
Abstract
Background: In 2003, the British Society of Rehabilitation Medicine (BSRM) published guidelines on amputee and prosthetic rehabilitation, including those with congenital limb deficiency.
Objectives: The aim of the study was to evaluate the service provided by the Regional Disablement Service (RDS) to children with congenital upper limb deficiency, against BSRM guidelines.
Study Design: Retrospective chart review.
Methods: Chart review.
Results: Analysis of the group (n = 44) showed 52% were male, with 61% of children affected on the left side, and 73% having a transverse deficiency. Compliance to individual aspects of the guidelines varied considerably. Only 14 (32%) of children had met with the multidisciplinary team by the recommended age of six months. Analysis of referral sources and timings suggested that children were initially seen elsewhere and later referred to RDS after consultation with a surgeon.
Conclusions: RDS compliance with the BSRM guidelines was variable. Particularly disappointing was the low rate of children and families meeting the multidisciplinary team at an early age (< 6 months). The low rate of early referral prompted us to contact all paediatricians in Northern Ireland highlighting the guidelines, the benefits of early contact with RDS and encouraging referral on diagnosis.
This work will be of interest particularly to those involved in treating paediatric amputees. The challenges we face in treating upper limb deficient children in accordance with current guidance may not be unique and our study may prompt other units to consider how best to improve service to this group.
Introduction
The majority of individuals seen at prosthetic and amputee rehabilitation centres (PARCs) have had an amputation as a result of vascular disease or trauma, 1 but a smaller, equally important group of patients have congenital deficiency of one or more limbs. 2 The family of a child born with limb deficiency, and the child themselves, will have differing needs to the acquired amputee. 3 The involvement of a skilled and experienced multidisciplinary team at an early stage offers parents reassurance and advice at a time when they are likely to have many questions, and allows the most appropriate treatment plan to be made for their child.4,5 The physical limitations of a child with a lower limb deficiency will relate to mobility, while a child with an isolated upper limb deficiency is likely to have no mobility restriction but potentially significant functional difficulties. Both groups may face bullying from their peers, and there may be other associated congenital abnormalities which can impact on both the child’s functioning and their parents’ adjustment to a child with limb deficiency. 6
While recognizing there is a wealth of clinical experience in managing children with congenital limb deficiency, the development of guidelines in recent years has helped standardize care within this specialist field. The working party of the Amputee Medical Rehabilitation Society (AMRS) published a report in 1997, stating recommended standards of care specifically relating to congenital limb deficiency. 7 The particular challenges faced by this group were discussed, and the various treatment options for different types and levels of deficiency outlined. The guidelines on both upper and lower limb congenital deficiencies were subsequently updated and incorporated within Amputee and prosthetic rehabilitation – standards and guidelines, published by the British Society of Rehabilitation Medicine (BSRM) in 2003. 8
With regard to upper limb deficiency in particular, the 2003 guidelines recommend that:
children with congenital upper limb deficiency be referred to, and seen by, a consultant in rehabilitation medicine as soon as possible, ideally within one month of birth, and certainly by the age of six months;
where diagnosis has been made antenatally, the parents should be referred to the service as soon as the deficiency is recognized;
early specialist occupational therapist (OT) input is obtained;
the opportunity of availing of skilled counselling and support services such as clinical psychology should be offered;
as parents may have concerns regarding future pregnancies, the opportunity to meet with a geneticist should be offered;
the role of voluntary organizations, such as REACH, in supporting children with upper limb deficiency and their families is promoted, and should be highlighted to parents.
Our centre, the Regional Disablement Service (RDS), provides a service to the population of Northern Ireland (approximately 1.8 million according to the Northern Ireland Statistics and Research Agency). This is comparable to other PARCs in the UK. The multidisciplinary team at RDS includes medical and prosthetic staff, as well as physiotherapists and a specialist OT. There has been input on an individual basis for children and families who required clinical psychology.
This study was carried out to evaluate the service provided by RDS to those with congenital upper limb deficiency against the standards set in the 2003 BSRM guidelines. The work was undertaken as part of the unit’s commitment to audit and quality service provision. Should any variance be identified, an opportunity would exist to determine and address the reasons for this, improving the service provided to this group of patients.
Methods
From the RDS database (CIMS), all children under the age of 18 with upper limb deficiency of any kind were identified and their medical charts retrieved. The data were collected in 2008 and the charts reviewed related to children born between 1990 and 2008. Those children who had an acquired deficiency were not included in the study. While some of the study sample were born prior to the publication of the 2003 and 1997 guidelines, all children with congenital upper limb deficiencies and aged under 18 years were still included. As the guidelines were developed from published evidence and highly experienced clinicians, it was felt that many of the components in the guidelines should already have been part of our practice prior to their publication.
Demographic data were collected from the chart on gender, site and type of deficiency, according to the ISO/ISPO Classification of congenital limb deficiency. 9 Data were also obtained regarding the source of referral to RDS, the age at which this occurred and the time from referral to the first appointment. Pearson Chi squared test was undertaken on demographic and referral data to determine any statistically significant difference.
It was recorded whether, and at what point, a specialist OT was involved. Specifically where this occurred at the first attendance this was noted, and for the purpose of this study we chose ‘early’ OT involvement to be within three months of initial consultation. This was on the basis that if a child is referred promptly to RDS then a further three months will allow an OT to see them around the time that they begin reaching, grasping and performing bimanual activities. 10 Documentation of the family’s first visit was reviewed specifically with regard to discussion of genetics, clinical psychology and voluntary organizations.
The study was undertaken in accordance with trust audit protocols and ethical approval was not sought.
Results
In total, 51 children were identified from the database search. Two charts were unavailable while one child had just been referred and had not yet attended the centre – these three were therefore excluded. Four children had acquired deficiency and were also excluded. A further child had undergone amputation for an ischaemic forearm at birth; for the purpose of this audit this was considered as a congenital deficiency and included in the analysis. In total, 44 children were included.
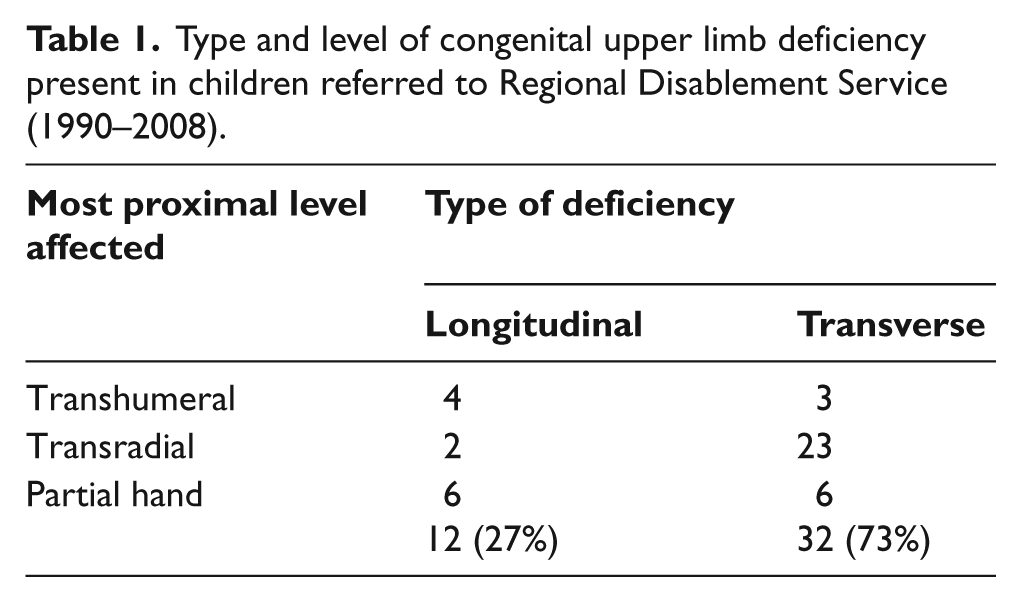
Analysis of the demographics showed that 21 (48%) were female, 23 (52%) male, with between one and five children being referred with an upper limb deficiency each year. Left upper limbs were affected in 27 children (61%), right in 14 (32%), and three children (7%) had bilateral deficiencies. Table 1 details the profiles of the deficiencies seen. Transradial deficiency was significantly more common in those with transverse deficiency (Pearson Chi squared; p = 0.004).
Type and level of congenital upper limb deficiency present in children referred to Regional Disablement Service (1990–2008).
With regard to standards 1a and 1b, two children (4.5%) were referred within their first month, and a total of 21 (47%) by age six months (Figure 1; there was no significant difference between referral ages of children with longitudinal and transverse deficiency (p = 0.111)). Of the eight children referred beyond their fifth birthday, three had just moved to Northern Ireland and had previously been treated in another PARC, the other five were referred for consideration of a prosthesis to aid purely in cosmetic appearance.
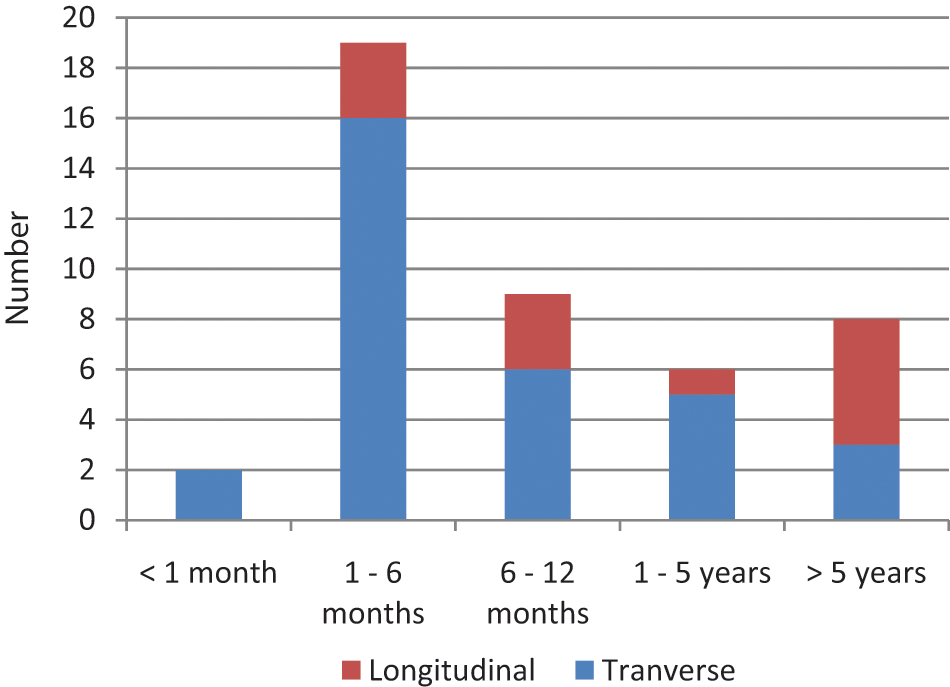
Number of children with congenital upper limb deficiency referred to Regional Disablement Service (1990–2008) by type of deficiency and age at referral.
Review of the timeframes between referral to the centre and attendance for first appointment showed that 42 children (95%) were seen by the multidisciplinary team within three months of referral having been received (Figure 2). It was not possible to determine a reason for two children waiting more than three months for their first appointment (one was seen 13 weeks from referral, the other 18 weeks). None of the children in the study were seen at the centre within their first month of life, and only 14 (32%) were seen for their first appointment before the age of six months.
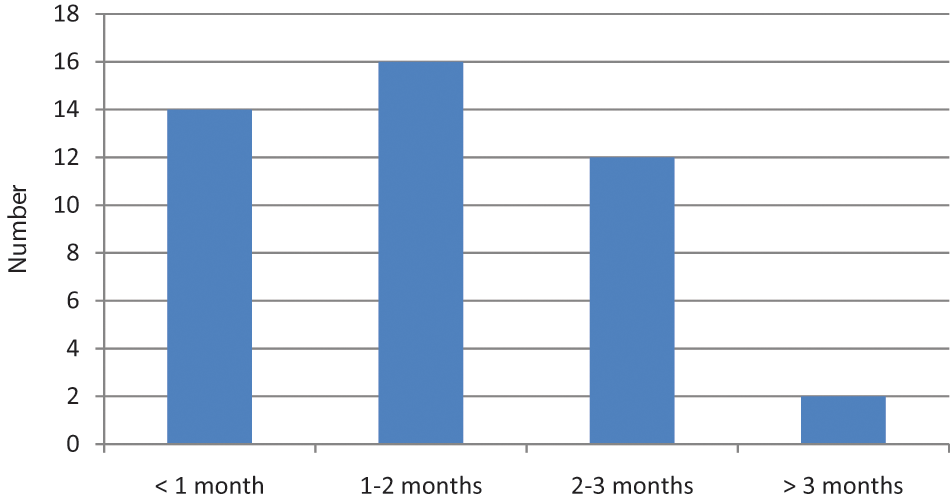
Time between referral of a child with congenital upper limb deficiency and first appointment at Regional Disablement Service (1990–2008).
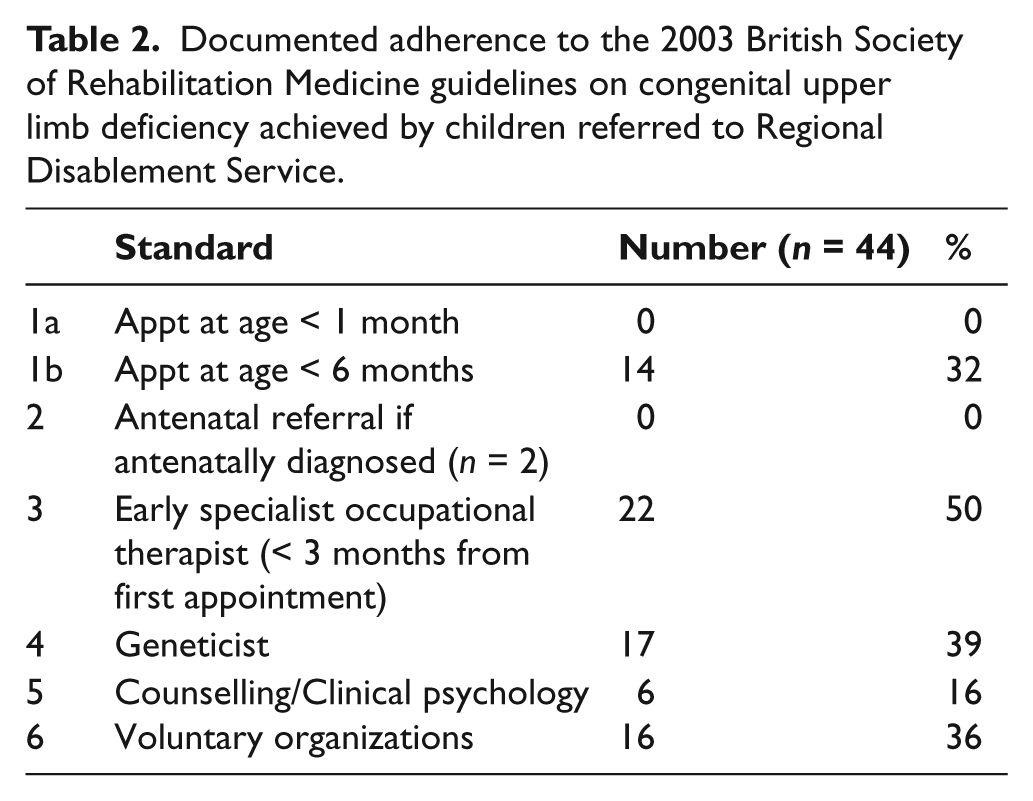
In two children (4.5%) an antenatal diagnosis had been made, but in neither case was a referral received prior to the birth of the child (Table 2). One was subsequently referred by their general practitioner (GP) at age four months, the other by an orthopaedic surgeon at seven months.
Documented adherence to the 2003 British Society of Rehabilitation Medicine guidelines on congenital upper limb deficiency achieved by children referred to Regional Disablement Service.
RDS receives referrals for paediatric patients from a number of different sources, including orthopaedics, plastic surgery, paediatricians and GPs (Figure 3). Of 16 referrals received from orthopaedic surgeons, only 44% were made while the child was less than six months old. There was no significant difference between the source of referral and its promptness (p = 0.341).
A specialist OT was involved at some point with 40 children (91%), and in 22 (50%) this occurred at an ‘early’ stage (either at the initial consultation or within the following three months). Of the children who did not see an OT (n = 4), one child’s family declined OT input, and three were referred as older children requesting an artificial limb for cosmetic reasons only.
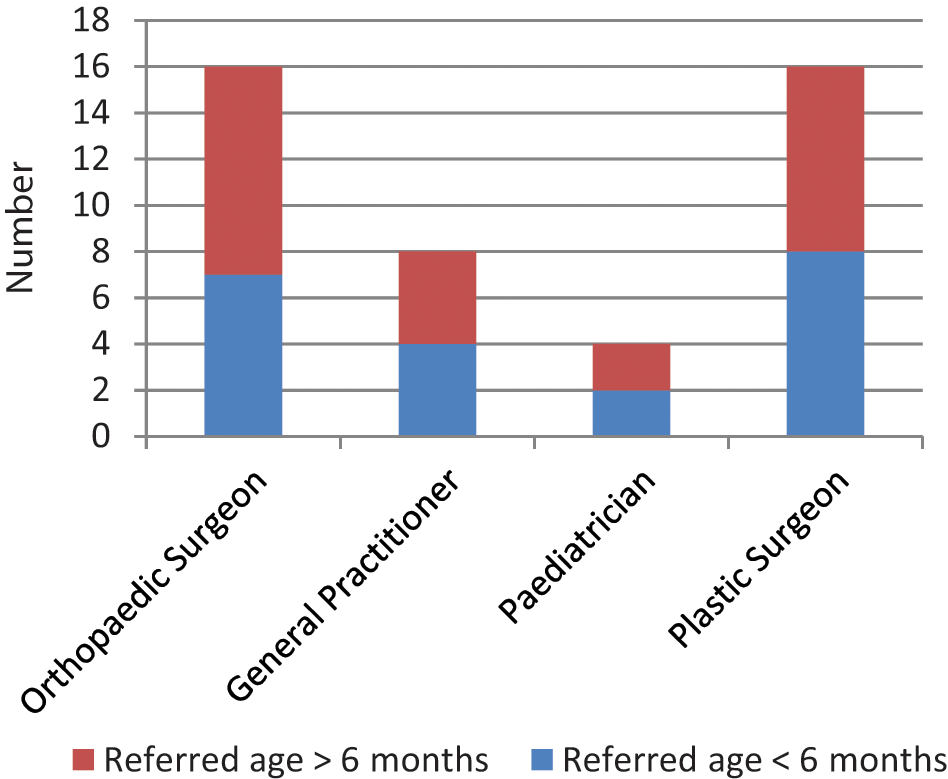
Source of referrals of children with congenital upper limb deficiency to Regional Disablement Service (1990–2008).
Skilled counselling and/or clinical psychology input was mentioned in six (16%) charts, and 17 (39%) families were documented as being offered, or having attended, an appointment with a geneticist. In five of those who had been seen by a geneticist, there were other confirmed congenital abnormalities.
The role of voluntary organisations was documented as having been discussed in 16 (36%) of the initial consultations at RDS.
Discussion
The demographic profile of our patient group is similar to that of other studies.2,11,12 We found an almost equal male:female occurrence of 1.1:1. Left:right ratio was 1.9:1, and three children (7%) were affected bilaterally. Transverse transradial deficiency of a single limb was the most common upper limb abnormality, as in other published work.11,12
Our study focused on children referred to RDS, but it is likely that there are children with upper limb deficiency in Northern Ireland of whom RDS has no record. There is a recognized association between longitudinal limb deficiency and associated abnormalities and syndromes such as congenital cardiac problems. 13 Where associated problems exist they may take precedence over limb considerations, and referral to RDS might not be considered. Longitudinal upper limb deficiency may be amenable to surgical procedures giving an acceptable level of function and if child and family have no concerns with cosmetic appearance again they may not be referred. It is also possible that children with either type of deficiency may have moved into our catchment area without requiring any input from the service.
This study of our service to children with limb deficiency in relation to BSRM guidance has highlighted definite areas for improvement. Compliance rates with standards regarding early referral of patients, speed of appointment times on referral receipt, and our documentation of involvement of other specialists such as geneticists and psychologists were disappointing.
Of particular concern in our study was the low rate of achieving first RDS attendance by the age of six months (n = 14, 32%). By the age of six months, a child may already have achieved sitting balance, begun bimanual activities and been rolling or even crawling. 10 At this point, and even earlier, there is potential benefit in fitting a child with a passive limb,14-16 so it is important that parents have met with the multidisciplinary team prior to this in order to discuss the options. We undertook a closer examination of each referral to determine the reasons for difficulty in achieving early appointments. Review of referral ages and appointment times showed that where a referral is received, most children (95%) can be seen within three months. This suggests that the service has capacity to see children within the recommended timeframe, allowing parents to meet with a skilled multidisciplinary team in a position to address many of their queries and concerns. It was not apparent from review of the charts why not all children were seen promptly on referral. One possible factor is that such appointments are generally arranged via telephone and every effort is made to accommodate parents in arranging a convenient time. Both parents (and even grandparents) are likely to wish to attend, and there may be work implications and childcare for siblings to consider. It is also possible that some families did not feel ready to meet the team, preferring to spend time with their newborn before approaching the next stage.
Given that only 21 children (47%) were referred to us within their first six months, even a rapid response from our service will result in non-compliance with the recommended standard. In order to improve the service and the experience of children and families, we felt that raising the profile of our centre among our colleagues in related branches of practice would be the most appropriate way forward.
Limb anomalies are recognized at birth, and a referral is generally made to an appropriate surgical team. However, congenital limb deficiency can be associated with other health problems, such as congenital cardiac abnormalities, and these critical issues may take precedence for a time. The majority of children are then referred on to our centre by the surgeon once they have attended the surgical clinic.
Strong links exist between the consultants in rehabilitation medicine and local plastic and orthopaedic surgeons, and a Combined Congenital Upper Limb Clinic involving all three specialties occurs three times a year. A number of children were first highlighted to us at this particular clinic. With the delay in specialist rehabilitation team input there may be a negative impact on the child and family. The parents may feel unable to gain a full picture of what will be possible for their child in the future, may be distressed by the number of professionals they meet, and are less likely to have the opportunity of an early meeting with another family in a similar situation without having met the rehabilitation team. Where there is a significant delay the child may not benefit from early use of a prosthesis to encourage them in bimanual activities, and in adjusting to the sensation of a prosthesis if it is appropriate.
Our results highlighted an opportunity to improve our service, and raising our profile among our colleagues in paediatrics appeared the most appropriate way of being referred such children at an earlier stage. Accordingly all hospital-based consultant paediatricians in the region were identified and written to by the consultants in rehabilitation medicine, with an explanation of our role and the benefits to child and family of early referral. The BSRM guidelines and our audit findings were highlighted, and referral to RDS at the same time as to the surgical team(s) was requested. While we as rehabilitation specialists see such children regularly, for our colleagues in other branches of medicine it is much less common. Having a clear indication of where the appropriate service is to be found and how to access it is likely to be regarded in a positive light, particularly if it is something a practitioner has not encountered before, and patients can be seen in a timely manner. As we suspect that the practice in our unit is similar to that elsewhere, obtaining referrals of children promptly may be a challenge others also face. A further study after several years would allow time for enough new referrals to be meaningfully analysed, and determine the effect of our actions.
The value of OT input in children with upper limb deficiency is well recognized.4,5,8 Regular contact with an experienced professional providing practical advice and training enables children and their families to maximize their function regardless of whether a prosthesis is used. Only 22 children (50%) met with our specialist OT within three months of their first appointment, from a total of 91% who had OT input at some point during their management. An improvement in this could be achieved by better communication between disciplines when scheduling a first appointment.
Parents of children with limb deficiency may have questions about why this has happened to their family, whether they are in some way to blame, and if there is a risk of a similar issue with further children.3,4,6,8 The chance to meet with a clinical geneticist and discuss these issues may address a number of their concerns and assist them to address the situation positively, which in turn will benefit their child. It is understandable that some parents and families require more support in coming to terms with the situation, and may benefit from meeting with a skilled counsellor or psychologist. The support and reassurance provided by meeting and learning from the experiences of families in a similar position may also assist parents and siblings to come to terms with a limb deficiency.4,8,17 As the child themselves grow, the peer support provided through organisations such as REACH may prove invaluable. Unfortunately our study found disappointing figures for involvement of a geneticist (39%), clinical psychologist (16%) and discussion of voluntary organisations (36%).
There were a number of limitations to the study. Only charts held in our facility were reviewed. As there may be duplication with other specialties, particularly where a child has been seen by another team initially, it is possible that genetic counselling, support organisations and psychological support were discussed elsewhere and not recorded in our notes. It is also possible that non-uptake of offered services was not documented in every case.
Conclusion
The findings suggest variable compliance with BSRM guidelines on management of congenital upper limb deficiency in Northern Ireland. The poor rate of early appointments is in part due to a low rate of early referral. By highlighting the role of a prosthetic and rehabilitation centre to local paediatricians, as well as the current guidelines on management of children with limb deficiencies, we hope to ensure prompt referral on diagnosis of a limb deficient child to an experienced multidisciplinary rehabilitation team.
Footnotes
Acknowledgements
Ethical approval for this retrospective chart review was not sought. The work was carried out in accordance with local audit guidance, and the findings have been formally presented at the trust audit meeting.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors report no conflicts of interest.