RKO parameters (Table 2) and training activities were modified (Table 3). After the six-week programme, RKO use was discontinued. No special instructions were given during the follow-up period and subject activity was not monitored.
Clinical measures
The balance, gait, and functional ability of each subject while not using the RKO were assessed by one physical therapist not involved in treatment and blinded to past results. Latin square randomization insured that test order differed for each subject. 19 Two-minute rests were provided between each assessment.
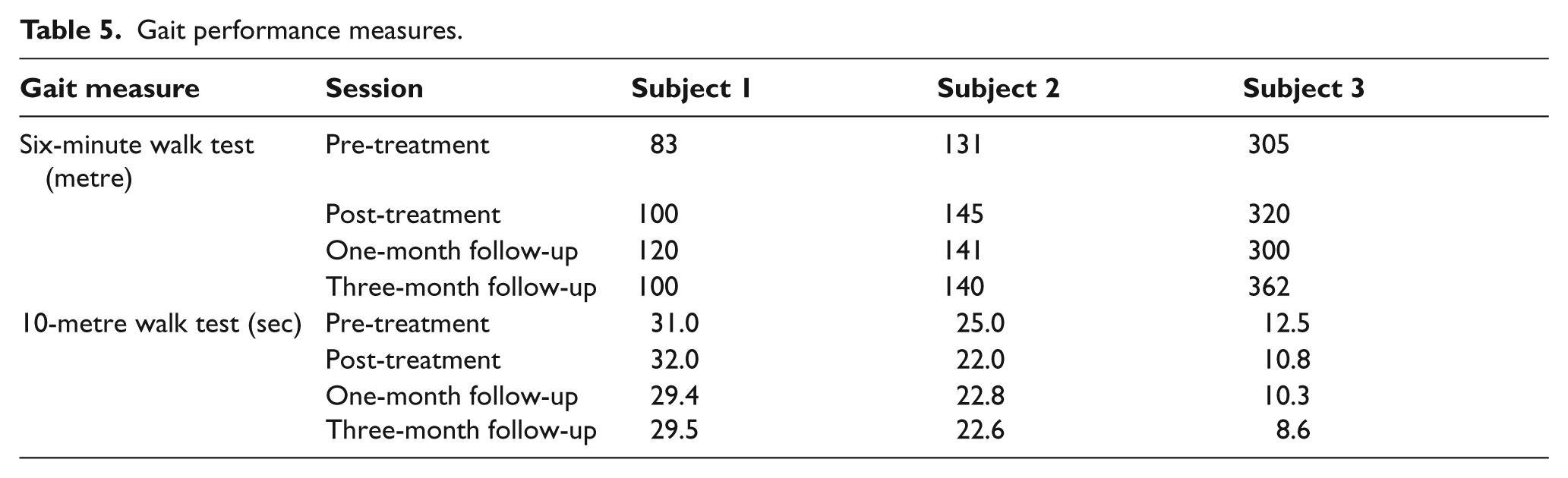
Balance was assessed using the Berg Balance Scale (BBS), consisting of 14 tasks, including a Romberg test, rated on a 0-4 scale and then summated. 20 The BBS has moderate 21 to excellent reliability 20 and excellent validity compared to other functional measures in stroke survivors. 22 The BBS has identified both community-dwelling 23 and inpatient stroke survivors at risk to fall, 24 and documented improvements even six months after stroke.25,26 Gait speed was assessed with the 10-metre walk test (10MWT) 27 and gait endurance with the six-minute walk test (6MWT). 28
Function was assessed with the five-time sit-to-stand test (5TSST) and Emory Functional Ambulation Profile (EFAP) – that includes Timed-Up-and-Go (TUG). The 5TSST correlates with leg strength and has excellent reliability. 29 The TUG combines sit-to-stand, gait initiation and turn-while-walking, 30 and has good reliability 31 particularly in chronic stroke survivors. 32 The EFAP includes five-timed tasks including TUG, stair negotiation, carpet and tile walking, and obstacle avoidance, and is a reliable and valid measure of functional walking ability in stroke survivors21,33,34 with excellent reliability 34 and responsiveness-to-change. 21 The self-report California Functional Evaluation (CAFE 40) assessed functional health status. 35
Statistical analysis
Only descriptive data were reported due to the small sample size. Percent change for each subject was calculated to show within subject change.
Discussion
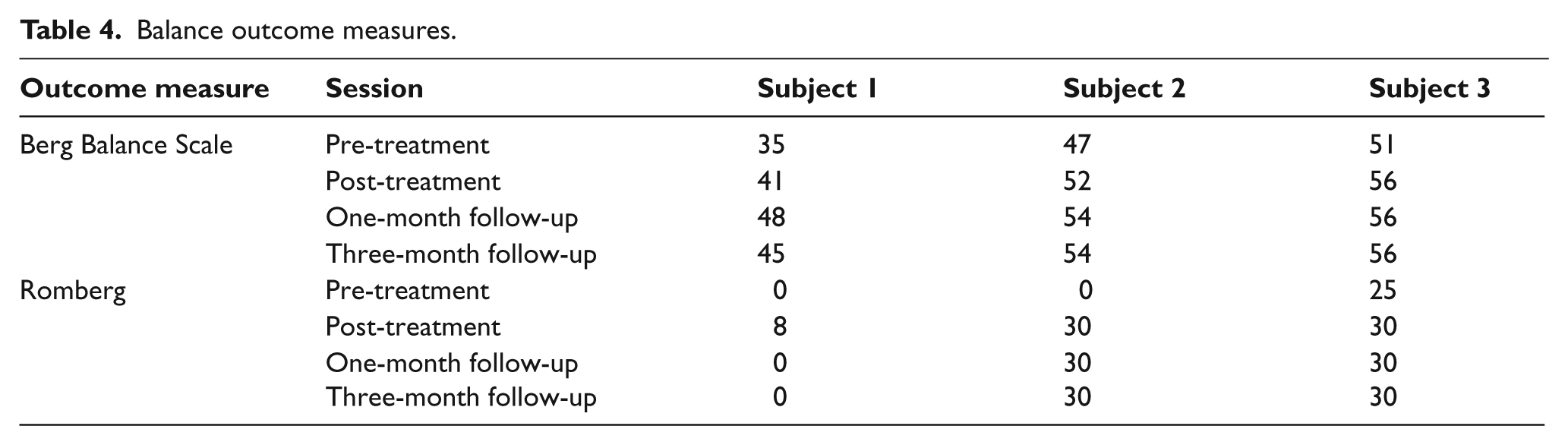
After RKO training, all three subjects demonstrated improvements without RKO on balance, gait and functional outcome measures (Tables 4–6). All three subjects improved in every outcome measure post-treatment except for Subject 1 whose 10MWT time increased by one second. Improvement was demonstrated after treatment for all measures except for the TUG time for Subject 2 and the self-report functional assessment for Subject 1, who injured his knee two days before the three-month follow-up. No adverse events, such as skin breakdown, falls or injury, occurred during RKO treatment. This case-series introduced the use of a wearable one-joint RKO in physical therapy for chronic stroke resulting in improved balance, untethered over-ground gait, and functional performance for all three subjects. All subjects improved their BBS scores by 5 to 13 points, representing true change. 36 Two subjects’ BBS scores improved above the 52 to 54 point cut-offs that predict falls with highest sensitivity and specificity in community-dwelling elderly 37 and stroke survivors 23 ; and two subjects initially unable to perform the Romberg test succeeded after treatment (Table 4). All subjects also improved gait speed and endurance post-treatment, with average gains of 7.5% (10MWT) and 12.0% (6MWT). Stroke survivors do not consistently maintain gait speed and endurance gains after rehabilitation 38 especially after three months,39,40 but gains in this case-series were maintained for all subjects (Table 5). Functional performance generally improved for all subjects. Although Subject 2 performed the TUG one second slower, all subjects improved EFAP times, which included the TUG time. Subject 2 was unable to perform the 5TSST before or after training; the two subjects able to perform the 5TSST improved by a mean 9.4% post-treatment.
Balance outcome measures.
Gait performance measures.
Functional performance measures.
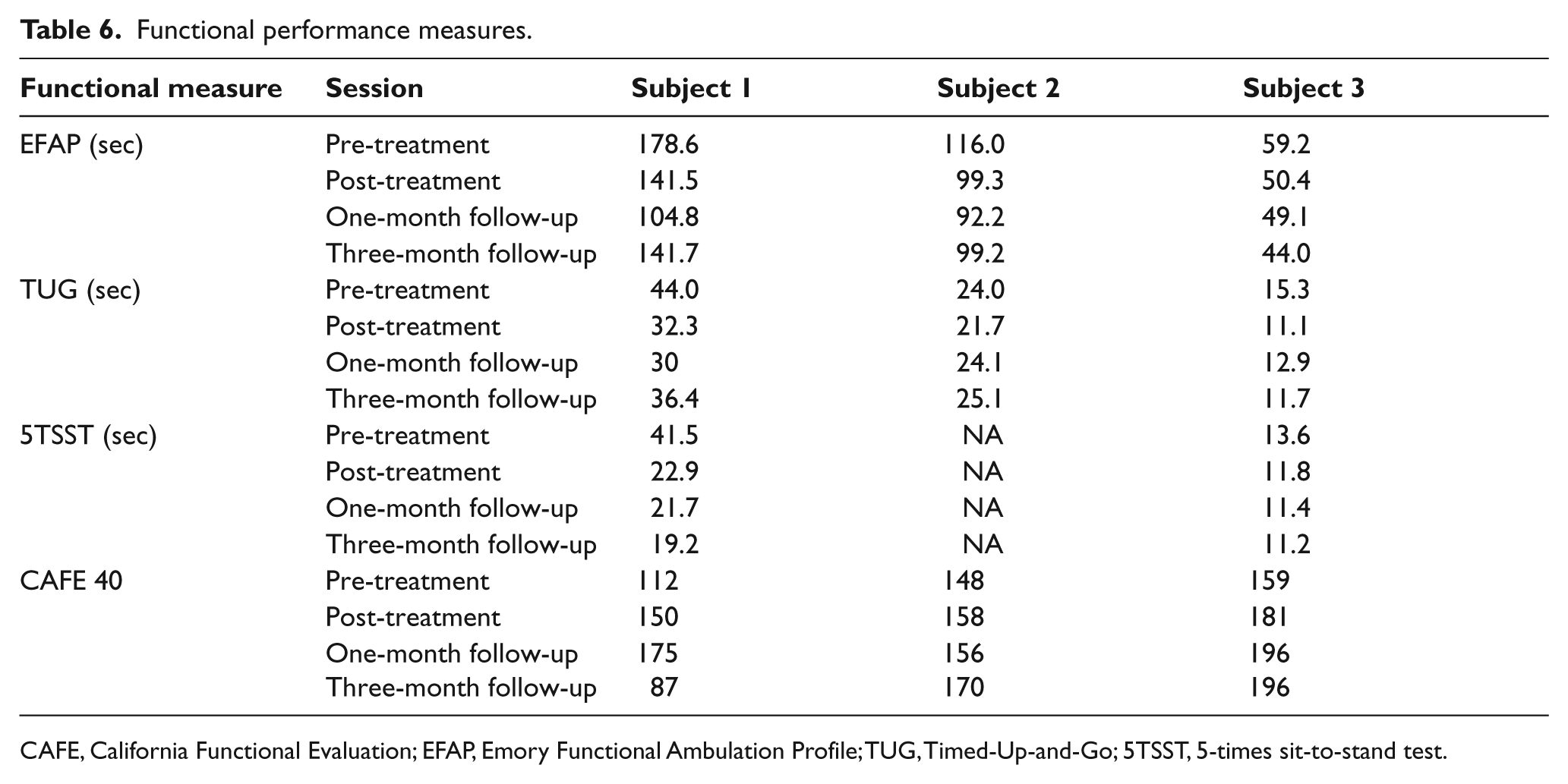
CAFE, California Functional Evaluation; EFAP, Emory Functional Ambulation Profile; TUG, Timed-Up-and-Go; 5TSST, 5-times sit-to-stand test.
Observed balance improvements may be due to emphasizing balance and untethered functional activities in treatment and post-treatment BBS scores suggest a decreased fall risk.23,37 Subjects reported more feeling in their leg during weight-bearing activities, but no data support this subjective claim. The wearable RKO made it possible to perform untethered robot-assisted task-specific functional training, which may have facilitated transference of training that benefited their independent functional performance without the RKO. 9 Furthermore, task-specific training in activities including, stairs, obstacles and transfers may have positively affected performance on functional tests that included those activities.
Wearable robotic leg orthoses reported in stroke rehabilitation have had multi-joint designs that are more restrictive and twice as heavy as the single-joint RKO.12,17,18,41 The light-weight RKO in this case-series was used with stroke survivors who could actively move their leg and ambulate independently, though it can be combined with passive AFO for those with ankle instability. While this may have encouraged more weight-bearing training and potentially stimulated more activity and cardiovascular training than possible without an RKO, the knee extension assistance appeared insufficient to enable one subject to rise without using hands. Stroke survivors who require powered assistance for hip movement might find the one-joint RKO insufficient. While simple for the physical therapist to apply, the weight and complexity of the RKO may inhibit independent patient use or continual wear, and may be most convenient for unilateral use. Minor migration of the RKO occurred during training for Subject 2, without deleterious effects such as skin breakdown, and was corrected before continuing training. RKO migration can result in mal-alignment of the anatomical and orthotic knee joint axes, which could inhibit normal knee flexion. The RKO does not assist active knee flexion and subjects were observed at times to have decreased swing phase knee flexion ascending stairs wearing the RKO, which matched the observation by others during robotic KAFO use of similar weight in over-ground training. 17
The results of this case-series cannot be generalized beyond these subjects and should be considered only as descriptive. Study limitations include recruitment from a database of stroke survivors interested in participating in research that may have biased selection towards motivated higher functioning individuals, variation of subject motivation or functional status among the study time points, lack of independent subject activity assessment, and lack of kinetic and kinematic gait analysis. The case-series design precludes drawing any conclusions. Therefore, future research into patient criteria for use, costs, benefits, risks and potential adverse events should be conducted to determine feasibility for larger studies that could explore RKO use in in-patient, out-patient, home-care, or independent-use settings; for subjects with stroke or other diagnoses; and at different functional levels. Controlled designs including comparison groups receiving no-treatment, robotic treatment without physical therapy, or physical therapy without robotic treatment are required to determine effects of RKO use in stroke rehabilitation.
In conclusion, a wearable RKO for over-ground functional physical therapy programme was safely used by three stroke survivors. This case-series suggests that using the RKO to augment untethered task-oriented physical therapy may have benefited the stroke survivors in this study.
Key Points
This case-series is the first to document Tibion RKO use in a patient population.
The Tibion RKO was safely used as an adjunct to stroke rehabilitation.
The RKO provides clinicians with a new option that may be beneficial in untethered over-ground functional training outcomes for some stroke survivors.
Footnotes
Funding
This research was partially funded by the Tibion Corporation, which provided the devices needed for the duration of the study.
Conflict of interest
The authors declare that there is no conflict of interest. The authors alone are responsible for the content and writing of the paper.