
Abstract
Background: Chronic low back pain (LBP) is a common secondary musculoskeletal problem among adults with cerebral palsy (CP). This study investigated the feasibility of incorporating backpack carriage with daily production activities for relieving chronic LBP among adults with CP.
Objectives: The effects of backpack carriage in relieving chronic LBP for adults with CP.
Study Design: A multiple bivariate approach with convenience sampling.
Methods: Nine adults with CP suffering from chronic LBP were scheduled to carry a 4 lb backpack at work for 60 minutes on weekdays for four consecutive weeks. The pain level was rated by the participants on an 11-point scale. Muscle activity of erector spinae was measured by surface electromyography.
Results: Significant improvement in back pain was found immediately after the backpack carriage with no adverse effect reported. It was accompanied with significantly reduced erector spinae activity. Although the overall change in pain ratings across the study period was not significant, a decreasing trend with time was observed.
Conclusions: The loaded backpack has the potential to serve as an ‘orthosis’ for immediate back pain relief among adults with CP. Its underlying mechanism can be attributed to a reduction in back muscle tension during the load carriage.
Clinical relevance
Results obtained from this study can be used to develop active training protocol in the management of chronic low back pain among adults with cerebral palsy.
Introduction
Chronic low back pain (LBP) is a common secondary musculoskeletal problem among adults with cerebral palsy (CP). It has been reported between 59% and 72.3% of adults with CP experience chronic LBP.1-3 The condition can be a lifetime problem and its mean duration varies from 13 months to 14 years.1,4
Studies on the aetiology and management of LBP in the CP population are limited and the findings inconclusive. Harada et al. 5 found that spastic diplegia with lumbar hyperlordosis were prone to develop LBP due to spondylolysis and spondylolisthesis. Their findings fall in line with an earlier claim that LBP in CP was related to hip flexion contractures. 6 However, in a prospective study of spondylolisthesis among ambulatory CP, Hennrikus et al. 7 concluded that hip flexion contractures did not predispose the group to spondylolisthesis or LBP. Excessive muscle actions that underlie their movement disorders may also contribute to the development of LBP in CP.8,9 With varied degrees of involvement and patterns of movement disorder variation, in terms of tissue tightness and bony deformities among different types of CP, was common. Thus, no single factor is the cause of the problem.
In physiotherapy, the patient is seldom a solely passive recipient of treatment. 10 A therapist may approach the LBP with passive or active therapy or both. In a survey on pain treatment for people with CP, it was reported that up to 72% of the respondents preferred passive types of intervention (e.g. medication, heat/cold pack, electrotherapy, etc.), rather than interventions requiring their active participation (e.g. biofeedback, therapeutic exercise, etc.). 11 This may be attributed to their difficulty in following the physical instructions involved in the active types of intervention. Gallien et al. 12 demonstrated that botulinum toxin injection into dystonic paraspinal muscles reduced LBP and lumbar hyperlordosis for adults with CP. In considering the potential side effects, non-pharmacologic therapy is more commonly adopted. The notion that an active approach may have adverse effects on patients with movement disorders and their ability to participate, a passive approach has become a treatment of choice for this population group. In a longitudinal study of treatments of CP-related chronic pain, Jensen et al. 11 pointed out that electrophysical treatment provided only short-term symptomatic relief for adults with CP. Active types of intervention are recommended in order to get to the root cause of the problem.
By comparing non-loading and light backpack loading in an upright posture, electromyography (EMG) studies on the erector spinae have consistently reported a lowered back muscle activity under the loading condition.13-15 Motmans et al. 16 found that the back muscle activity reduced during backpack carriage and it was accompanying with a forward trunk lean in the sagittal plane. In a non-loading upright situation, the upper body centre of mass is located in front of the lumbosacral joint and back muscle action is required to counterbalance the flexion moment generated by the upper body. In a backpack loading situation, the backward shift of the combined centre of mass of the trunk-and-backpack system changed the flexion moment to an extension one.13,16 Consequently, the trunk leaned forward so as to minimise the extension trunk moment during backpack carriage.17,18 Grimmer et al. 19 reported that this forward trunk lean was observed in case of backpack loading at 10% body weight (BW) or less. These findings helped to shape our understanding of the underlying mechanism and condition of backpack carriage in reducing back muscle activity.
In clinical applications, Kaplan and Sinaki 20 employed the principle of backpack carriage to develop a pain relieving spinal orthosis. Improvements in dynamic posture, back extensor strength, balance and gait, pain intensity and fall tendency were reported in patients with osteoporosis.21-23 A significant decrease in back muscle activity with 1-kg load carriage during standing and walking was also reported among elders with spinal deformities. 24 The reduced back muscle recruitment may contribute to back pain relief.22,24
Backpack is a common form of load carriage. It is a simple task that most patients with CP, from moderate to severe motor dysfunction, are capable of doing. The feasibility of incorporating backpack carriage with daily production activities in sheltered employment settings for relieving chronic LBP among adults with CP was investigated in this study. Our hypothesis was that by wearing a loaded backpack for definitive periods during working periods, adults with CP would experience less LBP compared to their normal pain levels during the working day.
Methods
A multiple bivariate approach with convenience sampling was employed. The effects of backpack carriage, while engaging in productive work, on the level of back pain and back muscle activity in adults with CP suffering from chronic LBP were evaluated. Written informed consent was obtained from participants who met the following inclusion criteria: (1) adults with CP at age 18 or above; (2) those who had suffered from LBP for at least three months; (3) those able to follow simple instructions; (4) those capable of sitting safely on a stool for at least one hour; and (5) those who had received no surgical intervention in past 12 months.
The experiment was conducted in sheltered workshops on weekdays for four consecutive weeks (i.e. a total of 20 sessions across 26 days). All participants were requested to carry a loaded backpack for 60 minutes and worked as usual in their workshops. During backpack carriage, the participants were seated on a stool without back and arm supports at a height with feet flat on floor. Each participant rated their back pain level before and after the backpack carriage on every Monday, Tuesday and Wednesday throughout the four-week period (i.e. a total of 12 pain-rated sessions on Days 1–3, 8–10, 15–17 and 22–24). Muscle activity of erector spinae at the L3–4 level was measured before and after the 60-minute backpack carriage at one of the experimental sessions.
A two-strap backpack (Junior 13, Podia Adventure, Hong Kong) with removable sandbags was used (Figure 1). A load of 4 lb (~1.82 kg) was used based on the findings of a pilot study on two adults with CP who suffered from chronic LBP. To attain the lowest energy cost, previous studies recommended a backload positioning as close as possible to the centre of body mass.15,25 In addition to keeping the backload close to the centre of body mass, the strap length was adjusted to ensure that it did not touch the stool while the study participant was seated and the surface electrodes were not pressed while capturing EMG signals.
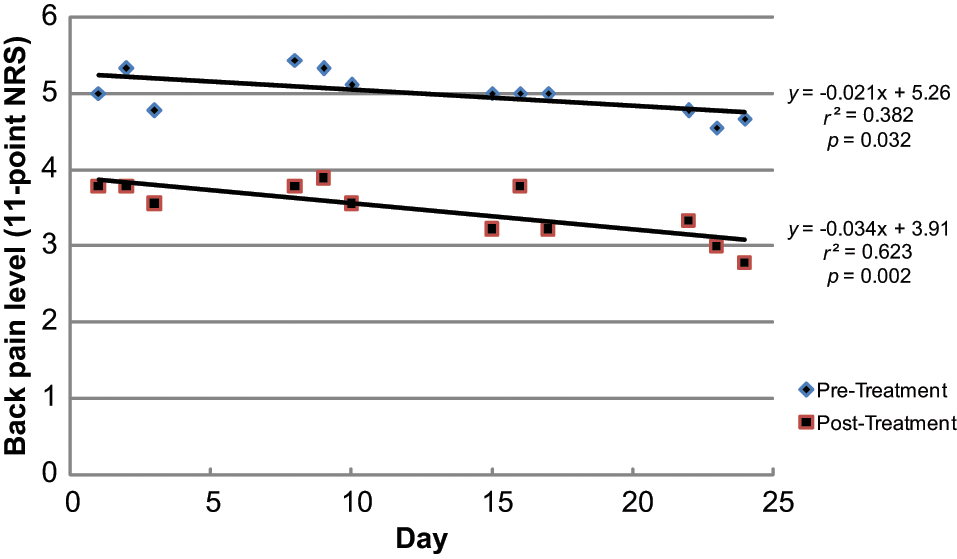
Average back pain levels, rated on an 11-point numerical rating scale (NRS), of the nine participants before and immediately after backpack carriage at the 12 pain-rated experimental sessions. A significant trend of decreasing back pain (p < 0.05) was observed across the four-week (26-day) course of backpack carriage.
An 11-point (0–10) numerical rating scale (NRS) was used to evaluate the participant’s subjective perception of the intensity of their back pain. Point ‘0’ indicated no pain while point ‘10’ indicated the worst possible pain. 1 Two sets of pain rating were collected at each pain-rated experimental session. The first set was captured immediately before the backpack carriage and the second was captured immediately after the backpack removal.
EMG data were taken from three positions: lying prone, sitting upright and sitting upright with backpack carriage. Surface EMG electrodes were placed at the L3–4 level over the muscle bulk of left erector spinae. A reference electrode was attached to a bony landmark. The EMG signals were acquired via an A/D converter at 3 kHz for 30 s. A fourth order Butterworth bandpass filter (30–400 Hz) was used to filter out the high frequency noise as well as the EMG signals. A root mean square (RMS) filter, every 100 ms, was used to process the output signals and the average RMS of the EMG activity was determined for each measurement. Nine sets of EMG data were obtained from each participant. The first and second sets were taken while the participant was lying in a prone position and sitting upright respectively with the latter as the baseline measurement. The remaining seven sets were taken at 0, 15, 30, 45 and 60 minutes of the backpack carriage, and at 5 and 20 minutes after the removal of the backpack. The EMG data relative to those with participants in a prone lying position were used for comparisons.
Pooled results of all participants on changes in back pain ratings before and after backpack carriage (i.e. ‘treatment’ factor with two levels: ‘pre’ and ‘post’) and across the 12 pain-rated sessions (i.e. ‘time’ factor with 12 levels: ‘Days 1–3, 8–10, 15–17 and 22–24’) were tested by two-way repeated measures analysis of variance (ANOVA). Pooled results of the participants on changes of the relative RMS EMG of erector spinae across the eight data sets in a single experimental session were tested by one-way repeated measures ANOVA. Data analysis was performed using a statistical package (PASW Statistics 18, SPSS Inc., Chicago IL) with level of significance set at 0.05.
Results
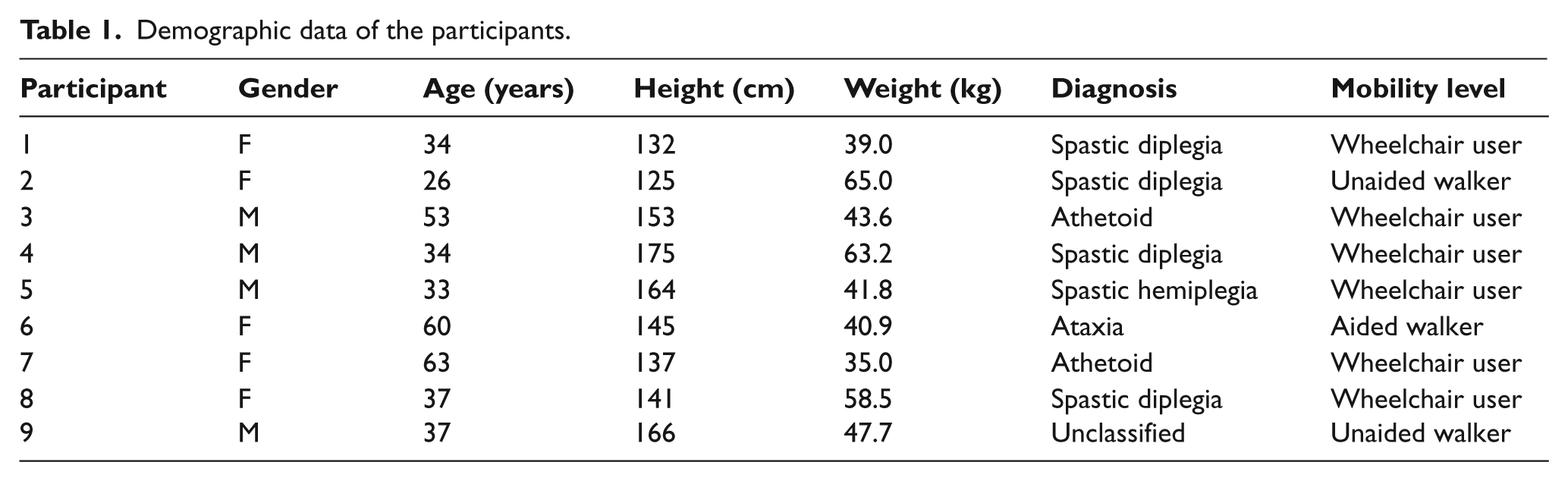
Nine subjects (four males and five females) with a mean age of 42 (range: 26 to 63 years old) were recruited from four sheltered workshops. Demographic data of the participants are shown in Table 1.
Demographic data of the participants.
Back pain
Pre- and post-load carriage pain ratings of the nine participants across the 12 pain-rated sessions were pooled together for data analysis. The average back pain level immediately after removing the backpack was found to be significantly lower than that before carrying the backpack (p < 0.05) (Figure 1). However, the pain returned at the next experimental session. On examining the changes in pain level over the four-week (26-day) study period, a significant trend of decreasing back pain ratings was observed both immediately before (r2 = 0.38, p < 0.05) and immediately after (r2 = 0.62, p < 0.01) the backpack carriage (Figure 1). However, the overall change in back pain level over the 26 days of intervention was not statistically significant.
Muscle activity on erector spinae
To allow inter-participant comparison, relative RMS values of the EMG signals obtained from a seated position with respect to that from prone lying were determined. One participant (participant 5) opted out of the EMG study due to other health reasons. Results from the remaining eight participants were pooled together and comparisons among the eight sets of relative RMS EMG taken before, during and after the backpack carriage were made by one-way repeated measures ANOVA. Contrast analysis was performed to evaluate the changes in the relative RMS EMG signal at different time points in comparison with that of the initial baseline measurement (i.e. initial unloaded upright sitting posture) with level of significance at 0.05. Results of contrast analysis revealed a significant decrease in the relative RMS EMG of erector spinae (p < 0.05) at the five data sets captured while the participants were carrying the backpack (Figure 2). No significant difference was observed at the EMG activity after the removal of the backpack.
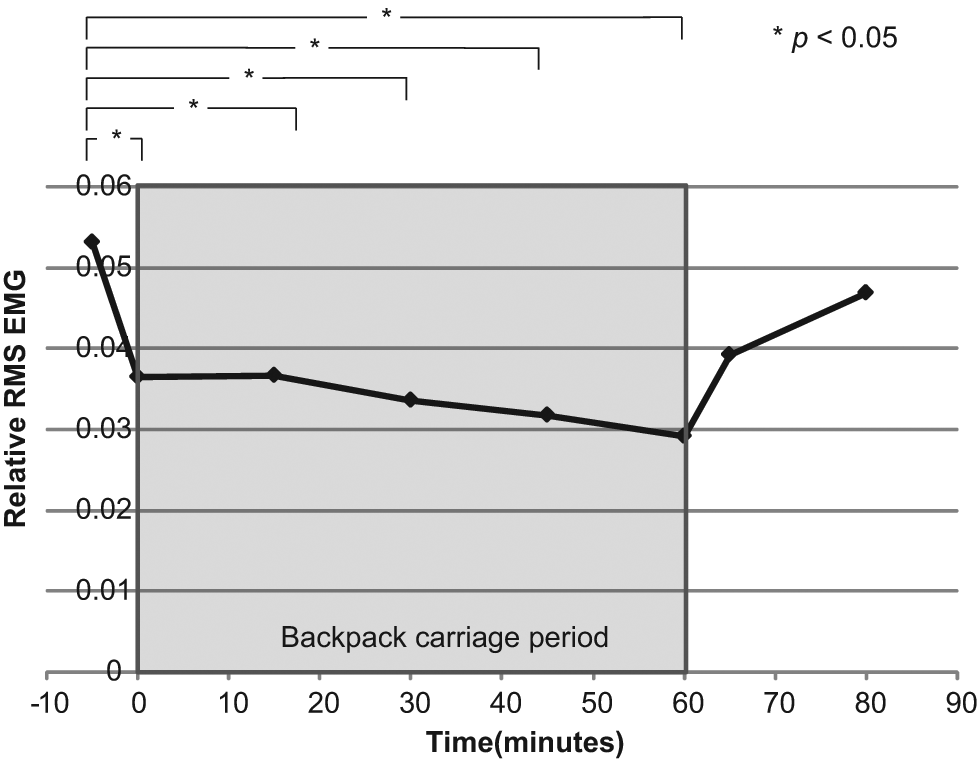
Average root mean square (RMS) electromyography of erector spinae of the eight participants relative to initial prone lying posture during (the shaded area) and after backpack carriage.
Discussion
For non-disabled people, a forward trunk lean with reduced back muscle activity was observed when carrying a posterior loading of 10% BW or less. 19 With tissue tightness, body deformities and movement disorders among adults with CP, carrying a backpack at 10% BW may be too heavy. Findings from one of our pilot studies recommended a backpack carriage of 3 kg or less for adults with CP 26 ; another pilot study further limited the loading to 4 lb (~1.82kg) for participants with chronic LBP.
Kaplan and Sinaki 20 suggested load carriage enhances proprioceptive input for postural control. It was the increase in postural awareness which contributed to the back pain relief. In an attempt to investigate the underlying pain relief mechanism, Ishida et al. 24 found that back muscle activity reduced significantly when carrying a load of about 1 kg. All these studies were conducted on patients with osteoporosis or elders with lumbar kyphosis.
In the present study, the application of backpack carriage for back pain relief was extended to adults with CP. Participants with varying body build, structural deformities and movement disorders were recruited (Table 1). Our findings demonstrated an immediate and significant back pain relief (p < 0.05) while carrying the backpack by the participants with CP. The improvement in pain was accompanied with a significantly reduced activity of erector spinae (p < 0.05). The increase in back muscle activity once the backpack was removed reinforced the ‘orthotic’ role of backpack carriage in relieving LBP.
The mechanism of backpack carriage for reducing back muscle activity is unclear. In addition to the increased postural awareness, it is suggested that a backward shift of the combined centre of mass of the backpack and upper body may have a role. It was observed that sheltered workshop trainees with CP tend to lean forward while sitting at work. With the centre of mass shifts forward, back extensors will be called into action causing lower back stress. By wearing a properly loaded backpack, the external flexion moment will decrease with a reduced demand on the back muscle action. The present study did not investigate the postural changes during backpack carriage and further study in this area is recommended.
CP is a collective term used to describe a group of people with a range of postural and motor impairments that result from a non-progressive insult to the developing central nervous system. 27 With no control on the types of CP being recruited, the participants in this study were heterogeneous (Table 1). Due to their varying mobility levels, the experiment was conducted in a seated position. Further study on comparing the response of ambulant CPs to backpack carriage in different positions (e.g. standing) and activities (e.g. walking) is recommended. Moreover, in view of the significant trend of pain improvement over the four-week course of intervention, a longer follow-up period was indicated to ascertain any carryover or ‘therapeutic’ effects of the backpack carriage.
Although no adverse effect was reported during and after the backpack carriage period, tiredness was reported by six participants after carrying the backpack for an hour. Shoulder discomfort was reported by two participants upon completion of the last few experimental sessions. Similar findings were reported in previous studies.21,24 A standard carrying load of 4 lb was used for all participants in this study. Further research on balancing the back pain relief and shoulder complication on different types of CP is warranted.
The major limitation of this study was the small sample size due to a difficulty in recruiting participants suffering from chronic LBP with reasonably good cognitive functioning to respond to the 11-point NRS and with good sitting balance and tolerance. In this study, the EMG data were not normalised with the maximum voluntary contraction (MVC) of the erector spinae as it was difficult to perform the MVC test on the participants. An age range of 37 years among the participants might be a source of variation in muscle strength that might affect the EMG interpretation on the extent of muscle relaxation. Moreover, variation in sitting tolerance might affect the EMG results after prolonged sitting and loading. Further studies on the optimal weight of loading and length of carriage period for different types of CP and on the carryover of the pain relieving effect by extending the course of loading intervention to three months are recommended.
Conclusion
Load carriage, in the form of a backpack, is low cost and simple enough for adults with CP. The intervention can be incorporated into the work schedule of the carriers to promote their compliance by engaging them in productive activities while carrying the load. This study demonstrated the potential of employing a weighted backpack as an ‘orthosis’ for relieving chronic LBP among adults with CP. Further investigation on its underlying mechanism as well as the optimisation in weight of loading and duration of carriage on an individual basis are indicated and a longer follow-up study is needed to ascertain whether its therapeutic effect on LBP is warranted.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.