
Abstract
Background: The prosthetic rejection rates in children with an upper limb transversal reduction deficiency are considerable. It is unclear whether the timing of the first prescription of the prosthesis contributes to the rejection rates.
Objective: To reveal whether scientific evidence is available in literature to confirm the hypothesis that the first prosthesis of children with an upper limb deficiency should be prescribed before two years of age. We expect lower rejection rates and better functional outcomes in children fitted at young age.
Methods: A computerized search was performed in several databases (Medline, Embase, Cinahl, Amed, Psycinfo, PiCarta and the Cochrane database). A combination of the following keywords and their synonyms was used: “prostheses, upper limb, upper extremity, arm and congenital”. Furthermore, references of conference reports, references of most relevant studies, citations of most relevant studies and related articles were checked for relevancy.
Results: The search yielded 285 publications, of which four studies met the selection criteria. The methodological quality of the studies was low. All studies showed a trend of lower rejection rates in children who were provided with their first prosthesis at less than two years of age. The pooled odds ratio of two studies showed a higher rejection rate in children who were fitted over two years of age (pooled OR = 3.6, 95% CI 1.6 – 8.0). No scientific evidence was found concerning the relation between the age at which a prosthesis was prescribed for the first time and functional outcomes.
Conclusion: In literature only little evidence was found for a relationship between the fitting of a first prosthesis in children with a congenital upper limb deficiency and rejection rates or functional outcomes. As such, clinical practice of the introduction of a prosthesis is guided by clinical experience rather than by evidence-based medicine.
Introduction
About 16 out of 10,000 children are born with congenital anomalies of the upper limb (Kuyper et al. 2001). They may present as part of a syndrome or as isolated defects. The precise cause of many of these defects is unknown; they are most likely due to complex interactions between genetic and intrinsic factors. In the Netherlands, about 70 children with congenital defects of the upper limbs are born each year (Kuyper et al. 2001).
Children with a transverse failure of formation of the upper limb may be provided with a prosthesis. Most prostheses are prescribed to children with congenital upper limb defects at one-thirds and two-thirds of the forearm. Functional benefits may be expected from regained bimanual activities and body symmetry (Kuyper et al. 2001). However, it is known that there is a considerable rejection rate in patients with congenital anomalies. Several reasons for rejecting the prosthesis are revealed in literature. Considering the amputation level, the rejection rate in patients with an amputation through the upper arm or the hand is high. Handling an upper arm prosthesis is a demanding job. On the other hand, longer stumps are more useful as sensory tools. Children with a distal amputation will automatically develop compensatory skills for the necessary bimanual activities (Kuyper et al. 2001; Scotland and Galway 1983).
Patients also resist wearing the prosthesis in certain phases of their life. Young children perform mainly motor skills for which a helping hand can be useful. As children grow older, activities change towards more intellectual tasks and as such, the need for a prosthesis diminishes (Postema et al. 1999). Additionally, during puberty many patients deal with psychological problems regarding their deficiency.
Finally, the lack of functional benefits due to the technical limitations of the prothesis (weight, vulnerability of the electrical system, velocity, lack of sensory feed-back) is an important factor in rejecting the prosthesis. (Glynn et al. 1986; Scotland and Galway 1983; Kuyper et al. 2001).
Besides these explanations the age of the first fitting of a prosthesis is regarded to be an important factor in the acceptance of the prosthesis (Postema et al. 1999; Kuyper et al. 2001). Whether or not a child gets the opportunity to develop a wide variety of motor programmes in the sensorimotor cortices of the brain during the first years of life could be one of the explanations of this association (Hadders-Algra 2000; Shaperman et al. 2003). If a child learns to handle the prosthesis at young age, the prosthesis might be better incorporated into the body scheme and into the motor control of the child. As a result, one might expect that the usage of the prosthesis in children who were fitted at very young age is more favourable than in children who were fitted at later age.
In guidelines for prosthetic fitting of children with a congenital upper limb deficiency in different centres worldwide, the recommended age of the first fitting ranges from two months to 25 months (Postema et al. 1999; Kuyper et al. 2001). Fitting after this age seems to be related with higher rejection rates (Postema et al. 1999; Scotland and Galway 1983; Murray et al. 1972). However, how strong the scientific evidence of this data in literature is, has not yet been investigated.
The aim of this study is to reveal, by means of a systematic review, whether prescription of the first prosthesis at young age (<2 years of age) is related to lower rejection rates and better functional outcomes at later age (>2 years of age) in children with congenital unilateral upper limb deficiency.
Methods
Literature search
We identified relevant publications by means of computerized searches and citation tracking for the period 1966 – 2004. The search was carried out as a double retrieval (CS and MM). The search strategy included Medline (Pubmed 1966 – 2004 and Winspirs 1966 – 2004), Embase (Winspirs 1989 – 2004), Cinahl (Winspirs 1982 – 2004), Amed (Winspirs 1985 – 2004), Psycinfo (Ebsco 1966 – 2004), the Cochrane Library and online content/PiCarta. A combination of the following keywords and their synonyms was used: ‘prostheses’, ‘upper limb’, ‘upper extremity’, ‘arm’ and ‘congenital’ (Table I). Furthermore, references of conference reports, references of most relevant studies, citations of most relevant studies (Web of Science) and related articles were checked for relevancy. Functionality and satisfaction were not included in the final search while these terms did not provide any useful hits.
Strategy used for computerized searches.
Selection criteria
Studies were selected if they met the entry criteria (Table II). The assessment of the potentially eligible studies for meeting the entry criteria was done independently by two of the authors (CM and MM). In cases of disagreement consensus was sought with one of the other authors (CS). Interrater agreement was expressed using Cohen's Kappa.
Inclusion criteria for studies.
Assessment of methodological quality
All retrieved studies were scored on methodological quality. Two authors independently assessed the publications (CM and MM) with the Cochrane checklist for cohort studies (The detailed checklist used, is available from the authors). Thirteen criteria were used to evaluate the validity, clinical relevance and usefulness in the Dutch health system (Table III). Each criterion was scored ‘yes’, ‘no’ or ‘insufficient information’. Disagreements with respect to methodological quality were identified and resolved in a consensus discussion. If consensus could not be reached, a third reviewer (CL) made the final decision. The final quality score for each study was based on full consensus between the reviewers.
Criteria to assess the studies for quality.
Data extraction and data analysis
Where applicable, quantitave data, like odds ratios and proportions, were extracted. A (pooled) odds ratio was calculated based on available data.
Results
Selection of literature
The systematic literature search yielded 285 publications. Assessment of these potentially eligible studies for meeting the entry criteria reduced the number of studies to three with a moderate interrater agreement Cohen's Kappa (k) of 0.59. Hand search made the ultimate number of included studies to four.
Methodological quality
Table IV shows a detailed description of the included studies. The agreement of the methodological quality assessment of the two authors (CM and MM) was high and after discussion and consulting the independent reviewer (CL) full consensus was reached. All studies were retrospective cohort studies, level 3 (Wright et al. 2003). The characteristics of the study population and inclusion criteria have been clearly described (Brooks and Shaperman 1965; Lamb et al. 1971; Postema et al. 1999; Scotland and Galway 1983). A wide range in follow-up time was revealed (Brooks and Shaperman 1965; Postema et al. 1999) and selective loss-to-follow-up could not be judged (Brooks and Shaperman 1965; Lamb et al. 1971; Scotland and Galway 1983). Confounders like amputation level and time to follow-up were not analysed in relation to the age the first prostheses were described (Brooks and Shaperman 1965; Lamb et al. 1971; Postema et al. 1999; Scotland and Galway 1983). The all-over validity of the four selected manuscripts was doubtful.
Characteristics of included studies.
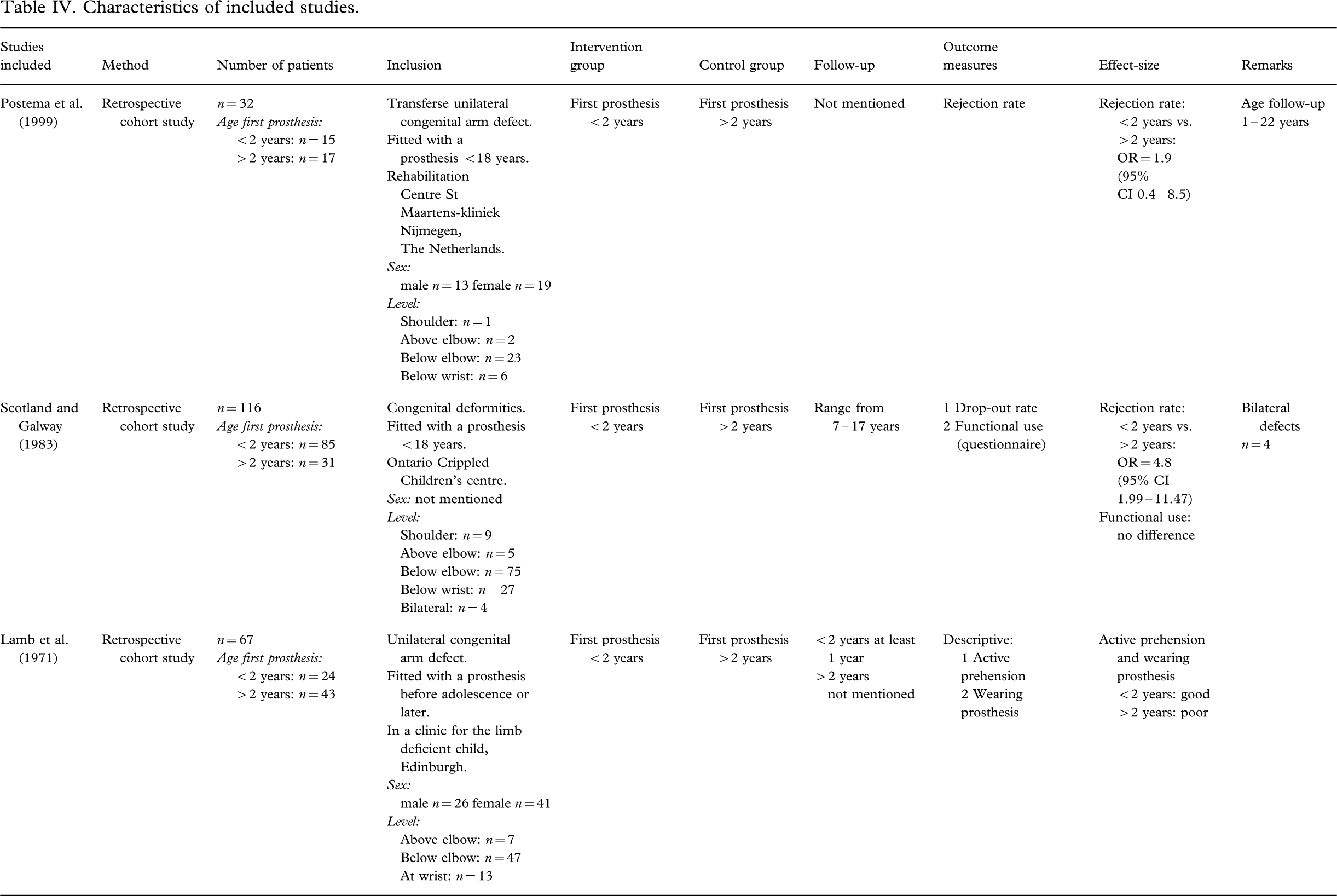
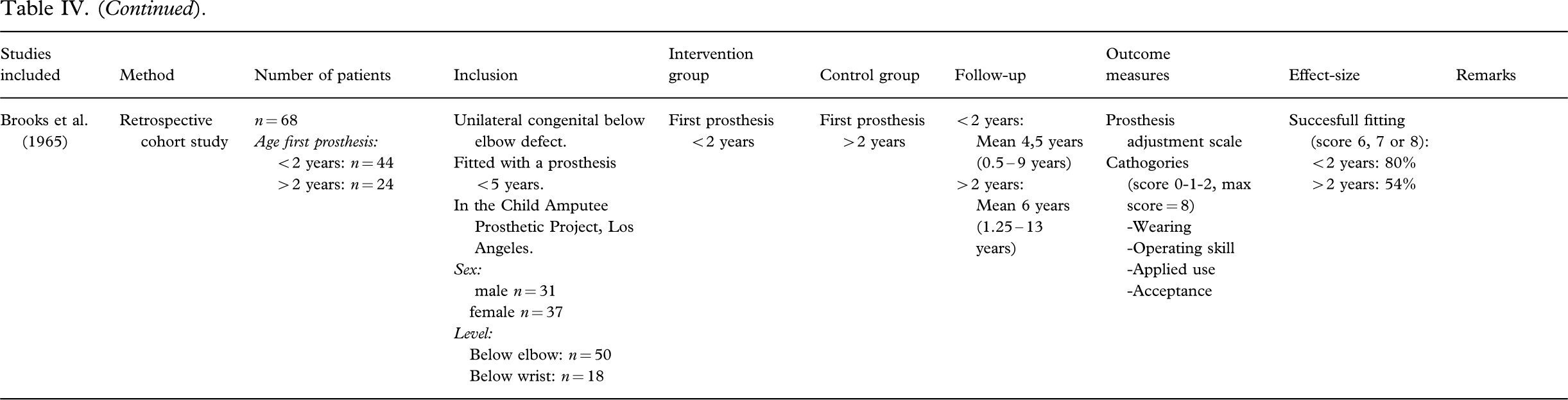
Results were measured in odds ratios (Postema et al. 1999; Scotland and Galway 1983), proportions (scored on a self-made scale) (Brooks and Shaperman 1965) or were only descriptive (Lamb et al. 1971) (see Table IV).
Data extraction and data analysis
Rejection rate
The relation between the age the first prosthesis was prescribed (<2 years vs. >2 years) and the rejection rate at later age was expressed in odds ratios (OR) by Postema et al. (1999) (OR 1.9, 95% CI 0.4 – 8.5) and Scotland and Galway (1983) (OR 4.8, 95% CI estimated by the authors: 2.0 – 11.5). The estimated pooled odds ratio of these two studies was calculated: OR = 3.6, 95% CI 1.6 – 8.0.
This calculation implies that the chance that children who receive the first prosthesis after the age of two years reject their prosthesis is 3.6 times higher in comparison with children who were provided with their first prosthesis before two years of age. The remaining two studies (Brooks and Shaperman 1965; Lamb et al. 1971) also described a lower rejection rate in children fitted less than two years of age.
Functional outcomes
In the study of Scotland and Galway (1983) a questionnaire was used to measure patterns of functional use (without direct observation). These authors found no differences in functional use of the prosthesis between children fitted before the age of two years and children fitted after two years of age. Lamb et al. (1971) analysed ‘active prehension’ and ‘wearing the prosthesis’. Both variables were ‘good’ for those fitted less than two years of age and ‘poor’ for those fitted over the age of two years. Brooks and Shaperman (1965) used the ‘prosthesis adjustment scale’. This scale was developed by the authors to measure ‘wearing’, ‘operating skill’, ‘applied use’ and ‘acceptance of the prosthesis’. The outcome was 80% successful fitting for those fitted under two years of age and 54% for those fitted over the age of two years.
Rejection rate and functional outcomes
No data have been found regarding the relation between the age of prescription of the first prosthesis for children with congenital unilateral upper limb deficiency and functionality or satisfaction as reason for rejection at a later age.
Discussion
Only four studies met the inclusion criteria of the study. Unfortunately, the methodological quality of all studies appeared to be doubtful. Although we performed this systematic review most accurately, the limited number and the low quality of the studies is a limitation of our study. Therefore, the results should be interpreted with caution. The most important result of our review is that all studies show a trend of lower rejection rates in children who were provided with their first prosthesis at less than two years of age. Furthermore, functional outcomes seem to be more favourable in those children fitted before two years of age. However, these conclusions should be seen as trends, rather than as evidence.
Our results lead to the question whether early exposure of the brain to the presence of a prosthesis can explain the differences in outcomes between children who were provided with a prosthesis before two years of age compared to those who were fitted at later age. The hypothesis that ‘earlier might be better’ is in line with the Neuronal Group Selection Theory (NGST) developed by Edelman in 1989 (Sporns and Edelman 1993; Hadders-Algra 2000). According to the NGST the brain is dynamically organized into neuronal networks or neuronal groups. The structure and the function of these networks are influenced by development and behaviour of the child. The NGST argues that motor development is characterized by two phases of variation: Primary and secondary variability. During the primary variability phase, motor activity is variable and not strictly tuned to environmental conditions. In the secondary variability phase, the child learns to select on the basis of active practice from the variable movement repertoire the most efficient motor strategy in each specific situation. The duration of the transition from the phase of primary to secondary variability depends on the motor function the child performs. For example, the transition of primary to secondary variability in reaching movements takes place during the second half of the first year. It takes until adolescence before secondary variability of all motor functions obtains its adult configuration.
In the child with a unilateral congenitaI limb deficiency the brain will not develop neuronal groups devoted to lower arm control. According to the NGST concept, providing an upper limb prosthesis during early phases of development (during the phase of primary variability) might induce neuronal groups devoted to the impaired limb, i.e., a representation of the limb with prosthesis in the brain. In addition, the presence of the prosthesis during the early stages of secondary variability will help the child to select strategies with the prosthesis as very basic strategies. This line of thought suggests that the first prosthesis should be prescribed as early as possible, maybe even at six months of age. As such, the child will have the opportunity to develop an extended motor repertoire: motor functioning with and without a prosthesis. Ultimately, better motor skills should lead to more satisfaction and better functional use of the prosthesis and with that, to a lower rejection rate. Of course, we realize that we cannot yet prove the above-mentioned statements, but the results of our study are a first initiative towards a better understanding in how the development of the sensorimotor cortices can be a guide in the use of artificial limbs, especially in children with congenital unilateral upper limb deficiency. Preferably, the cortical changes should be visualized, for example, by using fMRI or PET scans. However, in young or very young study populations such research meets considerable ethical problems and for the moment we will have to restrict ourselves to indirect evaluation techniques like observations, functional tests or questionnaires.
Conclusion
Our results make clear that there is only little evidence available in literature concerning the preferential age the first prosthesis should be prescribed in children with a congenital deficiency of the upper limb. Until now the relation between the age of the first prescription of a prosthesis and rejection rates or functional outcomes in this patient category has not been investigated properly. As such, we may conclude that all currently used guidelines concerning prosthetic prescription procedures are experience-based instead of evidence-based. The high costs associated with the prescription of upper limb prostheses make this statement very interesting and is of societal relevancy. We recommend that a randomized controlled trial should be performed to answer questions regarding at what age prostheses should be prescribed in children with congenital upper limb deficiencies. However, we realize that such a design is not easy to carry out, since only small numbers of patients are available and the follow-up time should be of considerable length. This implies that there is a need for cooperation between national and international centres dealing with paediatric prosthetic management.