
Abstract
Background: Electromyography (EMG) pattern recognition offers the potential for improved control of multifunction myoelectric prostheses. However, it is unclear whether this technology can be successfully used by congenital amputees.
Objective: The purpose of this investigation was to assess the ability of congenital transradial amputees to control a virtual multifunction prosthesis using EMG pattern recognition and compare their performance to that of acquired amputees from a previous study.
Study Design: Preliminary cross-sectional study.
Methods: Four congenital transradial amputees trained and tested a linear discriminant analysis (LDA) classifier with four wrist movements, five hand movements, and a no-movement class. Subjects then tested the classifier in real time using a virtual arm.
Results: Performance metrics for the residual limb were poorer than those with the intact limb (classification accuracy: 52.1%±15.0% vs. 93.2%±15.8%; motion-completion rate: 49.0%±23.0% vs. 84.0%±9.4%; motion-completion time: 2.05±0.75 s vs. 1.13±0.05 s, respectively). On average, performance with the residual limb by congenital amputees was reduced compared to that reported for acquired transradial amputees. However, one subject performed similarly to acquired amputees.
Conclusions: Pattern recognition control may be a viable option for some congenital amputees. Further study is warranted to determine success factors.
Clinical relevance
This research addresses a largely under-studied subject population. It suggests that some congenital amputees may be able to control multifunction prostheses with EMG pattern recognition, despite lacking a complete limb since birth.
Background
Approximately 0.8% of limb deficiencies in the USA are congenital, with an incidence of approximately 26 per 100,000 live births and over half affecting the upper limb. 1 Although congenital limb deficiency accounts for a small percentage of total limb loss in the USA, it is the predominant cause of limb loss in children (91%). 2 Congenital limb defects can stem from multiple causes, although a specific agent is rarely identified. In the 1950s and 1960s, 20% of newborns whose mothers took the sedative thalidomide had birth defects, the majority of which affected their limbs. 3 About 1.9 in 100,000 newborns experience limb malformations caused by amniotic band syndrome (ABS), a condition where fibrous bands wrap around a limb and restrict its growth. 4 Fetal genetic information extraction via chorionic villus sampling has also been associated with an increased risk of ABS and congenital abnormalities. 5 Although the population of congenital amputees in the USA is small, there is a need to provide them with improved prosthetic treatment; reported rates of prosthesis rejection by congenital amputees range from 34% (n=32) to 75% (n=20).6,7
Myoelectric prostheses are a common treatment for transradial amputees. These prostheses typically use the amplitudes of EMG signals from two different muscle sites to control a simple motorized hand. However, newer pattern recognition algorithms have been developed to extract more data from the EMG signals of multiple muscles, enabling intuitive control of multifunction wrists and hands. Studies with acquired amputees have demonstrated that muscles in the residual limb can be used for pattern recognition control of multifunction prostheses.8-13 A few studies have included congenital amputees in the study population14-17; however, no quantification of pattern recognition control by congenital amputees and comparison to acquired amputees is available in the literature. The results of a preliminary magnetic resonance imaging (MRI) study with four congenital amputees suggest that the residual forearm contains similar musculature to the intact forearm, although deficient limb muscles are less developed and covered with a greater volume of soft tissue. 17 It is unclear how these changes translate to the ability of congenital amputees to elicit patterns of muscle activity associated with different hand and wrist movements.
The purpose of this study was to quantify how well subjects with congenital limb deficiencies could control a virtual arm using EMG pattern recognition and to compare this performance to that of acquired transradial amputees measured in a previous study. 10 Due to the small size of the population of transradial congenital amputees, this initial study was limited to four subjects. The quantification of real-time control performance provides an assessment of the feasibility of myoelectric pattern recognition control of multifunction prostheses for subjects with congenital transradial limb deficiencies.
Methods
Subject information
Four subjects with unilateral congenital transradial amputations participated in the experiment (Table 1). Subjects provided informed consent and permission to publish photographs. The study protocol was approved by the Northwestern University Institutional Review Board.
Demographic data of the four congenital transradial subjects.
EMG data acquisition
Each subject was fit with 12 bipolar Ag/AgCl disposable electrodes with 2 cm centre-to-centre electrode distances (Noraxon USA, Inc.). During sessions with the residual limb, a ring of eight equally spaced electrodes was placed approximately 2–3 cm distal to the elbow crease. A ring of four equally spaced electrodes was placed on the distal limb (Figure 1). During sessions with the intact arm, a ring of six equally spaced electrodes was placed 2–3 cm distal to the elbow crease, and three equally spaced electrodes were placed 2–3 cm proximal to the wrist crease; the three remaining electrodes were placed on the hand over the thenar, hypothenar and first dorsal interosseous muscles. EMG signals were amplified, band-pass filtered (5–400 Hz), and sampled at 1 kHz. Custom software programmed in MATLAB (The MathWorks, Natick, MA) and a custom data acquisition system were used for data collection and subject prompting.

Electrode placement on one congenital amputee subject’s residual limb.
Experiment
Each subject participated in three sessions spaced one week apart. The residual limb was tested during the first (or practice) session and third session, and the intact limb was tested during the second session. The purpose of the practice session was to familiarize the subjects with the protocol. The second session was intended to determine how well subjects could perform with an optimal electrode configuration covering the majority of available wrist and hand muscles – including intrinsic hand muscles. The final session was intended to quantify the subjects’ ability to use pattern recognition for multifunction myoelectric prosthesis control with their residual limb. Each session consisted of three parts: (1) classifier training, (2) classifier testing (offline tests), and (3) control of a virtual arm (real-time tests).
For the classifier training trials, subjects were instructed to follow a series of randomly ordered visual prompts for 11 motion classes. The four wrist movements were forearm pronation, forearm supination, wrist flexion and wrist extension. The six hand motions were chuck grip, key grip, tool grip, power grip, fine pinch and hand open. The subjects also trained a no-movement class. Subjects used mirror movements of their intact limb to aid in attempting movements with their residual limb. Following each prompt, subjects attempted to perform and hold the movement for 4 s using a comfortable and consistent level of effort. EMG data for each movement were recorded twice in each of four trials, resulting in 32 s of data per movement. The rest times between movements in the four trials were 3 s, 2 s, 0 s and 1 s, respectively. The delay differences were intended to capture greater variability in EMG signals during movement initiation and therefore create a more robust classifier. EMG data for each individual movement were concatenated and segmented into a series of 150 ms windows with 50 ms of overlap. Four time-domain features (mean absolute value, number of zero crossings, waveform length and number of slope sign changes) were extracted from each window for each of the 12 channels. These feature sets were used to train a linear discriminant analysis (LDA) classifier, chosen for its computational efficiency and its comparative performance to more complex classification algorithms. 18
Each of the four training trials was followed by a testing trial. Testing trials were identical to training trials, except that all rest times between movements were 3 s. The additional 32 s of data per movement from the testing trials were concatenated and segmented in the same manner as the training data. The time-domain feature sets were extracted from the testing data and used to determine the classification accuracy: the percentage of correct classification decisions out of the total number of classifier decisions.
In real-time tests, subjects used the classifier built from the training data to perform the 10 wrist and hand movements with a virtual arm. The no-movement class was included in the classifier but not independently tested. The virtual arm responded to classifier decisions in real time, providing immediate visual feedback. Subjects were asked to move each degree of freedom through its full range of motion. For instance, to test wrist flexion, the virtual hand began in full wrist extension and the subject was prompted to fully flex the wrist. Subjects were given 5 s to perform each movement. EMG data were segmented into 150 ms windows with 50 ms of overlap, resulting in a new classification decision every 100 ms. A trial was considered successful if a total of 10 correct decisions (not necessarily consecutive) were made within the 5 s time limit. Each correct decision moved the virtual arm one step closer to the target posture; the arm reached the target posture after the tenth correct decision. Each classification resulting in movement in the opposite direction (for example, a wrist extension decision during wrist flexion) caused the number of correct movements to decrease by one. Other misclassifications did not affect the number of correct decisions. To make hand-grasp testing more functionally relevant, the first grip classification was applied to all subsequent grip classifications as the subject attempted to close the virtual hand. To select a new grip, subjects were required to fully open the virtual hand. Each of the 10 movements was performed three times per trial in six trials, resulting in 180 real-time tests for each session. Real-time tests were evaluated based on the percentage of successfully completed motions (motion-completion rate) and the time taken to complete a motion (motion-completion time) within a 5 s time limit. Motion-completion time was measured from the final no-movement decision prior to the initiation of motion and had a resolution of 100 ms. The median motion-completion times from each subject were determined, and these values were averaged across subjects for each session.
The abovementioned procedure replicated the study conducted by Li et al., in which patients with acquired amputations were tested. 10 This allowed for a comparison between the two subject groups.
Data analysis
Offline and real-time test results are reported for each individual subject and/or as overall averages ± standard deviations. Performance metrics were calculated for each individual motion, for hand motions combined, for wrist motions combined, and for all motions combined. Neither parametric nor non-parametric tests for statistical significance were possible given the small sample size.
Results
Offline classification accuracy
Classification accuracies for training and testing with the congenital residual limb increased by 12.6%±10.1% between the practice session and the final session (Figure 2a). The overall classification accuracy for the final session with the residual limb was 52.1%±15.0%; this was 41.1%±15.8% lower than that for the intact limb (Figure 2a). This was also lower than that of the residual limb of acquired amputees (79.1%±11.1%). 10 Classification accuracies achieved with the intact limb, however, were nearly equivalent between the two groups (93.2%±4.2% for congenital amputees and 93.7%±3.2% for acquired amputees). 10
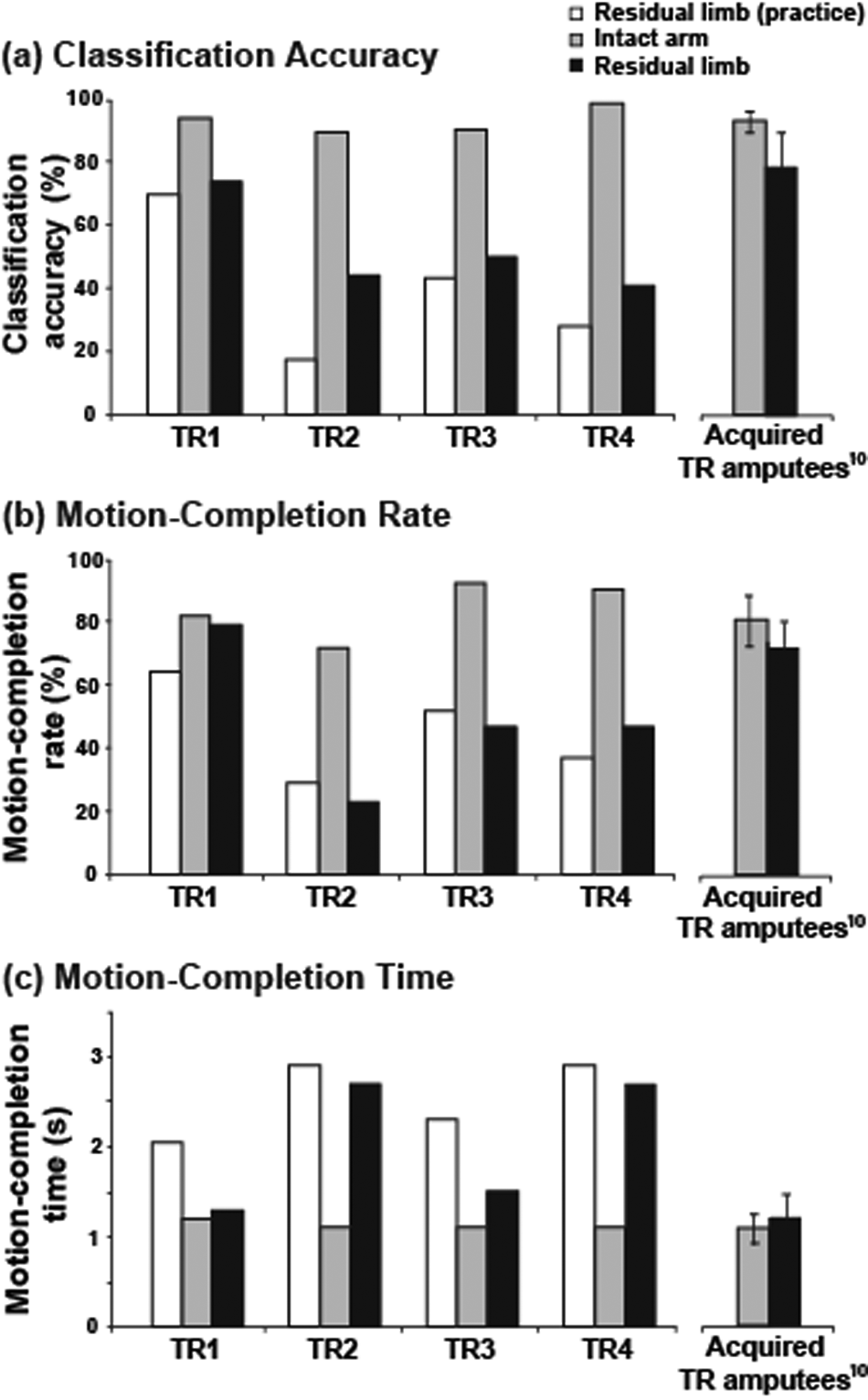
The ability of four congenital transradial amputees (TR1–4) to perform pattern recognition control of a virtual prosthetic arm with 10 motions and one rest class was measured using (a) overall offline pattern classification accuracies; (b) real-time motion-completion rates; and (c) real-time motion-completion times. The average values from five acquired transradial amputees reported in a prior study are presented for comparison. 10
For the residual limb of congenital amputees, wrist classes had an approximately 14% higher classification accuracy than hand classes (a difference of 14.3%±13.7% over the four subjects). Key grip, chuck grip and tool grip had the lowest overall classification accuracies (Table 2). However, the classification accuracy for power grip was greater than 50% for three subjects; the classification accuracy for hand open was greater than 50% for two subjects; and one subject achieved a classification accuracy of greater than 50% for three of the four grips (Table 2).
Offline classification accuracies for the residual limb of each congenital subject.
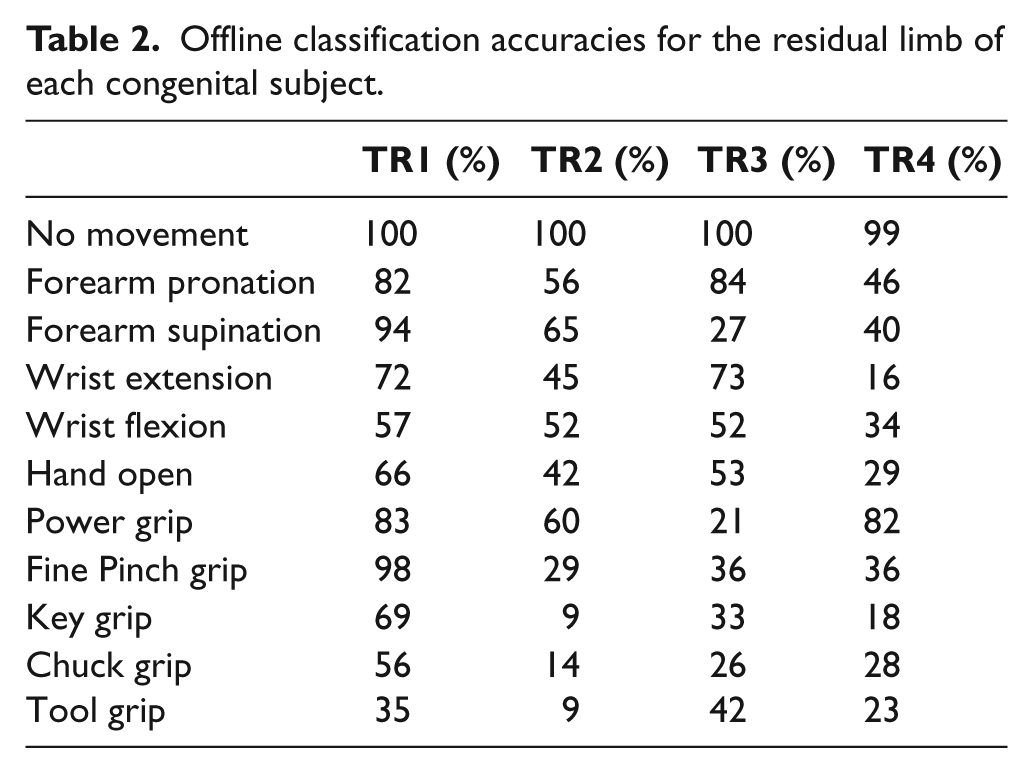
Classification accuracies increased when the number of classes was reduced to a clinically relevant configuration (wrist pronation/supination, wrist flexion/extension, hand open/power grip, no movement). For the subject with the highest overall classification accuracy for the 11-class classifier (TR1), the accuracy increased from 74%±20% to 87%±14%. For the subject with the lowest overall classification accuracy (TR4), the improvement was from 41%±26% to 53%±29%. For TR4, decreasing the classes further to include only wrist pronation/supination, hand open/close, and no movement increased the classification accuracy to 72%±20%.
Real-time virtual prosthesis control
Motion-completion rate
For three subjects, overall motion-completion rates with the residual limb were approximately 45% lower than those achieved with the intact arm (Figure 2b). For one subject (TR1), however, this difference was only 3.3%. Wrist motion-completion rates showed the largest degree of variation: the four subjects achieved motion-completion rates for wrist motions of 100%, 51.4%, 70.8% and 19.4%, respectively. For comparison, the average wrist motion-completion rate for the intact arm of each congenital subject was greater than 98%, and the average wrist motion-completion rate for the residual limb of each previously tested acquired amputee was greater than 97%. 10
The average motion-completion rate for combined hand movements (hand open and four grips) with the residual limb was 41.4%±17.6%. This was lower than the average achieved with the intact limb (73.6%±15.1%) but only slightly lower than that achieved by acquired amputees with the residual limb (53.9%±14.2%). Overall motion-completion rates with the intact limb were less variable among subjects and were roughly equivalent to those of acquired amputees (84.0%±9.3% and 81.2%±8.1%, respectively). 10
Motion-completion time
Overall motion-completion times decreased slightly for all four subjects between the practice and final session with the residual limb (Figure 2c). For one subject (TR1), the motion-completion times measured in the final session with the residual limb approached those achieved with the intact limb (Figure 2c). Average motion-completion times for all movements were 2.05±0.75 s for the residual limb and 1.13±0.05 s for the intact arm. Those for the congenital limb were slightly higher than those seen for acquired amputee subjects (1.24±0.27 s), while those for the intact limb were similar (1.14±0.17 s). Note that motion-completion times were only counted for movements completed in 5 s or less.
Discussion
The results of this study suggest that pattern recognition prosthesis control may be a viable and beneficial option for some congenital amputees. Although chance performance would result in an average classification accuracy of less than 10% for this 11-class paradigm, the overall offline classification accuracy for all four subjects was 52.1%±15.0%, with one subject achieving 73.9%. This same subject demonstrated a motion-completion rate of 100% for wrist movements and a motion-completion rate of 64.8% for hand movements, similar to acquired amputees.
The performance of these participants varied widely and was, on average, poorer than that of acquired amputees. This was not due to a reduced innate ability to perform the task, as both groups demonstrated similar performance with their intact arms. Instead, it was largely due to decreased wrist movement control. Whereas wrist motion-completion rates for the amputated limb of acquired amputees was close to 100% for each participant, wrist motion-completion rates in this study ranged from 19.4% to 100%. Hand motion-completion rates, by comparison, were only slightly reduced from those of acquired amputees. Acquired amputees consistently did better with wrist control than hand control. This is presumably due to the presence of the wrist muscles in the remaining forearm and absence of the intrinsic hand muscles. Congenital amputees had more variability in what they could control. Some of the congenital amputees may have had some intrinsic hand muscles in their residual limbs. This may have contributed to the relatively higher accuracy rates for some hand closing patterns in two of the congenital amputees. Wrist control was not consistently stronger in the congenital amputees, possibly due to deficits of wrist muscles in the limb or deficits in the motor pathways. The electrode configuration was the same for the residual limbs of both groups of subjects.
To successfully select candidates with congenital amputations for pattern recognition myoelectric control, it will be important to determine the factors that contribute to success. The exemplary performance of subject TR1 could be attributed to his age – he was the youngest subject – and/or to the fact that he was the only subject who regularly used a myoelectric prosthesis. Age of first use has been indicated as an important factor in the acceptance of myoelectric prostheses by congenital amputees, 19 and may contribute to the success of pattern recognition control. The length of T1’s residual limb may also have contributed to his success: subject TR3, with a similarly long residual limb, demonstrated the second highest classification accuracies and motion completion rates. However, it is very difficult to ascertain the ideal characteristics given the small sample size. Each of these factors should be investigated further to determine optimal conditions for candidacy. Additional factors to consider include muscle volume and the depth of the overlying fatty tissue. 17
The performance of these four subjects is promising for the use of simpler classifiers with more training. This protocol was challenging for these subjects, as they were new to pattern recognition control and were given limited training time with a complex classifier. However, three subjects had a motion-completion rate greater than 75% for at least one grip, and one subject (TR1) had a motion-completion rate greater than 80% for two grips. In addition, three of the four subjects had greater than 90% motion-completion rates for hand open. Classification accuracies increased for all four subjects when the number of classes was reduced. It is worth noting that for the subject with the worst classification accuracy (TR4), the number of classes had to be reduced to five (hand open/close, wrist pronation/supination and no movement) in order to achieve overall classification accuracies similar to that of subject TR1 with the 11-class system. Therefore, the applicability of pattern recognition control was highly subject-specific. Although we only saw a small improvement between the practice session and the final session with the residual limb, it is possible that subject performance could improve with more training.
This study encourages a closer look at the neuromuscular systems of congenital amputees. The ability of one subject to produce distinguishable muscle activity for two different hand-grasp patterns may support the theory that a cortical representation of the missing hand persists in congenital amputees. Studies comparing left and right hemispheres of unilateral congenital amputees have shown that cortical organization is largely unchanged, whereas a greater difference in cortical organization between hemispheres has been found in traumatic amputees. 20 Functional magnetic resonance imaging studies with unilateral congenital amputees have shown similar cortical activation patterns in the motor cortices on both sides.21,22 However, phantom limb sensation, which involves a neural representation of the limb, is more common with acquired amputees (present in 75% or more cases)23,24 than with congenital amputees (~20% of cases). 25 Even so, many believe that this representation develops regardless of the development of the physical limb. 26 It is also possible that the congenital amputees in this study were able to produce distinguishable muscle patterns for different movements even without well-developed cortical representations.
Conclusions
Pattern recognition control of myoelectric prostheses may prove to be a viable treatment option for many congenital amputees. Further study is warranted, with particular attention paid to factors that affect the ability of congenital amputees to successfully use this technology. Studies involving simpler systems and longer training sessions are also recommended for further analysis of this application.
Footnotes
Acknowledgements
The authors thank Guanglin Li for help in developing the protocol and Levi Hargrove and Blair Lock for reviewing the manuscript.
Funding
This work was supported by the National Institute of Child Health and Human Development, R01-HD-05-8000.
Conflict of interest
The authors report no conflicts of interest.