
Abstract
Background and Aim: In order to increase understanding of the biomechanical consequences of equinus foot on gait, we developed an orthosis to induce an adjustable degree of unilateral equinus. The aim of this study was to evaluate its feasibility and consequences on 3D ankle kinematics and kinetics.
Technique: 3D gait analysis was carried out in 10 healthy children without the orthosis, with the non–adjusted orthosis and with the orthosis adjusted to +10°, 0°, −10°, −20° of ankle dorsiflexion and maximum plantarflexion (MP). The amount of dorsiflexion at initial contact was close to the goniometric measurement. Significant kinematic and kinetic changes occurred at −10°, −20° and MP. The mean maximum equinus at initial contact −21.65° ± 4.17 and during stance −11.61° ± 4.82 were larger than those obtained with previous described devices.
Discussion: Our device was easy–to–use and induced an adjustable, well tolerated equinus. It provides a new way to simulate equinus and its biomechanical consequences on gait.
This study validated an orthotic device which induced an adjustable equinus. This device can be used to carry out biomechanical studies in children, increasing understanding of pathological problems and thus improving therapeutic management.
Background and Aim
Foot equinus frequently occurs in children with neurological disorders. 1 It is characterized by plantarflexion of the ankle causing toe strike and reduced dorsiflexion during swing phase of gait. Equinus can be dynamic (due to dorsiflexor weakness or spasticity of soleus and/or gastrocnemius) or fixed (due to joint or muscle stiffness). 3D quantitative gait analysis can be used to determine the primary causes of equinus and the biomechanical consequences on both lower limbs 1 thus aiding therapeutic management. In order to improve understanding and therapeutic management, many authors have tried to simulate equinus.2–6 These studies involved healthy adults simulating unilateral or bilateral toe-walking,2,4,5,7 cadaver models, 8 muscle-based models, 9 strapping 3 or orthosis.5,7 The main limitations of these studies were that:
the degree of the equinus was not controlled, reducing the clinical applications of the findings;
it is difficult to obtain a large degree of plantarflexion during the whole stance phase;
although therapeutic interventions are frequently carried out in children, no data are available in this population.
Thus, we developed a new orthosis which could induce an adjustable degree of unilateral equinus in healthy subjects. The aims of this study were to evaluate the feasibility of using such an orthosis in healthy children, to evaluate the capacity of the orthosis to induce different degrees of equinus, and to evaluate its consequences on 3D ankle kinematics and kinetics.
Technique
Orthosis design
An orthosis was custom molded for each child on the anterior surface of the leg and the dorsal surface of the right foot (Figure 1). Each orthosis consisted of two parts made of semi-rigid polyethylene SIMONA PE-W®. This material is commonly used to make orthotics in children. It is sufficiently rigid to constrain the joint while being flexible enough to allow comfortable gait. The two parts were linked by two anterolateral Gillette ®-type joints. The orthosis was lined with an 8-mm polyethylene layer for comfort and to avoid injury. A turnbuckle linked the two parts and allowed the degree of limitation of dorsiflexion to be adjusted. Plantarflexion was free because of the sliding mechanism of the turnbuckle. Self-adhesive bands were used to fix the device to the leg and the foot.
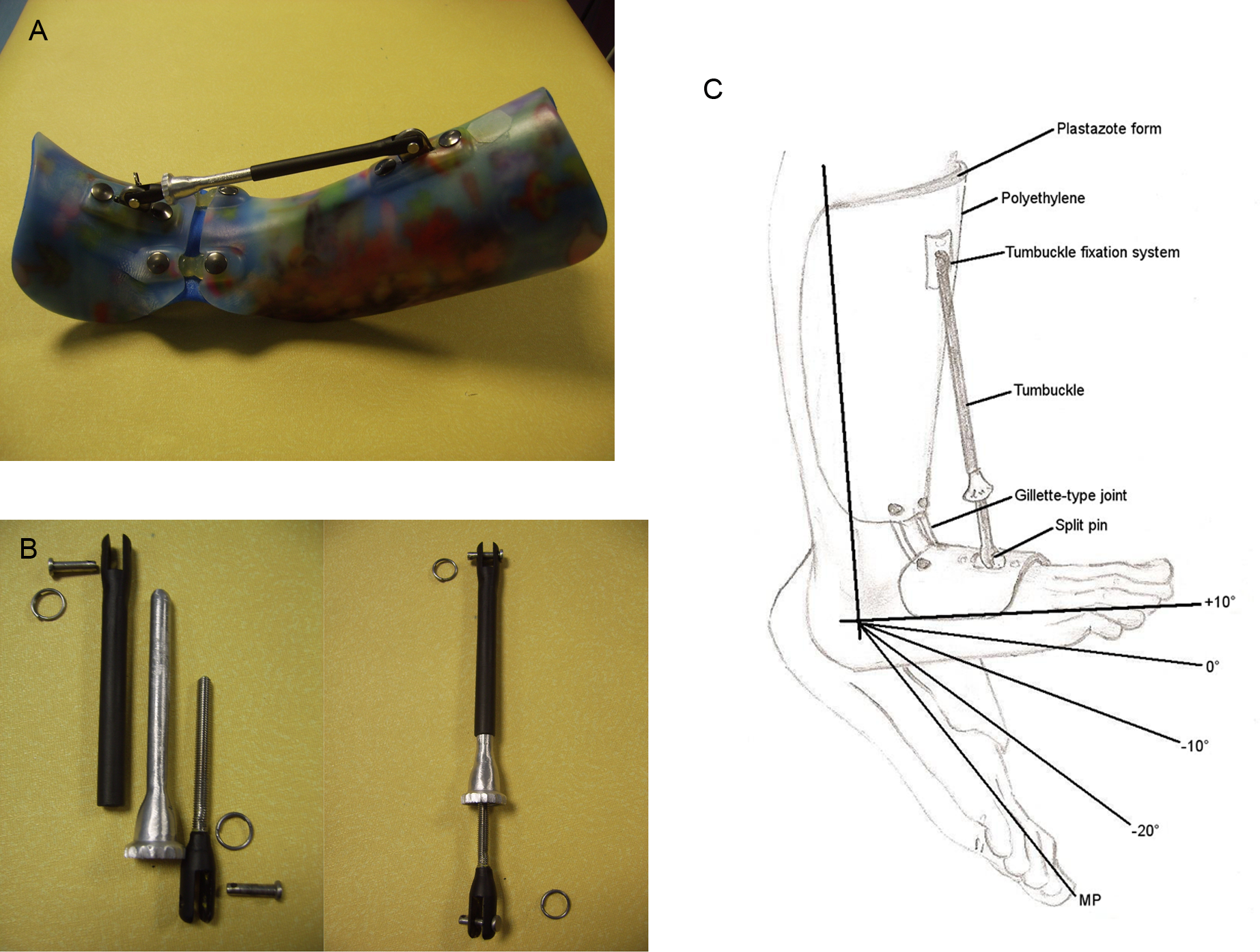
Photograph and diagram of the orthosis. (A) Orthosis (side view). (B) Detailed view of the turnbuckle composed of 3 parts and attachments. The central part slides into the superior part. The inferior part is a screw. The knurl of the central part allows the degree of equinus to be adjusted. The device used without the turnbuckle is the orthosis free (OF) condition. (C) Diagram of the orthosis and the five tested positions of equinus.
Protocol
Spatiotemporal, kinematic and kinetic gait parameters were recorded using an optoelectronic system (Vicon MX 13, Oxford Metrics, Oxford, UK) with nine infrared cameras and two AMTI force platforms 120 cm × 60 cm (Advanced Mechanical Technology Inc., Watertown, MA, USA). A total of 16 reflective markers were positioned on the lower limbs according to the protocol by Davis et al. 10 The markers did not interfere with the orthosis.
Ten healthy children (four females, six males) with an average age of 9.7 years ± 1.25, weight 32.22 kg ± 6.59 and height 1.38 m ± 0.08 were included. The research protocol was approved by our institutional regional research ethics committee. Children and parents signed informed consent for participation and publication. Gait was recorded bare foot without the orthosis (normal gait (NG)), while wearing the orthosis with the turnbuckle removed (orthosis free (OF)), with the orthosis in four successive positions of dorsiflexion limitation (+10°, 0°, −10°, −20°) and at the maximum dorsiflexion limitation allowed by the system (maximum plantarflexion (MP)) (Figure 1). The dorsiflexion angle was determined using a handle goniometer using the proximal and distal part of the fibula and the head of the fifth metatarsal as references. 11 We chose to increase the equinus progressively during the session in order to obtain a better tolerance. To avoid fatigue, children could rest during the adjustment and could interrupt the experiments at any time. All the children carried out the entire protocol without the occurrence of any fatigue.
Each child carried out four 10-meter walks for each angle of dorsiflexion limitation. Since gait velocity influences both kinematic and kinetic parameters of gait 12 a velocity close to 1 m/s was imposed. Using a simple stop watch, trials were discarded if the time differed by more than 10 percent of the imposed velocity (0.09 to 1.10 m/s). There were no statistically significant differences in the spatiotemporal gait parameters between conditions. Each subject walked approximately 50 meters prior to the data collection in order to become accustomed to each new position of the orthosis. No instructions were provided regarding gait strategy.
Data and statistical analysis
Joint kinematics and kinetics were computed using the VICON Plug-in Gait model. 10 Gait kinematics and external joint moments were extracted based on Benedetti’s recommendations 13 and maximal ankle power generation and absorption were calculated with a custom-made program (Table 1). The kinetic data were normalised to subject weight without taking into account the weight of the orthosis (approximately 0.3 kg). Since the sample of children was small and each child was compared to themselves in each condition, a Wilcoxon’s paired rank test (Statistica v 6.0 ®) was used to analyze each parameter. A difference was considered significant when p<0.05.
Mean (and standard deviation) of ankle kinematics and kinetics for each condition.
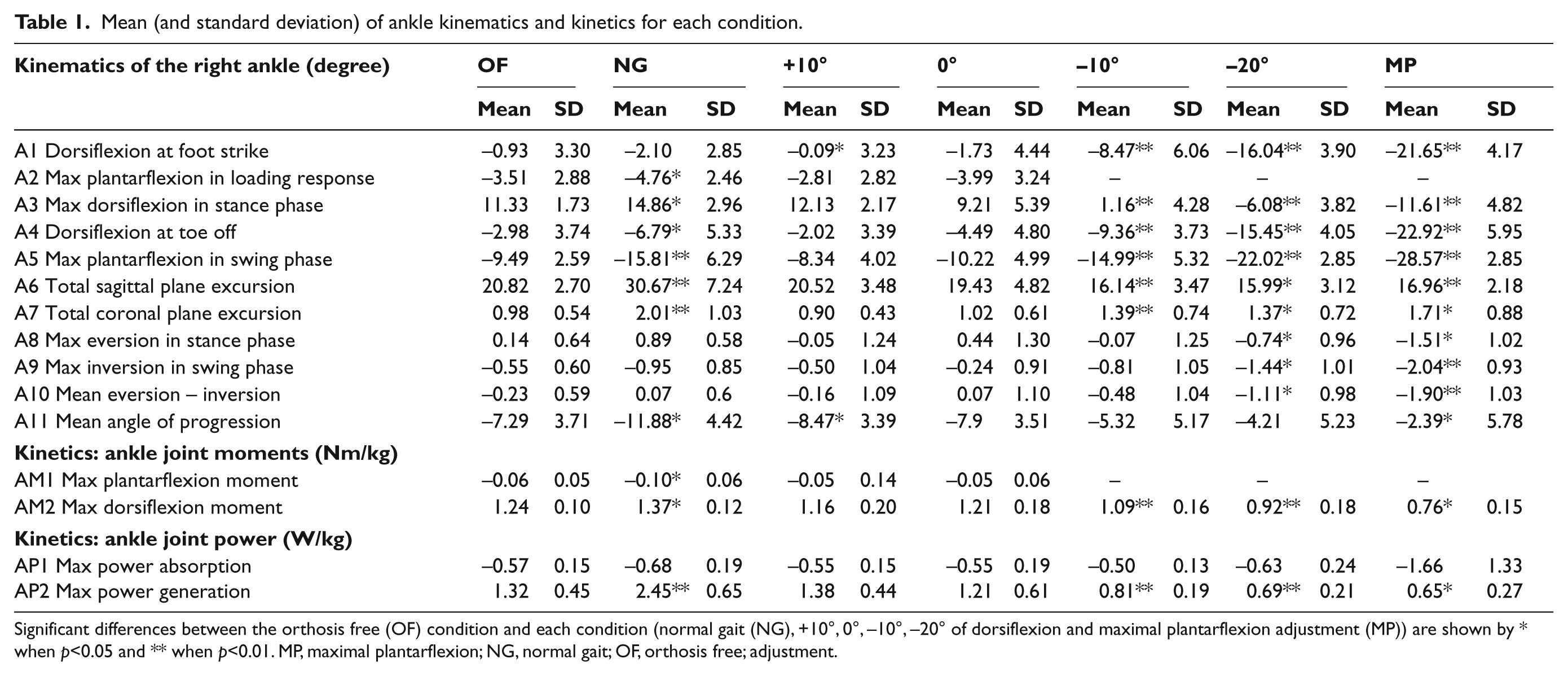
Significant differences between the orthosis free (OF) condition and each condition (normal gait (NG), +10°, 0°, –10°, –20° of dorsiflexion and maximal plantarflexion adjustment (MP)) are shown by * when p<0.05 and ** when p<0.01. MP, maximal plantarflexion; NG, normal gait; OF, orthosis free; adjustment.
Results
The orthosis was well tolerated by the children, there were no complaints of pain but there was slight discomfort at MP. Changes in ankle kinematics and kinetics in the six conditions are shown in Figure 2 and Table 1. Because there were some differences between OF and NG (Table 1), the effects of the different positions of the orthosis were compared with the OF condition.
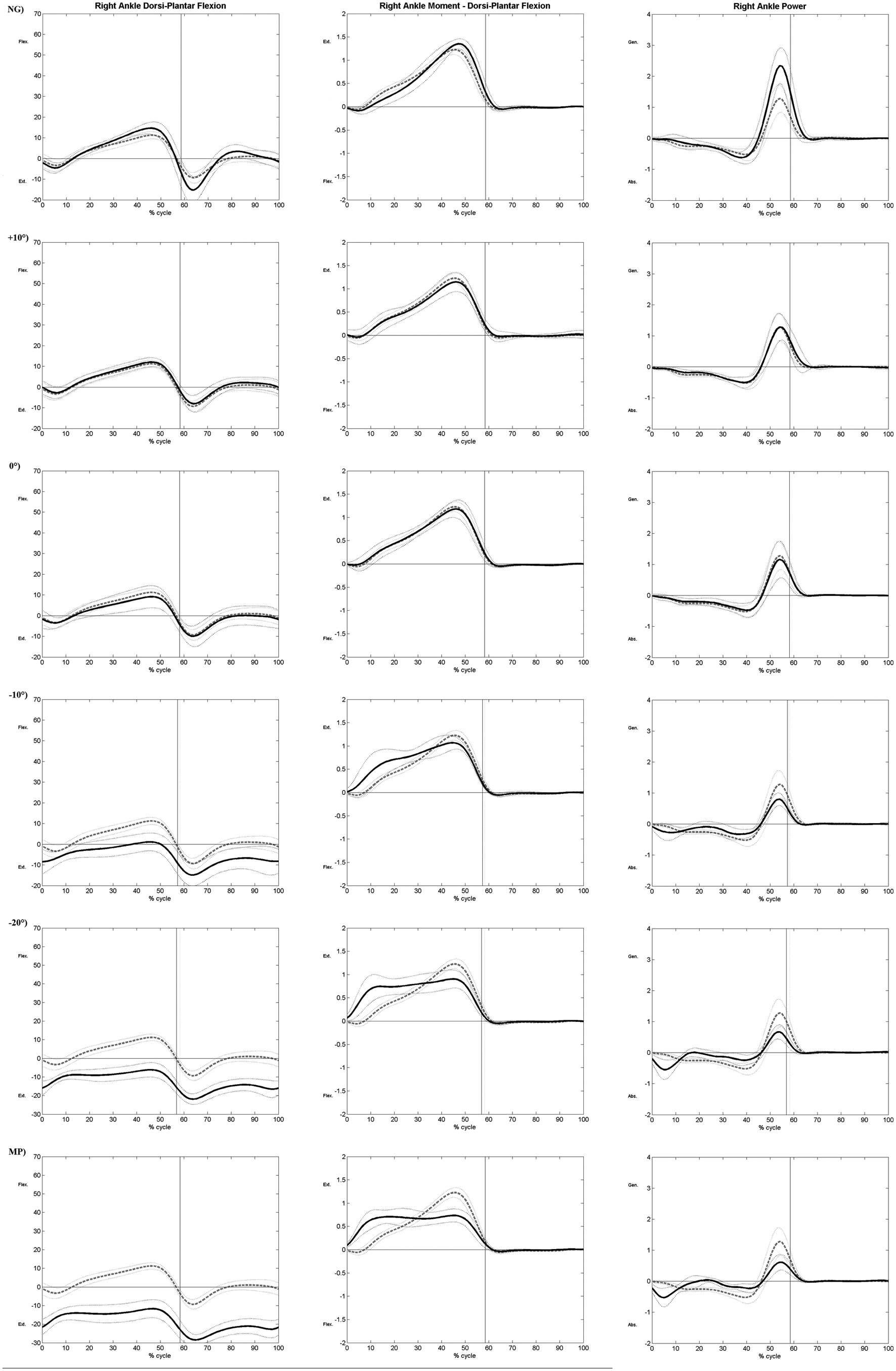
Ankle kinematics (left column), moments (middle column) and power (right column) for each condition. Gray dotted line (mean and standard deviation): orthosis free (OF). Black line (mean and standard deviation): position of the orthosis (normal gait (NG), +10°, 0°, -10°, -20° of dorsiflexion and maximal plantarflexion (MP)).
Kinematic changes were not significant for small limitations of dorsiflexion (+10° and 0°) but became significant from the −10° position. The amount of dorsiflexion at initial contact (A1) was close to the clinical adjustment of the orthosis from the 0° condition (−1.73° at 0°, −8.47° at −10° and −16.04° at −20°).
The amount of plantarflexion measured clinically at the maximum position of the orthosis was −28.22° ± −2.86 and the amount of plantarflexion during gait (A1) was −21.65° ± 4.17. Equinus occurred during stance phase (A3) from the −20° condition. The mean maximum plantarflexion angle obtained during stance phase was −11.61° ± 4.82 at MP. The orthosis allowed plantarflexion to occur during the pre–swing phase of the gait, even at MP. During swing phase, the increased equinus induced a greater maximum plantarflexion angle (A5), from −9.49° (OF) to −28.57° (MP). Changes in the frontal plane were in the order of 1−2° and the mean foot progression (A11) was more internal from −7.29° (OF) to −2.39° (MP).
Similarly to the kinematic parameters, significant kinetic changes occurred from the −10° position. The initial plantarflexion moment (AM1) disappeared and was replaced by an initial dorsiflexion moment. The maximum dorsiflexion moment (AM2) decreased from 1.24 Nm/kg at OF to 0.76 Nm/kg at MP and had a biphasic aspect. Maximum power generation (AP2) decreased from 1.32 W/kg at OF to 0.65 W/kg at MP and, in parallel, a power absorption peak (AP1) occurred from −10° during the loading response.
Discussion
The orthosis was easy to use, well-tolerated, could be adjusted to specific degrees of plantarflexion using the turnbuckle and did not interfere with the markers during gait analysis. The material was sufficiently strong and elastic to impose a ‘comfortable’ equinus. Moreover, this orthosis could be made by any orthotist. The use of a posterior ankle foot orthosis could make fitting of the orthosis on the foot easier, would probably limit the sliding of the orthosis and would allow the use of a lateral joint. However, an anterior device, such as the one used in this study, allows barefoot gait and does not interfere with the positioning of the markers.
To our knowledge, this study is the first to induce unilateral equinus using an external device in children. With regard to kinematic parameters, our system induced a plantarflexion angle of −21.65° ± 4.17 at the MP position. Previous studies in healthy adults found a plantarflexion angle of −18.74°± 5.67 at initial contact in subjects mimicking unilateral toe-walking gait, 6 an angle of −28° ± 6.0 when using a strapping method 3 and of −5.21° ± 4.56 with the device used by Matjacic et al. 5 Our orthosis induced a greater mean maximum plantarflexion angle during stance (−11.61° ± 4.82) than the previous studies (−1.12° ± 4.86 Romkes and Brunner 6 and −7° ± 7.8 Goodman et al. 3 ) and also allowed a positive dorsiflexion angle. 5 During swing phase, our kinematic results were similar to those of previous studies. With regard to kinetic parameters, there was a lack of dorsiflexion moment in initial stance, a bi-phasic plantarflexion moment and a decrease in peak power generation in pre-swing with the orthosis, all of which are coherent with the findings of other studies.3,5,6 At the maximal orthosis position, ankle kinematic parameters were close to those of the hemiplegic gait of children in the study by Winter et al. 14 (true equinus group: about −25° at initial contact and −7° ± 10 in stance phase).
The clinical adjustment of the orthosis using a goniometer yielded a similar degree of plantarflexion at initial contact but was not completely accurate. This could be due to several factors:
the polyethylene provided an ‘elastic’ resistance which induced small variations;
differences between clinical assessment and 3D kinematics are frequently observed, probably due to soft tissue artefacts and the approximations of biomechanical models. 15
Another limitation of the device is that, even when free (the OF condition) it caused small but significant modifications of the gait parameters. These changes consisted mainly of a mean difference of 3.53° less dorsiflexion in stance, 6.32° less plantarflexion in swing and 4.59° less external angle of progression. These differences can be explained by the necessary rigidity of the whole device to create an equinus and especially by the use of rigid Gillette joint and adhesive bands to control the sliding of the orthosis. In order to evaluate the real effect of the equinus and not the combined effect of the orthosis, future users should compare the data to the OF condition.
This orthosis should help in the understanding of the biomechanical consequences of equinus gait and should help in decision making for the management of pathological gait in children.
Key Points
The study describes a new, adjustable, well-tolerated orthosis used to impose specific degrees of equinus in children.
A mean maximum equinus of −21.65° was induced at initial contact and −11.61° during stance.
The orthosis provides a new way to simulate equinus and its biomechanical consequences on gait.
Footnotes
Acknowledgements
This work was supported by Beaufour Ipsen Laboratories. We would like to thank Ouest Orthopedie company for their help and advice in the conception of the orthosis. We also thank Johanna Robertson for correcting the English of this paper. The authors express their gratitude to the volunteers who participated in this study.
Conflict of interest
The authors listed on the manuscript had no conflict of interest and there was no financial relationship between the authors and the sponsoring organisation during the study or preparation of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors