
Abstract
Study Design:
Prospective, concurrent-cohort study.
Objectives:
To determine the effects of volitional preemptive abdominal contraction (VPAC) on trunk control during an asymmetric lift in patients with recurrent low back pain (rLBP) and compare with matched controls.
Methods:
Thirty-two rLBP patients and 37 healthy controls performed asymmetric lifting with and without VPAC. Trunk, pelvis, and hip biomechanical along with neuromuscular activity parameters were obtained using 3-dimensional motion capture and electromyography system. Hypotheses were tested using analysis of variance.
Results:
The VPAC resulted in significantly reduced muscle activity across all trunk extensor muscles in both groups (M ± SD, 6.4% ± 8.2% of maximum contraction; P ≤ .005), and reduced trunk side flexion (1.4° ± 5.1° smaller; P ≤ .005) and hip abduction (8.1° ± 21.1° smaller; P ≤ .003). rLBP patients exhibited reduced muscle activity in external oblique (12.3% ± 5.5% of maximum contraction; P ≤ .012), as well as decreased hip flexion (4.7°, P ≤ .008) and hip abduction (5.2°, P ≤ .001) at the final position of lifting in comparison with healthy controls.
Conclusions:
The results of this study defend the recommendation that the use of a VPAC increase spine stability during an asymmetrical loading task. Our results provide an indication that a VPAC strategy that is achieved during an asymmetric lifting decreases exposure for lumbar spine injury and instability. Spine care providers and ergonomists can use this information when designing neuromuscular control training programs, both for healthy individuals aimed at prevention of injury, as well as those with a history of rLBP, aimed at full functional recovery and protection from future injury.
Keywords
Introduction
Low back pain (LBP) is the main cause of disability worldwide with 540 million individuals experiencing unilateral or bilateral symptoms between T12 and the mid-thigh for one or more episode over their life span. 1 LBP occurs across all ages, is highly linked to disability, and represents a serious burden on health care providers. 2 The etiology of LBP is often multifaceted and is typically hard to link to specific, individual pathologies. Potential nociceptive contributors to LBP may include the intervertebral disc, facet joints, vertebral endplates, the vertebral ligaments, tendons, and muscle pain. 3,4 Deficiencies in low back musculature size, integrity, and motor coordination have also been linked to LBP. 5 -9 Persistent LBP has been linked to core trunk and low back muscle weakening, which can result in motor control deficiencies and asymmetries. 10 -12 Over time, these imbalances can affect patients abilities to stand, walk, lifting, and or prolonged periods of sitting or standing naturally, and in turn, may become a self-perpetuating driver of LBP itself. 12 -17 Biomechanical research suggests that patients with recurrent LBP (rLBP) lack adequate spinal stabilizing contractions and may also demonstrate impaired postural control, delayed muscle reflex latencies, and abnormalities in trunk muscle recruitment patterns. 18,19
Asymmetric lifting is a known risk factor for low back disorders, 15 -17,20 and such repeated loading places the patients at a higher risk for injuries to the lumbar spine and lower extremity. 21 Often, patients are required to manage materials while performing lifting tasks in restricted areas in various body positions. 21 -24 Such common lifting scenarios are encountered repeatedly in healthcare, 25,26 farm animal management, 27 physically heavy and monotonous work, 28 and performing arts. 29 A typically slouched posture during lifting sequences is often accentuated when returning to an upright position with the load, 30 which increases the compressive forces between the lumbar vertebrae. 31 Moreover, the shear forces on the lumbar intervertebral discs are increased when lifting from that slouched position. 31 All too often, vocational lifting is asymmetric, 15,32 which is associated with decreased trunk strength, a reduction in the maximum acceptable weight of the lift, and more complex trunk motion. 15,22,32 Normal lumbar spinal segments in individuals without LBP appear to be tolerant of a 700- and1000-N shear force during repetitive versus occasional shear exposures, respectively. 14 However, repeated lifting in a slouched posture increases those shear forces during manually demanding activities, especially when the patient has a history of LBP. 22,27 Patients with LBP reportedly use naturally different lifting techniques to prevent pain exacerbation and damaged lumbar tissue overloading. 17
Several spine exercise protocols for LBP have been proposed with conflict in outcomes. 33 -36 The abdominal bracing maneuver is one form of volitional preemptive abdominal contraction (VPAC) that produces activity in both the abdominal and spine muscles. 37,38 The VPAC is commonly employed to improve lumbar spine stabilization and reduce pelvic motion in patients with spinal dysfunction. 21,39,40 Moreover, the VPAC induces deeper abdominal muscle activity, which works to stabilize the spine. 41,42 This trunk muscle recruitment is necessary in order to control trunk momentum and increase intra-abdominal pressure, which can improve spine stabilization. 43,44 The VPAC can serve as a protective measure during extremity movement. 21,42 This stabilization strategy can help prevent back injury or, in the event of existing LBP, can contribute to rehabilitation. 38 It has been previously investigated during landing and lifting maneuvers, with conflicting results regarding trunk control and the ability to reduce injury risk. 21,39,40,45 The effect of spine stabilization on patients with rLBP is well documented. 39,40,43 rLBP and asymmetric lifting have both been established in the literature as significant predictors for a low back disorder. 15,39 However, there is limited literature on whether spine stabilization strategies can increase spine stability and trunk control and decrease the risk of injury during asymmetric lifting in patients with rLBP. Therefore, the purpose of this study was to determine the effects of VPAC and rLBP on trunk mechanics and neuromuscular control during an asymmetrical 1-m box-lift task. Our findings can further the understanding of the complex interactions between spine stability, the lifting response, and the risk of development and recurrence of LBP.
Methods
Design
In this controlled laboratory study, a mixed 2-factor design was used to determine the effects of rLBP (rLBP vs healthy control) and abdominal contraction condition (VPAC vs no VPAC) on neuromuscular control and 3-dimensional (3D) spine and pelvis joint kinematics in a group of patients with rLBP compared with a group of healthy individuals during asymmetric lifting. The within-subjects factors were abdominal contraction condition, and the independent factor was a subject group. The sample size needed in this study to approach 80% statistical power was estimated from the data of previous literature that examined lifting. 24,40 A large effect size index of f = 0.40 was estimated. With the desired power of 80% (1 − β = 0.80) and desired α = 0.05, this effect size index would require a minimum sample size of 26 per group. 46
Subjects
All participants read and signed an informed consent form approved by the institutional review board for the protection of human subjects at the affiliated university. The study was approved by the Institutional Review Board for the Protection of Human Subjects at Texas Tech University (IRB#:504 051). Thirty-seven healthy individuals and 32 rLBP patients participated in the study (Table 1). All subjects were between the ages of 18 and 35 years. Volunteers were excluded if they had a history of knee pain, surgery to the knee or lumbar spine, active abdominal or gastrointestinal conditions, body mass index >30 kg/m2 or pregnancy, all documented by self-report. An additional inclusion criterion for the rLBP group was a history of rLBP that was intermittent, unilateral or bilateral symptoms between T12 and the mid-thigh. Subjects were to have experienced these symptoms for one or more episode over the previous 18 months. Subjects were to have experienced one or more of the following: (1) a severity sufficient to require medical or allied health intervention and/or (2) a severity sufficient to impair the subject’s ability to perform their normal activities of daily living. At the time of testing, subjects were to be in a period of remission from their LBP symptoms. 47
Anthropometrics Data.
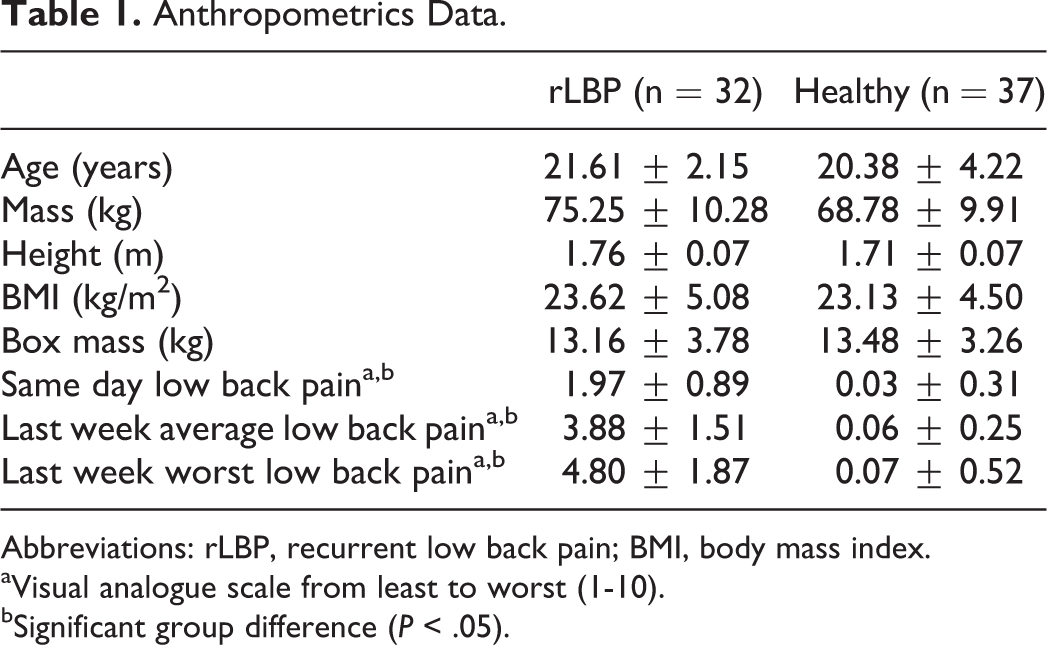
Abbreviations: rLBP, recurrent low back pain; BMI, body mass index.
aVisual analogue scale from least to worst (1-10).
bSignificant group difference (P < .05).
Data Collection Procedures
Subjects filled out a visual analog scale pain to indicate if they were experiencing any LBP (Table 1). The subjects were taught how to perform the VPAC when they were instructed to place their first webspace of each hand over the respective iliac crest. Once placed, the subject was then asked to “make their lower trunk wider” while continuing with diaphragmatic respiration. 18 The subjects were then taught how to perform the protocol of asymmetric lifting to the right. Lifting technique was based on the discretion of the individual and the subject’s box weight was determined by their maximum psychophysically acceptable weight (Table 1). 21,22 Participants performed 3 weighted box (0.65 m long, 0.35 m wide, and 0.15 m high) lifting trials with VPAC and 3 trials without VPAC to a 1 m high table in right side directions (Figures 1 and 2). The VPAC condition was presented in random order.
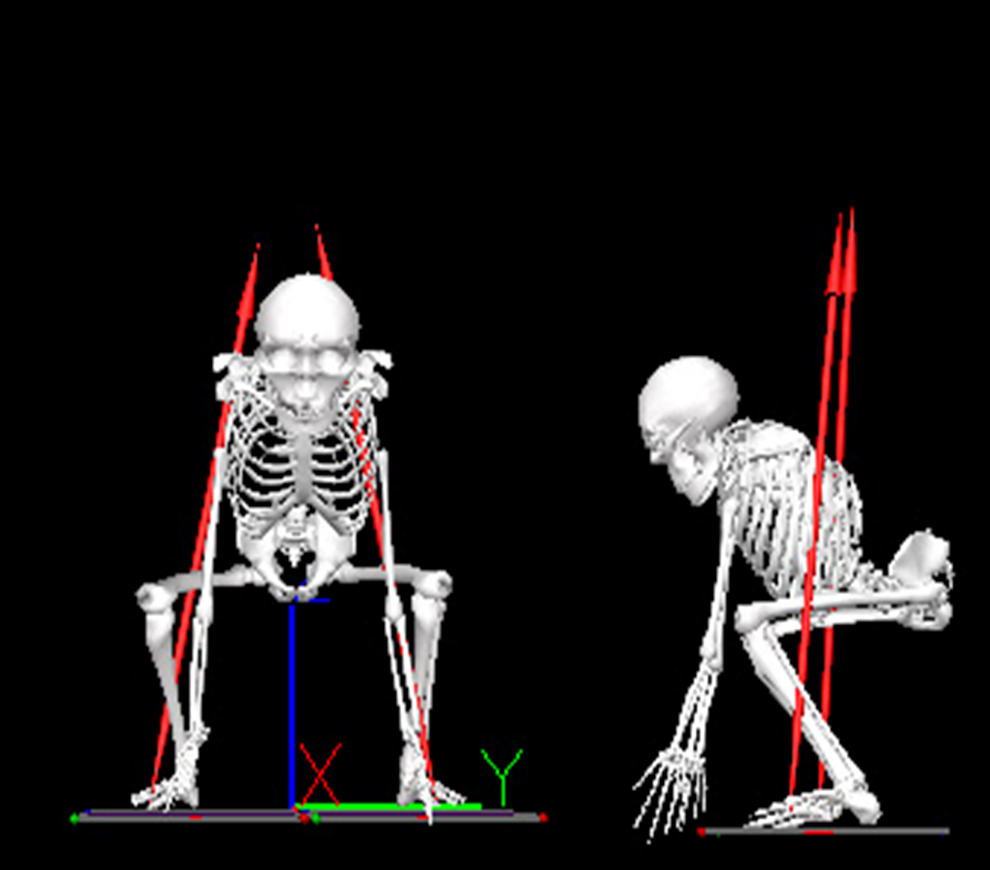
Initial position of 1-m asymmetric lifting.
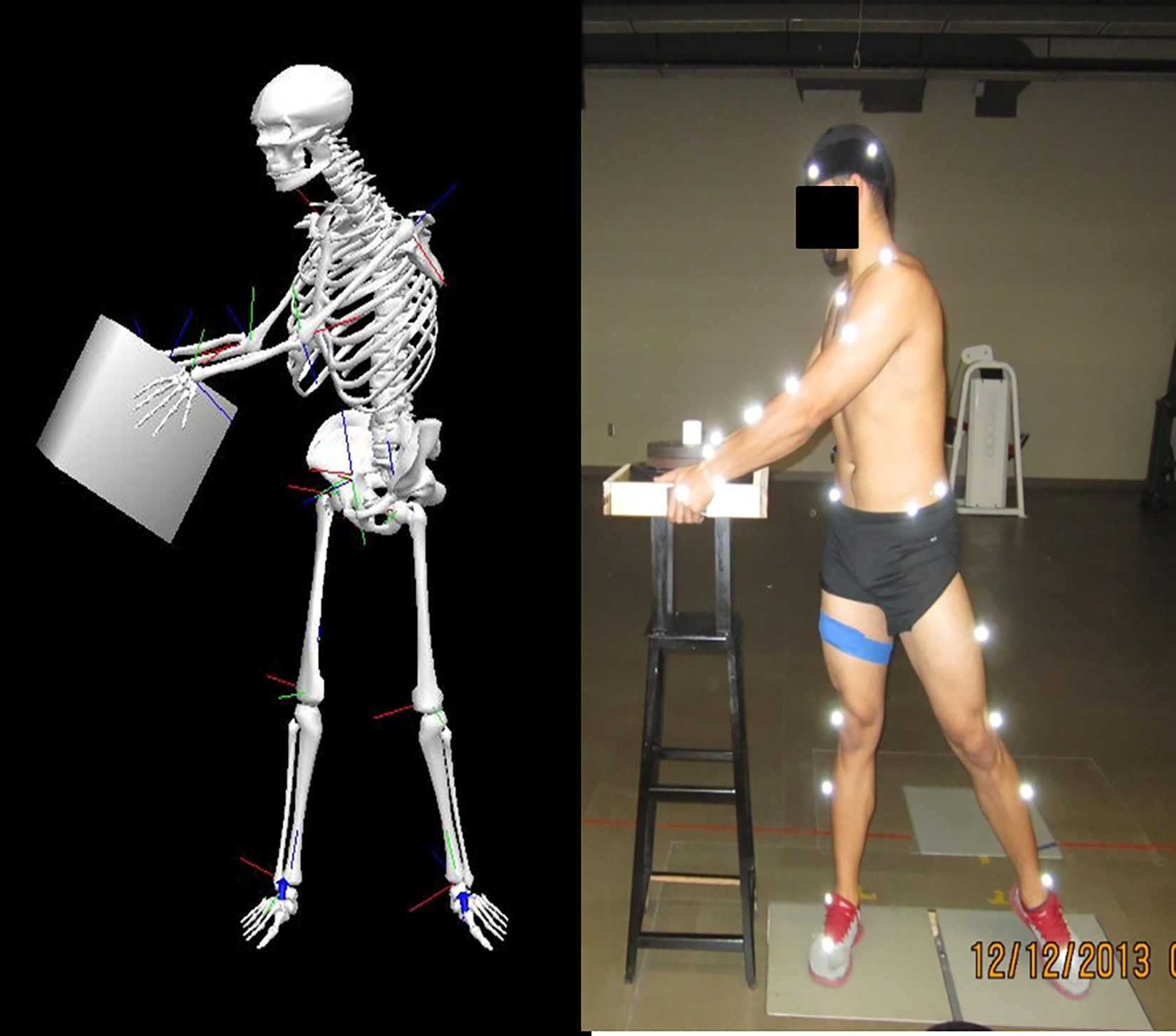
Final position of 1-m asymmetric lifting.
Electromyography (EMG) data from the right external oblique (EO), erector spinae (ES), and multifidus (Mf) at the fifth lumbar (L5) spinal level, and gluteus maximus (GM) 48 were measured using preamplified surface electrodes (Delsys Inc, Boston, MA) at 2000 Hz. The EMG sensor signal bandwidth was 20 to 450 Hz with a 3 µV peak-to-peak baseline noise. The overall channel noise was less than 0.75 µV with a common-mode rejection ratio of less than 80 dB. Each EMG sensor had 4 contacts with 5 mm by 1 mm dimensions and each contact was made of 99.9% silver. The skin was cleaned with alcohol, shaved as necessary, and then lightly abraded to reduce impedance. Subjects then performed maximum voluntary contraction (MVC) tests for all muscles listed above. The MVC outcomes were used later to normalize subjects’ muscle activity during the lifting maneuver. EMG data, kinematic data and ground reaction force data were collected with each lifting trial.
Forty-seven reflective markers (0.9 cm diameter) were incorporated in order to collect 3D kinematics (VICON Nexus 1.7.1, Denver, CO) of the lower extremity and trunk at a sampling rate of 100 Hz (Figure 1). Raw 3D coordinates were smoothed using a fourth-order no-phase-shift Butterworth low-pass digital filter with a cutoff set to 6 Hz prior to export for further analysis. A static trial was then collected to note marker placement. Ground reaction forces (GRFs) were measured at 2000 Hz using 2 parallel force plates positioned side by side (AMTI, Watertown, MA).
Data Reduction
Dependent variables included 3D trunk, pelvic, and hip joint angle, and EMG linear envelop magnitude for lower extremity and trunk muscles. Kinematics and linear envelop variables were analyzed at 2 times at initial position—0.05 seconds after lifting was initiated (Figure 1) and again at final position–0.05 seconds before the subject placed the box on the table (Figure 2). Those times were chosen since the body is at a mechanical disadvantage for lifting at the initial position, and the load is far from the body center of mass which creates a substantial moment across the trunk at the final position. All raw data was exported from the Vicon Nexus system and imported into a custom Matlab program (Mathworks Inc, v7.10.0, Natick, MA) and Visual3D for processing.
Statistical Analyses
A 2 (group) × 2 (abdominal contraction) crossover mixed design analysis of variance (ANOVA) procedure (SPSS, Version 21.0; IBM, Inc, Armonk, NY) was used to determine the effects of VPAC on the selected kinematic and EMG variables during 1-m asymmetric lifting in a rLBP patients group compared to a healthy comparison group. The VPAC condition (with or without activation) was within-subjects factors and subject group (rLBP or healthy) was a between-subjects factor. Interaction was assessed first for each 2-factor ANOVA, followed by main effects, as appropriate. Significant interaction effects were further evaluated by examining simple (pairwise) effects. In addition, 1-way ANOVA was used to compare group anthropometric and pain data.
Results
In rLBP patients, as well as healthy controls, the performance of the VPAC altered joint kinematics and muscle activity during an asymmetric lift. There were no statistically significant differences between the rLBP patients and healthy controls with regard to age, height, weight, body mass index, and box weight (Table 1). As expected, there were statistically significant differences in pain level between the groups (Table 1).
Interaction Between Volitional Preemptive Abdominal Contraction and Groups
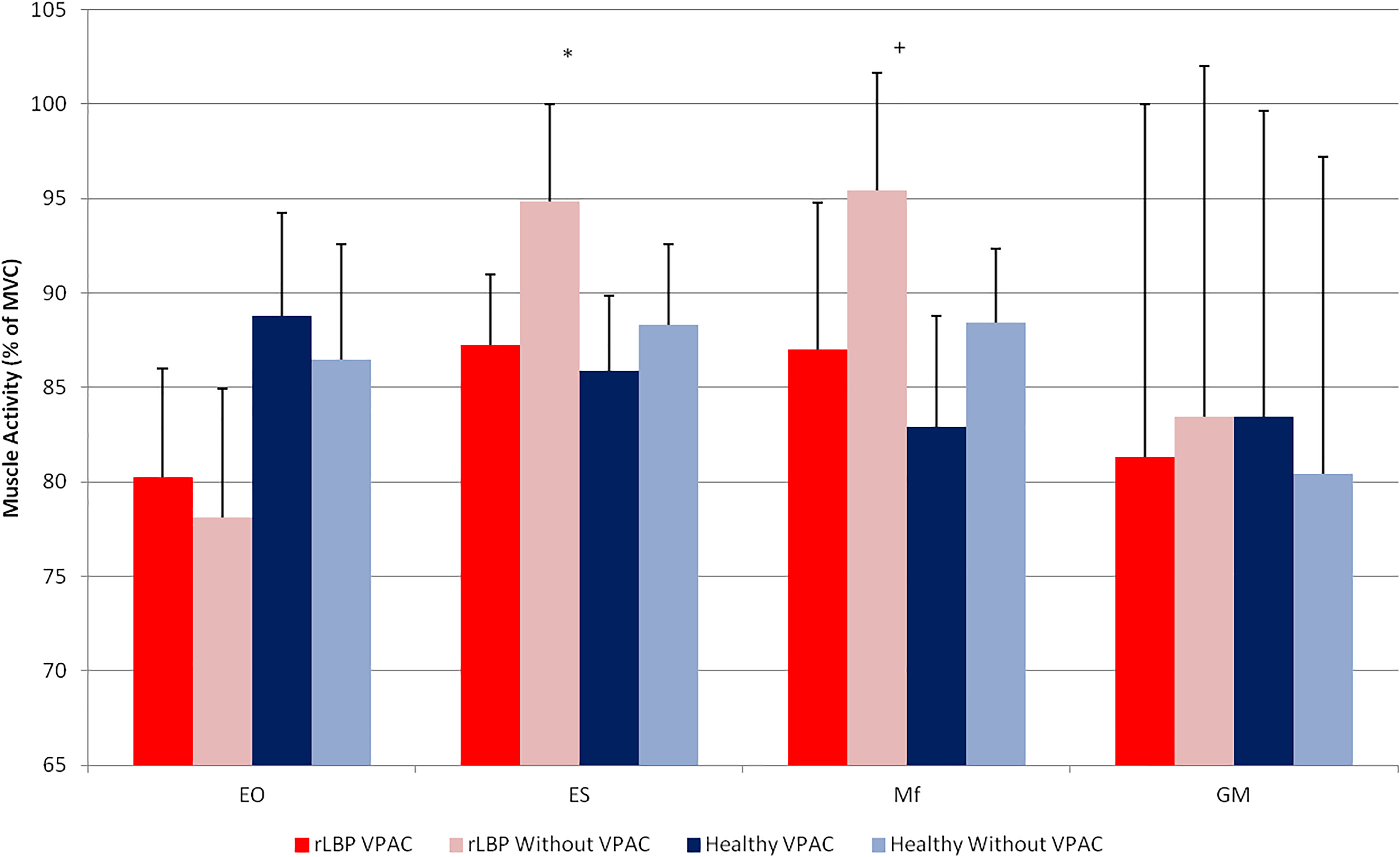
Tables 2 and 3 provide a summary of kinematics variables for each condition and group during the asymmetric lifting. Figures 3 and 4 provide a summary of neuromuscular activity parameters variables for each condition and group during the asymmetric lifting. Mf muscle activity in the initial position of the lifting exhibited a significant 2-way interaction effect in an asymmetric lifting (P = .011), when VPAC increase Mf activity in rLBP and decrease in healthy compare to the no-VPAC condition. Moreover, ES muscle activity (P = .047) and pelvis obliquity angle (P = .044) in the final position of the lifting exhibited a significant 2-way interaction effect in an asymmetric lifting as well.
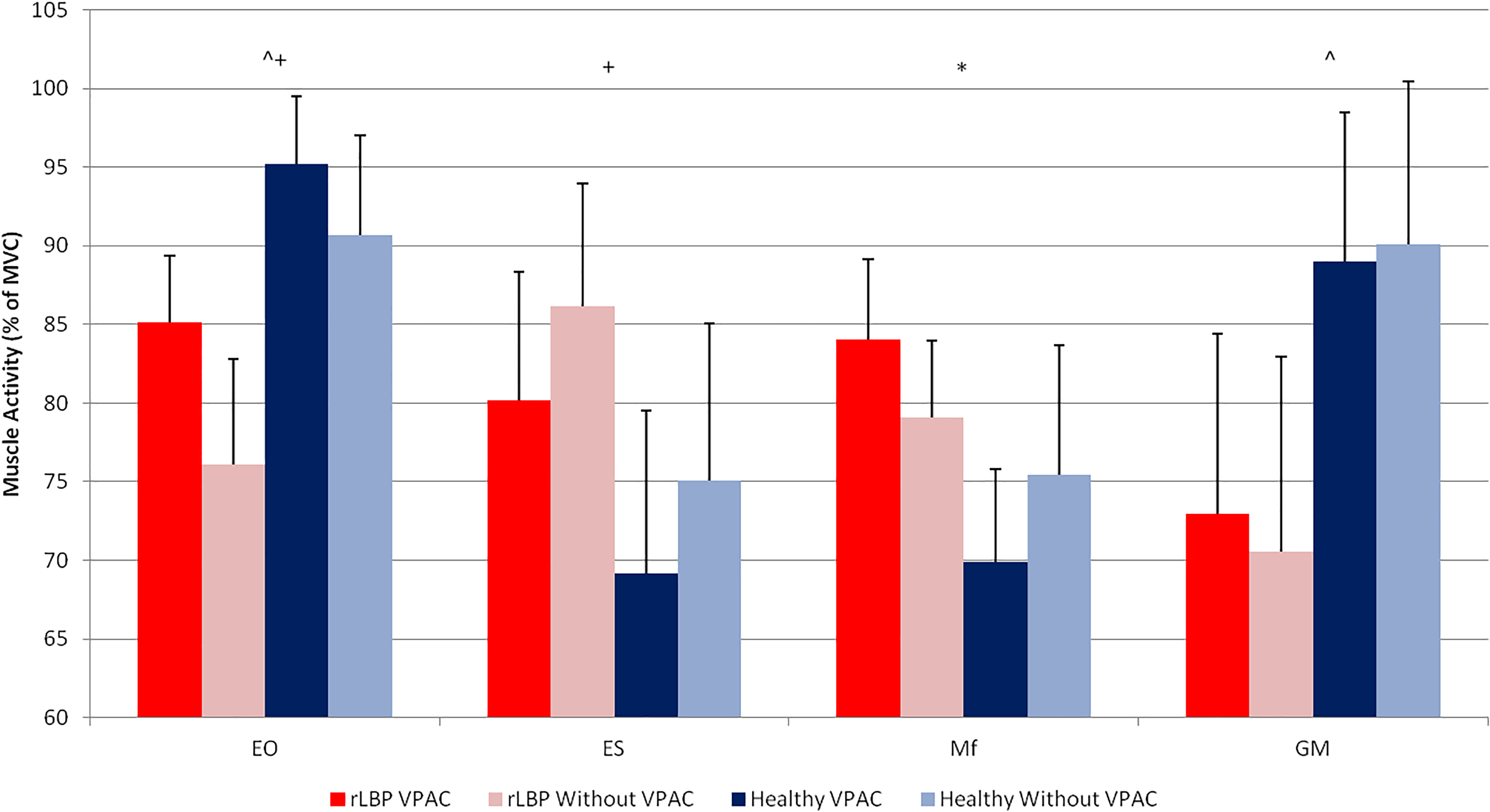
Electromyography variables during initial position in asymmetric 1-m lifting. EO, external oblique; ES, erector spinae, Mf, multifidus; GM, gluteus maximus; MVC, maximum voluntary contraction; VPAC, volitional preemptive abdominal contraction; rLPB, recurrent low back pain. *Two-way interaction (P < .05). +VPAC main effect (P < .05). ^Group main effect (P < .05).
Electromyography variables during final position in asymmetric 1-m lifting. EO, external oblique; ES, erector spinae; Mf, multifidus; GM, gluteus maximus; MVC, maximum voluntary contraction; VPAC, volitional preemptive abdominal contraction; rLBP, recurrent low back pain. *Two-way interaction (P < .05). +VPAC main effect (P < .05). ^Group main effect (P < .05).
Effects of Volitional Preemptive Abdominal Contraction
The VPAC altered trunk extensor muscle activity during the 1-m asymmetric lifting. Trunk muscle activity found to reduce with the performance of VPAC in ES (80.11% ± 9.00% of MVC without VPAC; 74.16% ± 9.38% of MVC with VPAC; P = .005) at the initial position of lifting, and in Mf (91.61% ± 7.07% of MVC without VPAC; 84.77% ± 7.66% of MVC with VPAC; P = .003) at the final position of lifting when data were collapsed across groups condition. Unsurprisingly, VPAC increased muscle activity in the EO (84.03% ± 6.79% of MVC without VPAC; 90.60% ± 4.30% of MVC with VPAC; P = .001) at the initial position of lifting when data was collapsed across groups condition. Volitional preemptive abdominal contraction had a little kinematic effect on the trunk and hip during asymmetric lifting. The VPAC significantly decreased trunk side flexion angle (−2.46° ± 4.73° without VPAC; −1.02° ± 5.47° with VPAC; P = .005), and hip abduction angle (29.60° ± 19.27° without VPAC; 21.54° ± 23.11° with VPAC; P = .003) at the initial position of lifting when data was collapsed across groups condition.
Recurrent Low Back Pain Versus Healthy Control
The rLBP group exhibited reduced EO and GM muscle activity compared with the healthy group. Recurrent LBP patients demonstrated reduced muscle activity in EO (92.94% ± 5.58% of MVC in healthy; 80.60% ± 5.49% of MVC in rLBP; P = .012) at the initial position of the lifting, when data was collapsed across core muscle activation condition. Furthermore, rLBP patients appeared to lift with smaller GM muscle activity at the initial position of lifting (P = .047). The healthy and rLBP groups exhibited minimal differences in hip kinematics during asymmetric lifting. The rLBP exhibited greater hip flexion angle (18.38° ± 7.53° in healthy;23.13° ± 8.44° in rLBP; P = .008), and smaller hip abduction angle (2.34° ± 6.10° in healthy;-2.90° ± 6.95° in rLBP; P = 0.001) at final position of lifting, when data was collapsed across core muscle activation condition.
Discussion
The purpose of this study was to determine the influence of VPAC and rLBP on trunk mechanics, as well as neuromuscular control, during an asymmetrical 1-m box-lift task. Our findings demonstrated that patients with rLBP exhibit differences in trunk neuromuscular control and spine kinematic during 1-m asymmetric lift. The rLBP group exhibited lesser EO and GM muscle activity and an increase in hip flexion angle and a decrease in hip abduction angle at the final position (Tables 2 and 3). The VPAC resulted in reduced Mf and ES muscle activity and increase in EO muscle activity, in both rLBP and healthy groups, and had minimal effects on pelvis and trunk kinematics during an asymmetrical lift (Tables 2 and 3).
Kinematic Variables During Initial Position in Asymmetric 1-m Lifting.a
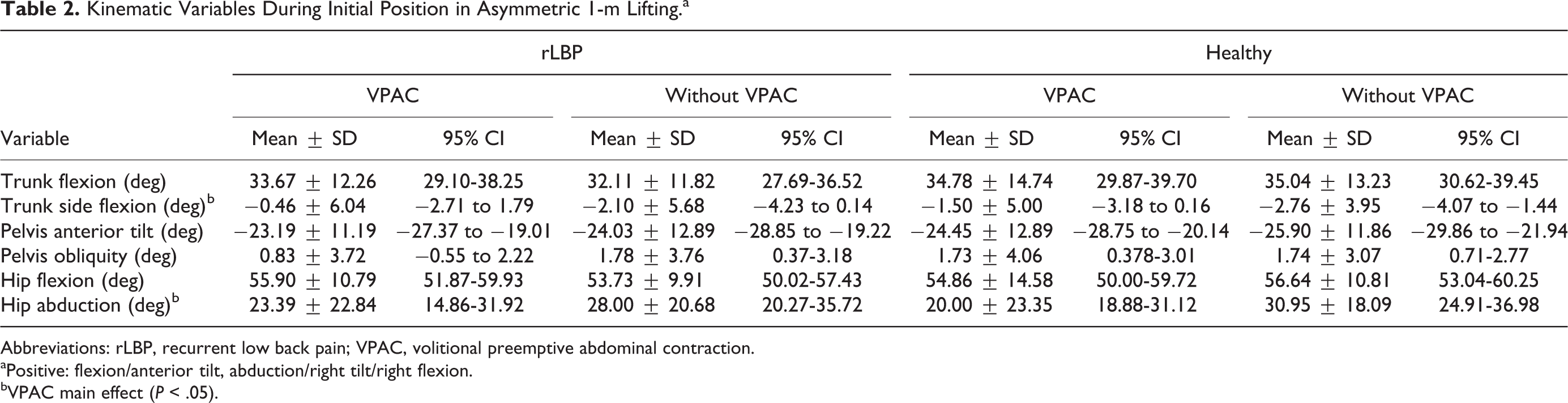
Abbreviations: rLBP, recurrent low back pain; VPAC, volitional preemptive abdominal contraction.
aPositive: flexion/anterior tilt, abduction/right tilt/right flexion.
bVPAC main effect (P < .05).
Kinematic Variables During Final Position in Asymmetric 1-m Lifting.a
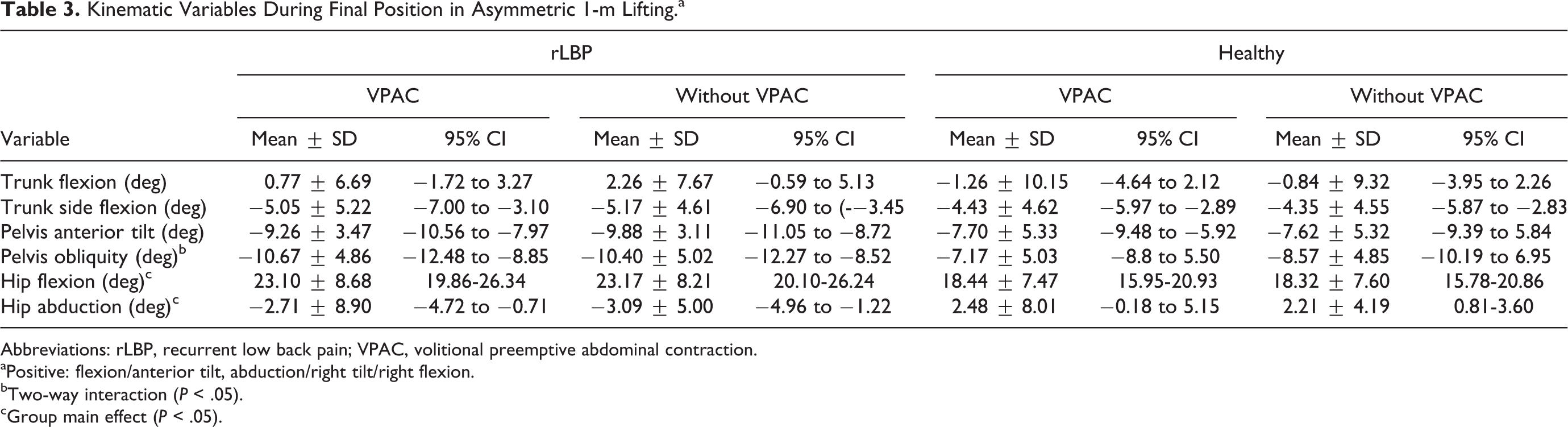
Abbreviations: rLBP, recurrent low back pain; VPAC, volitional preemptive abdominal contraction.
aPositive: flexion/anterior tilt, abduction/right tilt/right flexion.
bTwo-way interaction (P < .05).
cGroup main effect (P < .05).
Recurrent LBP patients have diminished trunk 49 and lower extremity strength, flexibility, and range of motion, 22,39,50 as well as altered neuromuscular control. 22,39,51 These patients presented with reduced activity in the EO and GM and increased activity in Mf in both initial and final position of lifting in comparison to healthy control. Laird et al 49 reviewed 43 studies on the lumbopelvic kinematics in LBP patients and found that these patients have reduced lumbar range of motion, move more slowly, and have reduced proprioception compared with people without LBP. Our study found that hip flexion and adduction were found to be higher at the final position of lifting in patients with rLBP, which can be explained by reduced GM muscle activity and by a different lifting style for people with rLBP in comparison with healthy subjects. 22
Predictably, the VPAC altered trunk neuromuscular control and kinematic during 1-m asymmetric lifting. As reported by Haddas and his group, trunk muscle function is altered in LBP sufferers. 21,22,39,52 Based on this study outcome, patients with rLBP may not be able to produce sufficient pelvic stability in order to provide a firm base for the trunk motion and control. The VPAC showed a significant effect on Mf and ES muscle activity in rLBP patients. Moreover, the VPAC causes a greater trunk side flexion angle in the final position of lifting which can be explained by the increased activity of the abdominal muscles and prepare for the asymmetric lifting. Furthermore, VPAC results in more hip adduction, which may potentially increase pelvic stability which is supported by previous studies. Increase in pelvis stability found to highly correlated with increased spine stability. 39,44 As part of a broad neuromuscular control training program, VPAC should be incorporated as a validated method for reducing injury in healthy individuals and those with rLBP.
As supported by ultrasound study, Nagar et al 40 also found increases in abdominal muscle activity during lifting. Our results agree with those of Nagar et al by virtue of the increased EO activity with the use of VPAC, which actively increases spine stability. A VPAC strategy using an abdominal bracing maneuver produces a global trunk muscle contraction, which includes the external and internal oblique muscles. 38 Oh et al 44 found that activation of the abdominal muscles significantly decreases the activity of the lumbar erector spinae muscles. Again, our results support this finding, VPAC reduced ES and Mf activity, which may potentially promote a reduction in the trunk flexion moment. Reduced lumbar spine extensor muscle activity could implement a more efficient lift. Increasing spine stability and alignment using VPAC may reduce trunk flexion load and reduce the need for the lumbar extensor muscles activity.
Although subjects in this study were trained on lifting techniques they were not assisted or guided in any way, and the subject’s box weight was determined by their maximum psychophysically acceptable weight. Our analysis focuses only on the subject’s right side, thus assuming symmetry between sides. Our data demonstrates large intersubject variability, therefore uncertainty around our estimates is a limitation that raises the risk of chance findings. Additionally, we acknowledge the limitations associated with the use of skin markers that may move during the lifting trials, as well as a potential system tracking error and data smoothing procedure error.
Conclusion
The results of this study defend the recommendation that the use of a VPAC increase spine stability during an asymmetrical loading task. Our results provide an indication that a VPAC strategy that is achieved during an asymmetric lifting decreases exposure for lumbar spine injury and instability. Spine care providers and ergonomists can use this information when designing neuromuscular control training programs, both for healthy individuals aimed at prevention of injury, as well as those with a history of rLBP, aimed at full functional recovery and protection from future injury. Such programs should focus on VPAC and other specific proven core muscle activation techniques in order to improve lower extremity and spine control and stability thus potentially decrease injury risk.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.